 |
Treating adult scoliosis is a challenge, as reducibility is low, back pain is frequent and bracing is poorly tolerated. However, in many cases it should be possible to avoid surgery.
|
 |
Fifty years ago, Lyon was one of the few cities treating adult scoliosis. Since that time this mission has been continued, and all patients treated have been integrated into a database computerised for more than 20 years. The treatment protocol has remained the same while integrating technological progress.
|
 |
All our patients are systematically called back for assessment every 5 years, to the great satisfaction of the treating doctors.
|
 |
In the same way, the technology of the brace and the high accuracy of the measurements have made it possible to generalise its use and to ensure that it is supported by the health services.
|
 |
For 200 years, the Lyon method has combined physiotherapy and mechanical means of correcting scoliotic curvature.
|
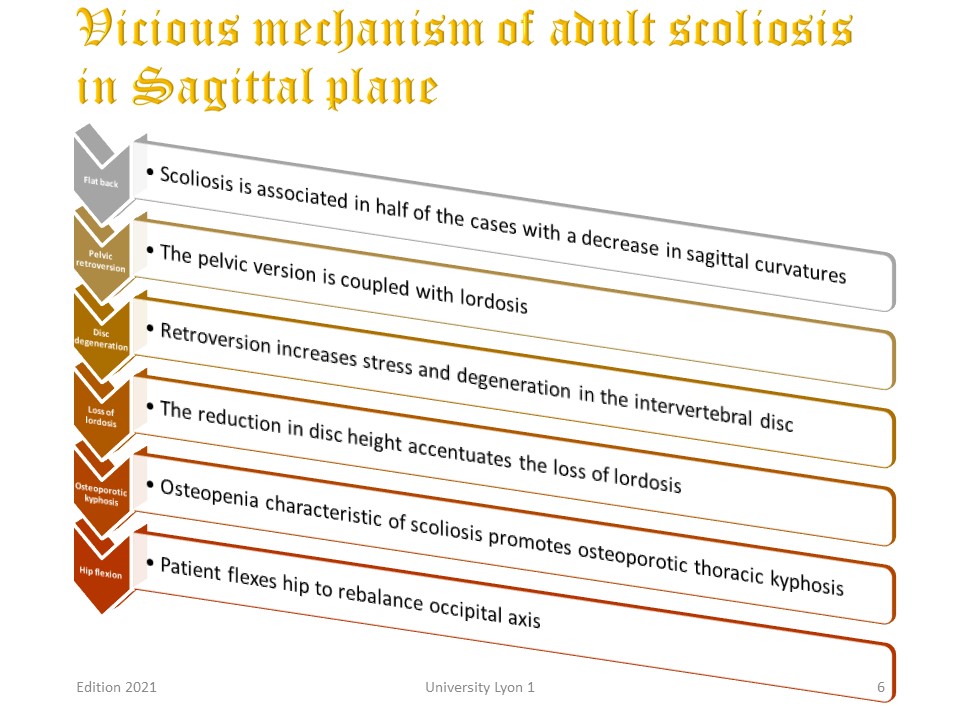 |
In addition to the regular accentuation in the frontal plane, there is a vicious mechanism of sagittal vertebral morphostatic which is important to know in order to provide the patient with indications of prevention.
Step 1: Scoliosis is associated in half of the cases with a significant flat back which can be accentuated by the brace.
Step 2: Pelvic and lumbar lordosis version are coupled. A decrease in lordosis is associated with pelvic retroversion.
Step 3: Pelvic retroversion increases the forward load on the intervertebral disc and promotes disc degeneration. The disc loses height.
Step 4: The reduced height of the intervertebral disc increases the loss of lumbar lordosis and promotes compensatory thoracic kyphosis.
Step 5: Osteoporosis also increases the high thoracic kyphosis.
Step 6 To rebalance the entire spine, the patient will flex the hips.
|
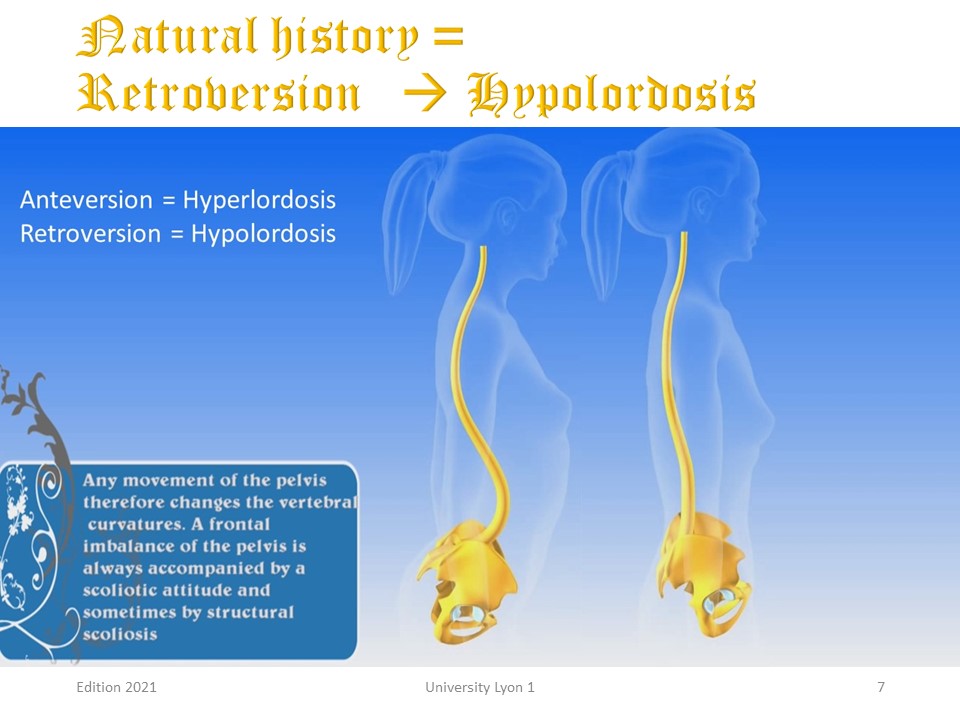 |
Each of these steps will be illustrated. Here we see the loss of lordosis associated with pelvic retroversion. For this reason, care should be taken with brace devices such as the Milwaukee brace and active axial self-elongation exercises.
|
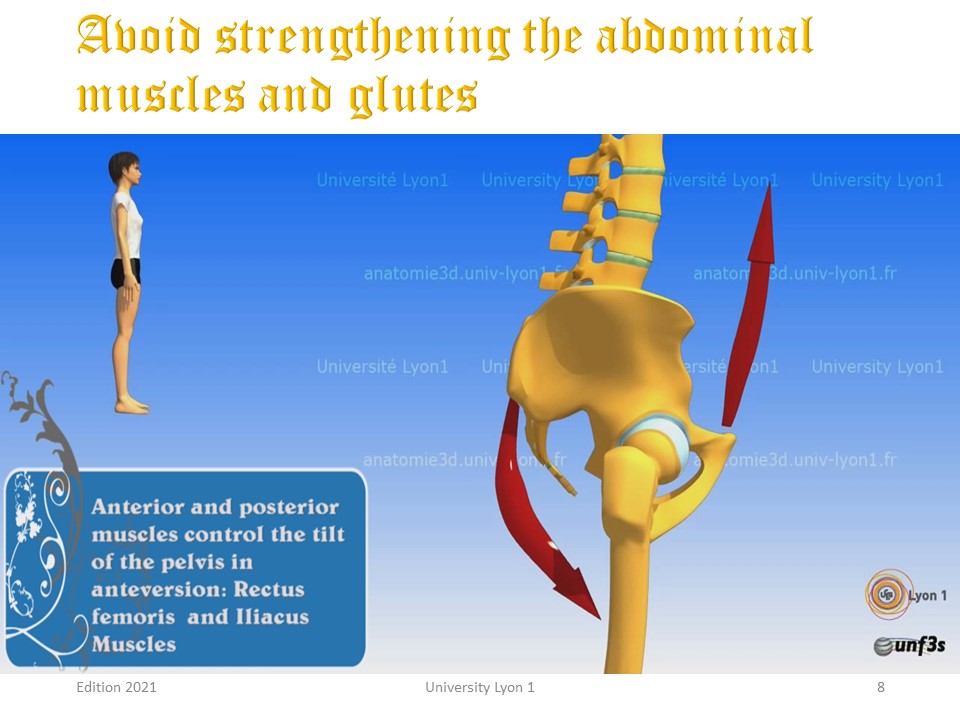 |
The majority of fitness exercises promote the strengthening of the gluteal and abdominal muscles, which in homo-sapiens have been one of the fundamental mechanisms of bipedalism. Unfortunately, their strengthening favours retroversion.
|
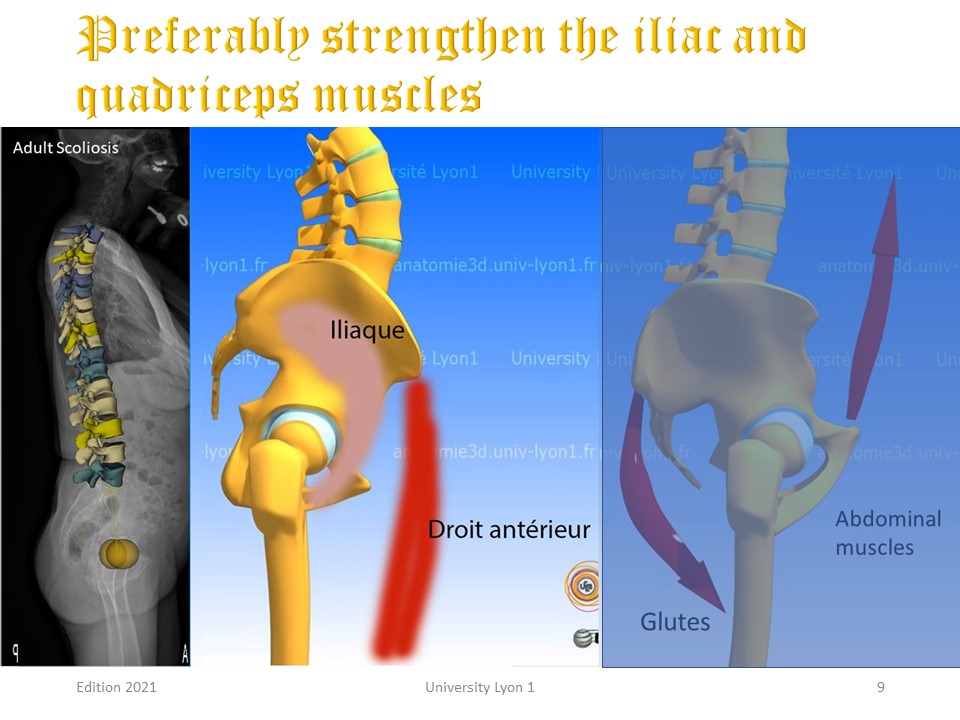 |
This is why in adult scoliosis with lumbar hypolordosis, it is preferable to strengthen the iliac psoas muscle and the rectus femoris.
|
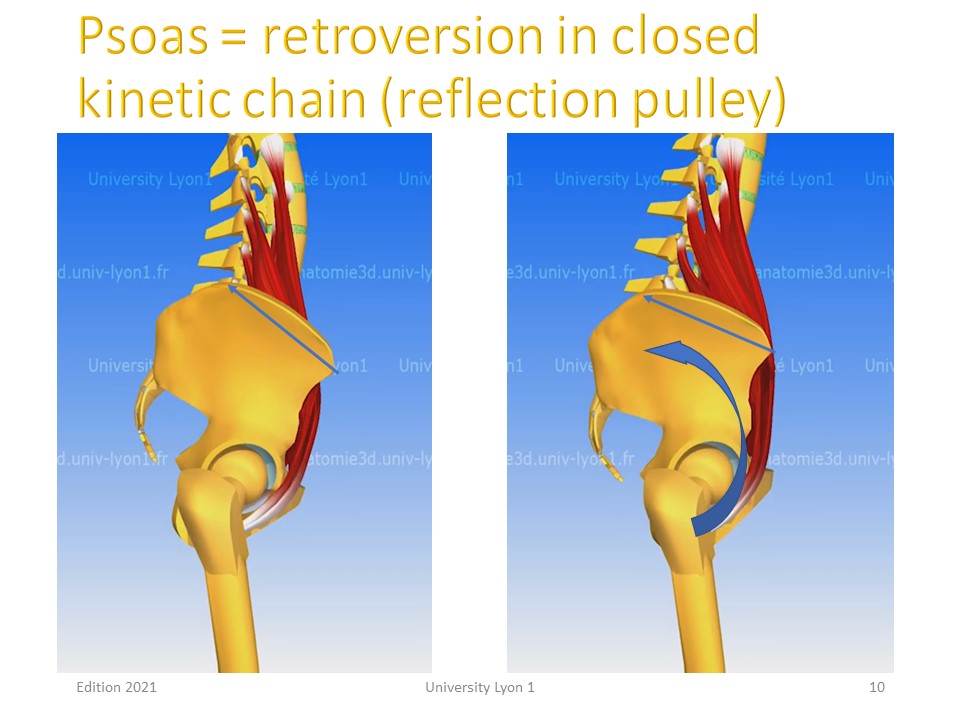 |
However, care must be taken to reinforce the iliac psoas in an open kinetic chain to avoid the retroversion effect on the reflection pulley of the inguinal fold.
|
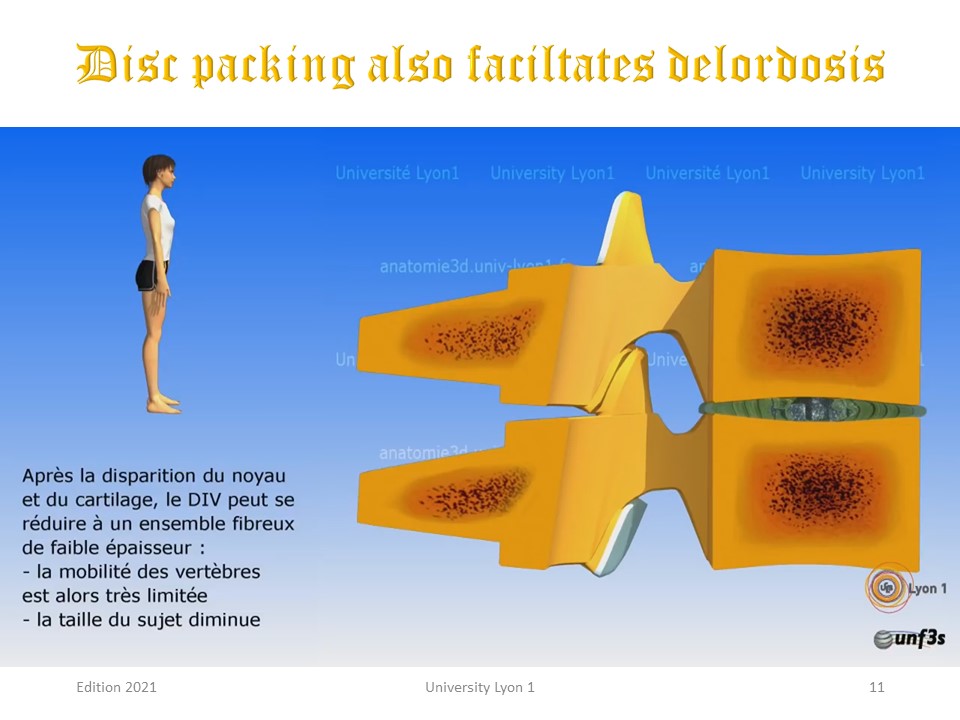 |
After the loss of the nucleus and cartilage, the intervertebral disc can be reduced to a thin fibrous assembly resulting in rigidity, hypolordosis, and a decrease in size with loss of tensegrity.
|
 |
Osteoporosis is physiological and results in a high thoracic vertebral cuneiformization, probably favoured by the sitting position and the anterior rolling of the shoulders.
|
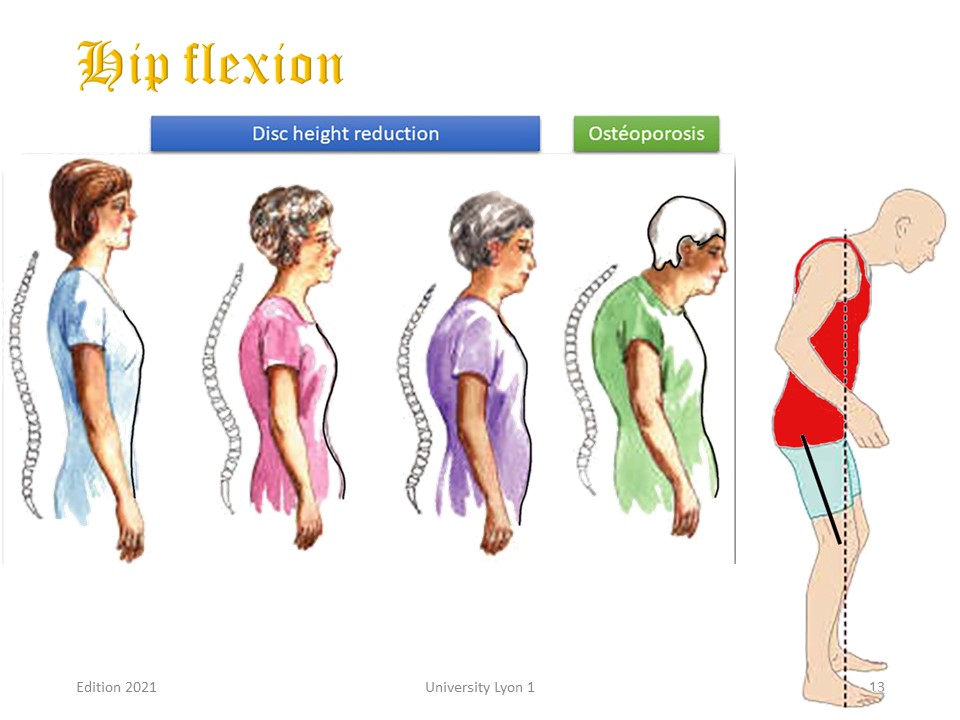 |
The last adaptation in the sagittal plane is the flexion of the hips to decrease the anterior projection of the line of gravity.
|
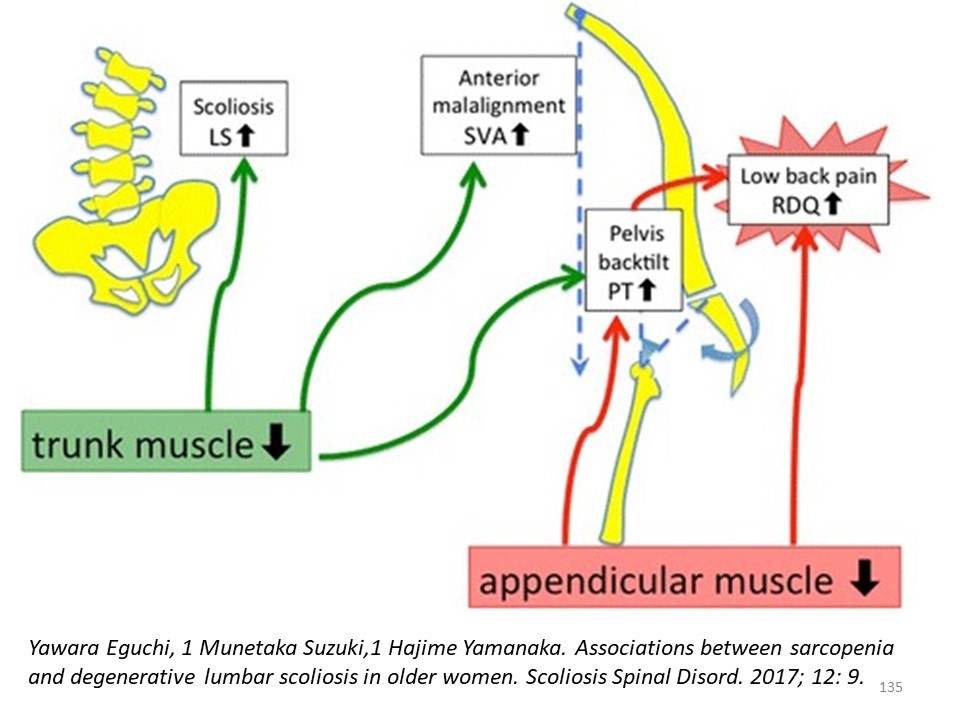 |
The pyramidal musculature with significant sarcopenia from the age of 40 also participates in this morphostatic evolution and does not succeed in slowing it down. This is why the strengthening of the pyramid muscles in aerobic metabolism must be associated in adult scoliosis with the strengthening of the extra-pyramid muscles.
|
 |
At the end of growth, it is important to give some indications of prevention to the patient.
|
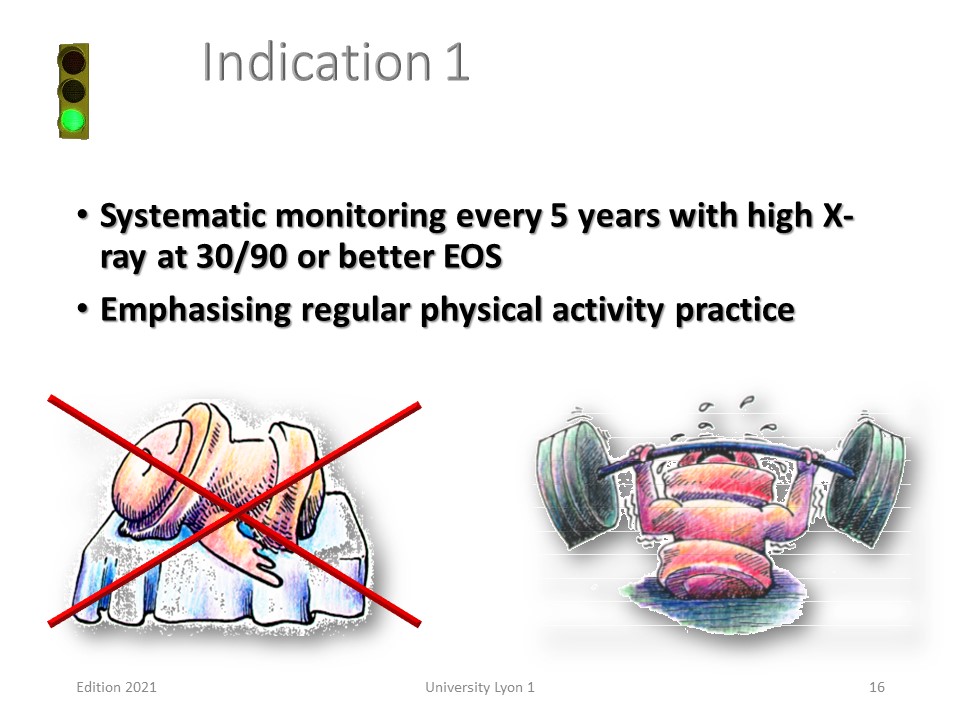 |
The first indication is to inform the patient of the evolutionary risk in adulthood. No evolution below 20°, average evolution of 0.5 % for an angulation between 30°-35° and 1° per year for a scoliosis of more than 40°. This evolution is very variable, it is therefore advisable to assess it by a systematic check-up every 5 years.
|
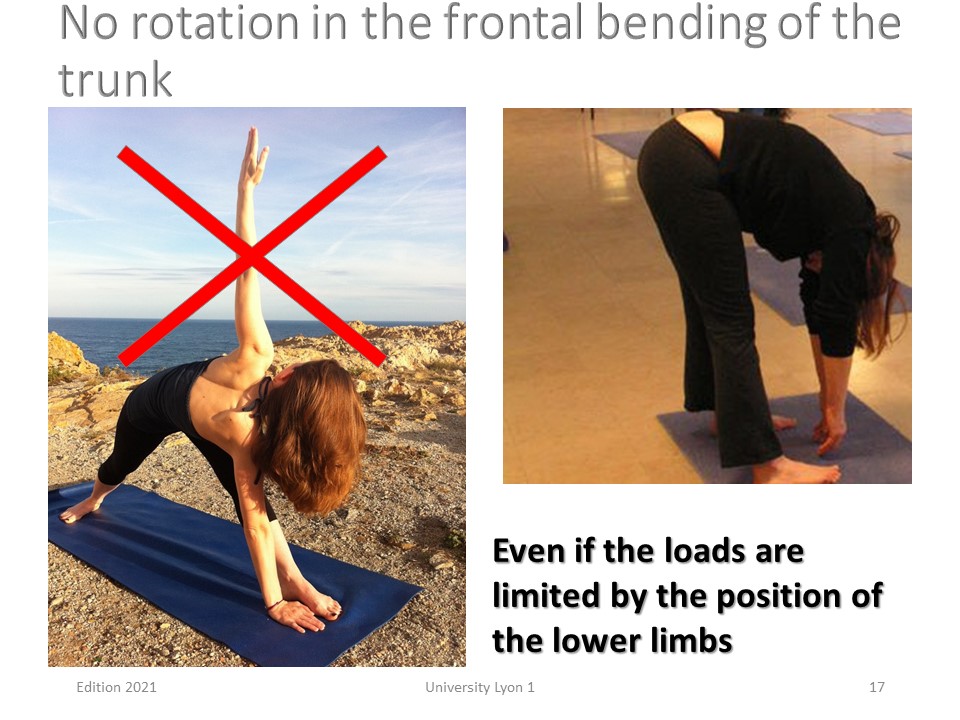 |
Forward bending of the trunk to pick up an object from the ground is usually done without bending the knees when not lifting a heavy load. On the other hand, any associated rotation of the trunk should be avoided, especially when the angulation exceeds 40°.
|
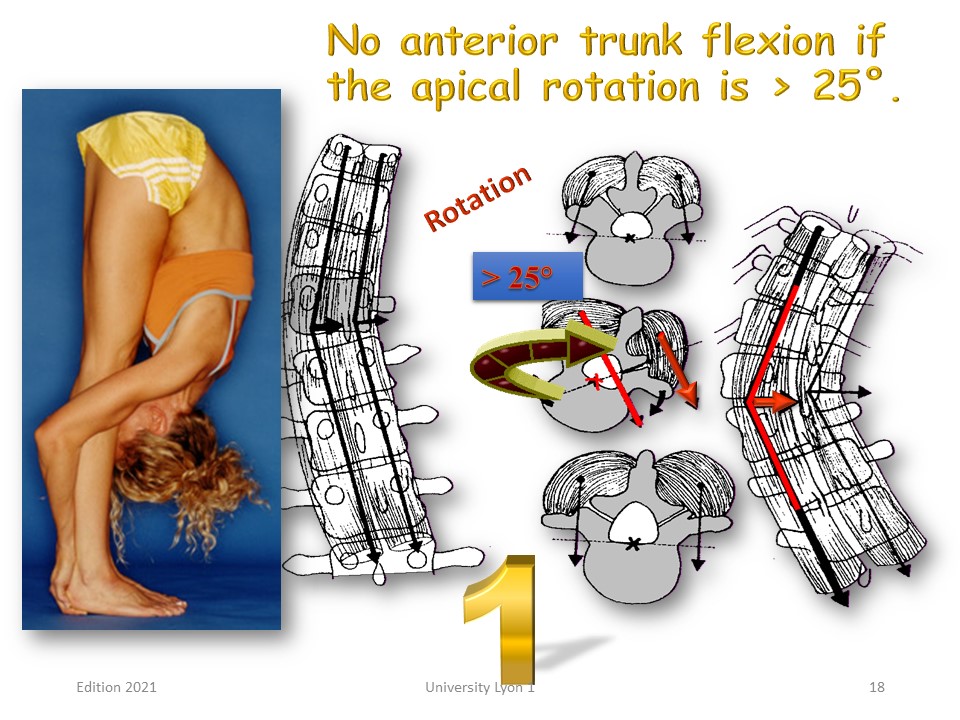 |
The anterior flexion movement of the trunk with little rotation is stable, as the concave and convex muscle lever arms are located on either side of the Instant Rotation Centre (posterior wall of the vertebral body). When the rotation is greater, the lever arms are on the same side and the vertebrae skids like a scooter in an excessive curve.
|
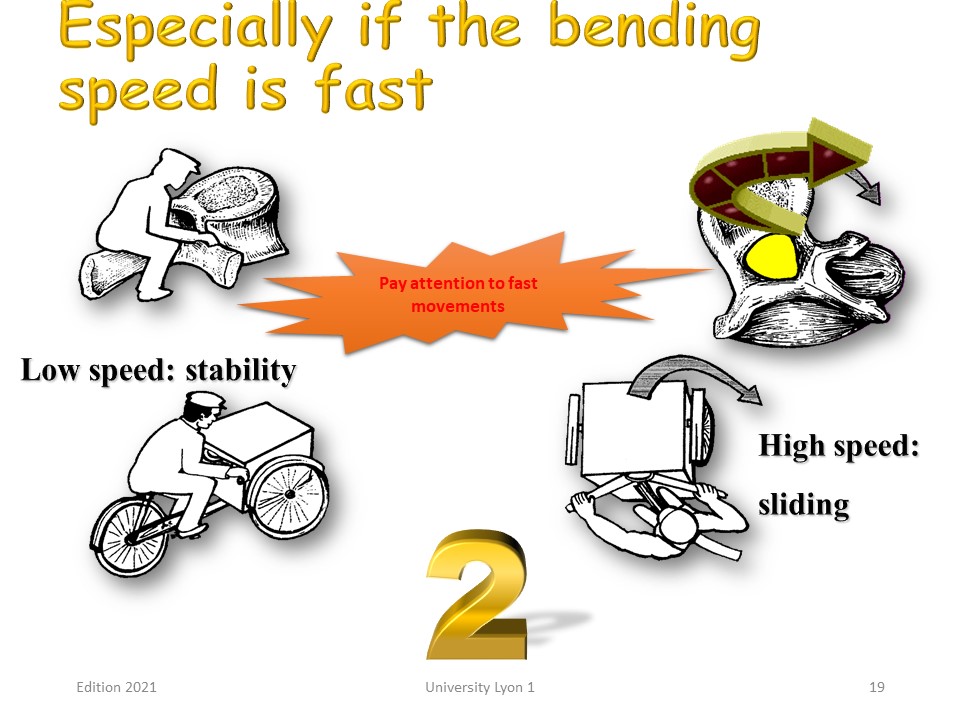 |
The speed of the anterior flexion of the trunk also contributes. If the flexion is performed slowly, the muscles stabilise. However, if the flexion is fast, there is also a skidding mechanism, such as a turn taken too quickly on the bicycle.
|
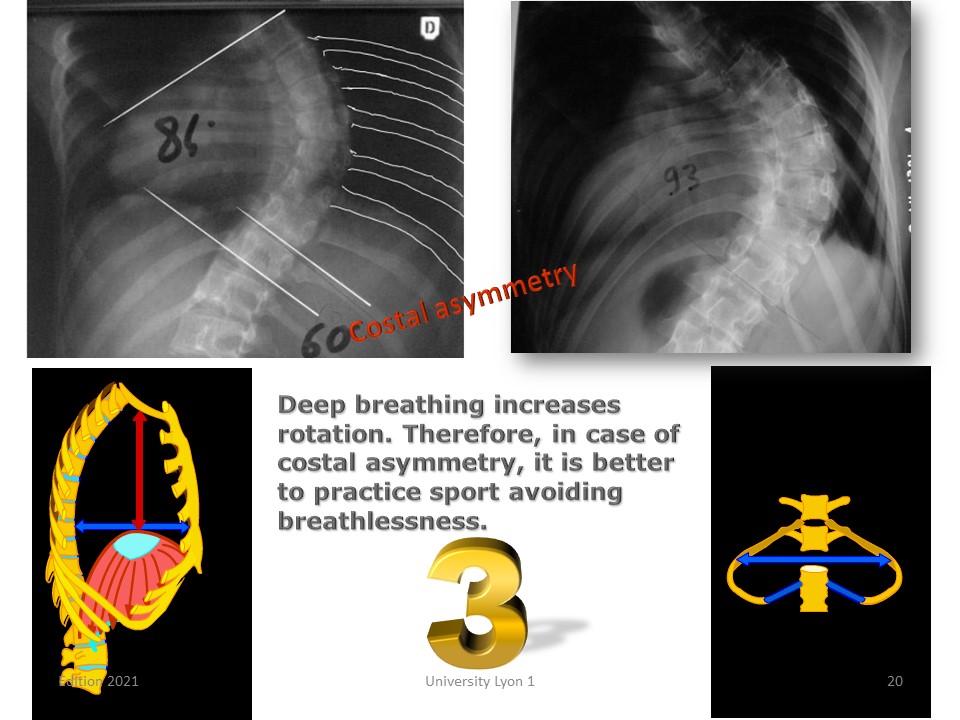 |
The costal orientation is also to be taken into account, it is very variable for the same Cobb angulation. In the case of significant asymmetry, deep breathing favours rotation. It is therefore necessary to avoid breathlessness when practising sport.
|
 |
The main risk factors in adulthood are therefore: imbalance of the occipital axis, Apical rotation, Flat back, Costal asymmetry, Short curvature (Harrington coefficient), Low vital capacity, Occupational invalidity.
|
 |
We will consider the clinical elements of adult scoliosis. Both adolescent scoliosis in the adult (ASA) and degenerative de-novo scoliosis (DDS) can cause significant pain, but their progression is different.
|
 |
In 1969 Vanderpool shows that the frequency of scoliosis in adults increases steadily with age until it reaches 10% of the population at age 65. The gender ratio of 2 women for a man is not the one we observe in everyday practice, which means that men consult less than women.
|
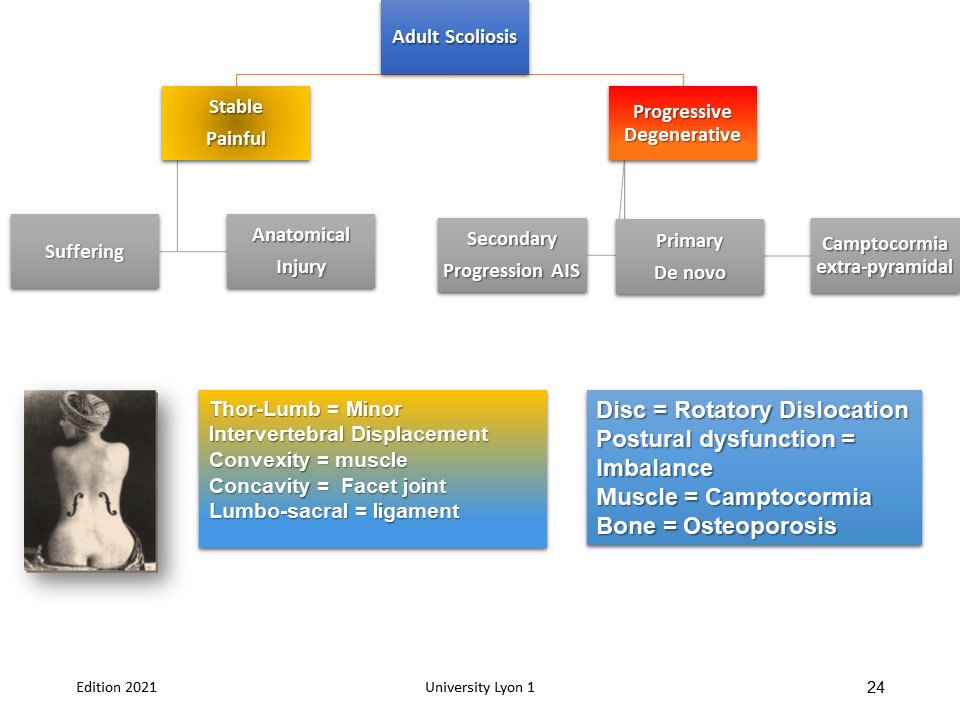 |
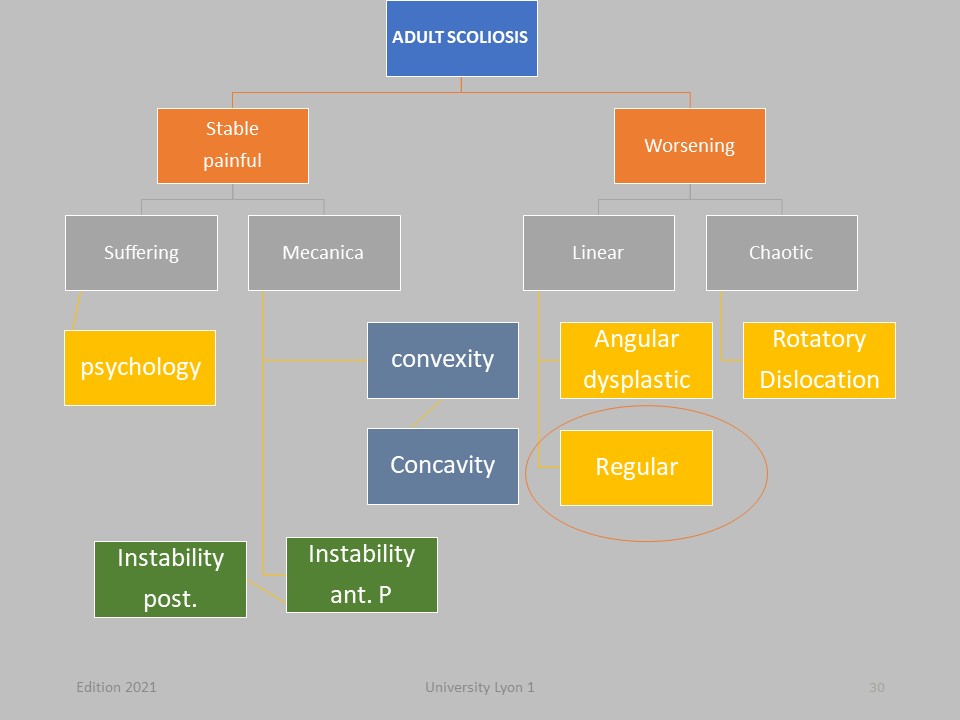
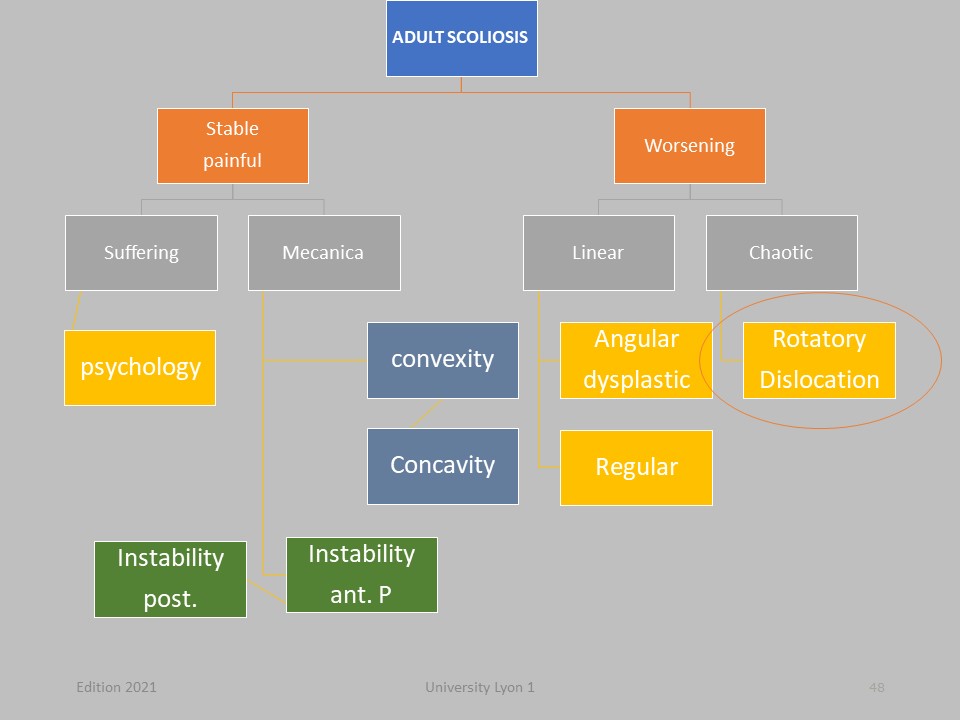
The pain is not synonymous with progression of the deformity. Some stable scoliosis are painful and others evolve without pain. It will be necessary to try to make the difference between the "anatomical" pain and the “suffering” when the patient does not support his deformation any more. Pain in adulthood depends more on the sagittal plane than on the frontal plane, Thoraco-lumbar pain often corresponds to minor instabilities. The pains of convexity are of muscular origin. The pains of the concavity are posterior: facet joint syndrom. The lumbosacral pain of ligament origin. These pains respond perfectly to physiotherapy. When scoliosis progresses, it is either: First the evolution in adulthood of an adolescent idiopathic scoliosis, or Second a de novo scoliosis usually of discal origin, or Third a camptocormia of muscular origin. In all cases, there may be: disc disease with sometimes rotatory dislocation, postural impairment with imbalance, extra pyramidal muscle involvement and bone involvement (osteoporosis). In these progressive cases, bracing or surgery may be necessary.
|
 |
It is often difficult to distinguish between suffering and mechanical pain: The rib hump is no longer accepted psychologically. The others’ eyes disturb, and the demand is aesthetic.
|
 |
From 20 to 30 years old, the main problem is the anatomical pain. From 30 to 50 years old, the main problem is the discal decompensation. Backpain is correlated to sagittal alignment. The prognosis of scoliosis in adulthood depends on the sagittal plane.
|
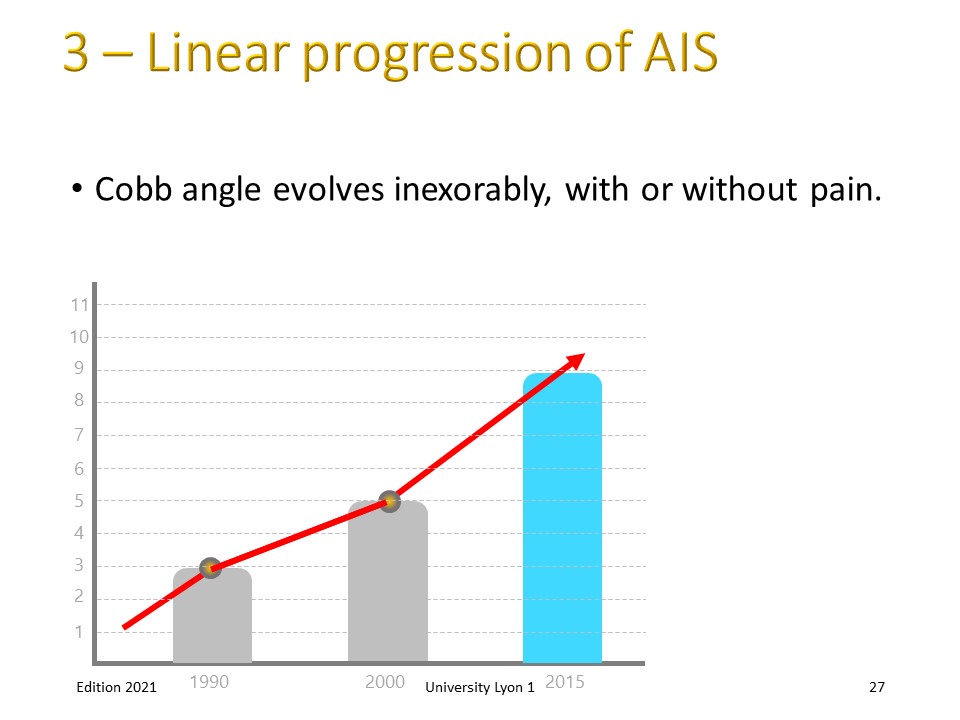 |
There are two types of progression: linear progression and chaotic progression. When scoliosis evolves in linear affine mode, the structures become unbalanced gradually and at a given moment the body can no longer compensate.
|
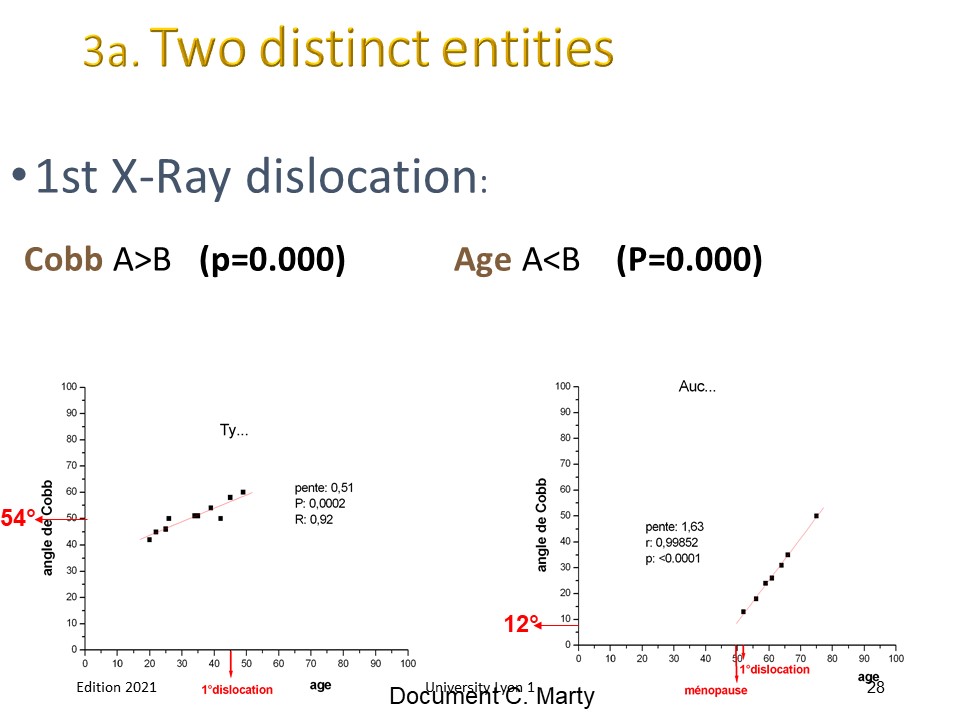 |
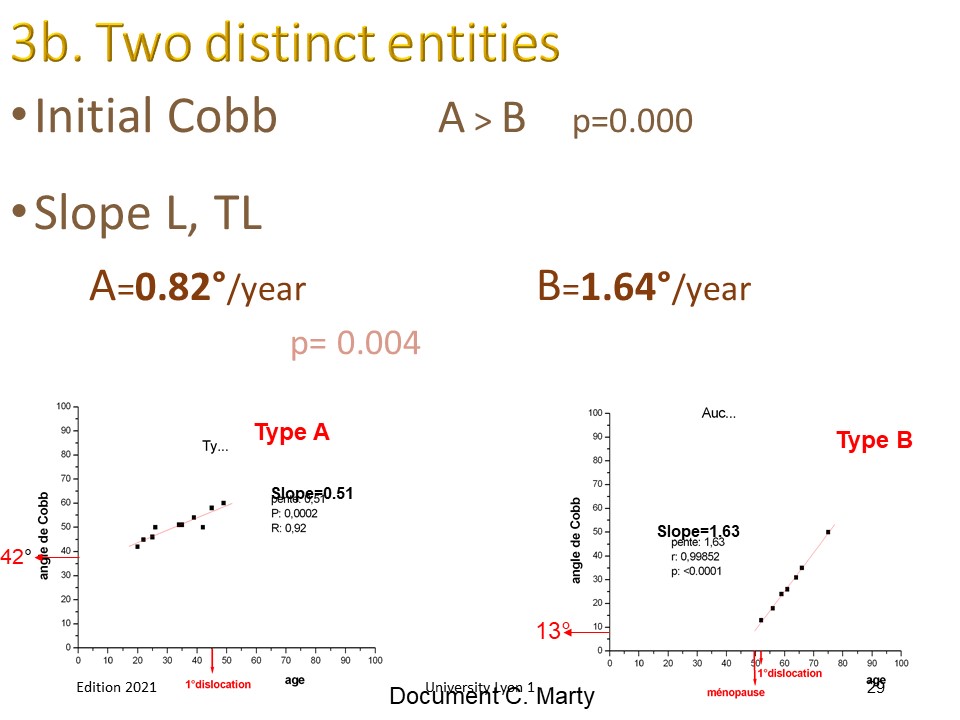
Two distinct entities: A = Adult Progression of AIS >40° with first rotatory dislocation at 45 years. The natural history was studied by Weinstein. The average progression is about 1° per year. B = de Novo scoliosis with low Cobb after 50 years. First dislocation at 52 years after menopause.
|
 |
De novo scoliosis are more progressive than Adolescent Idiopathic scoliosis. For AIS progression and respiratory problems are correlated to curve angulation.
|
 |
For group A, the evolution in adulthood can be regular. Physiotherapy is often performed during an episode of lumbar instability. Due to scoliosis the possibilities of natural adaptation are more limited and the vertebral loads must be perfectly distributed.
|
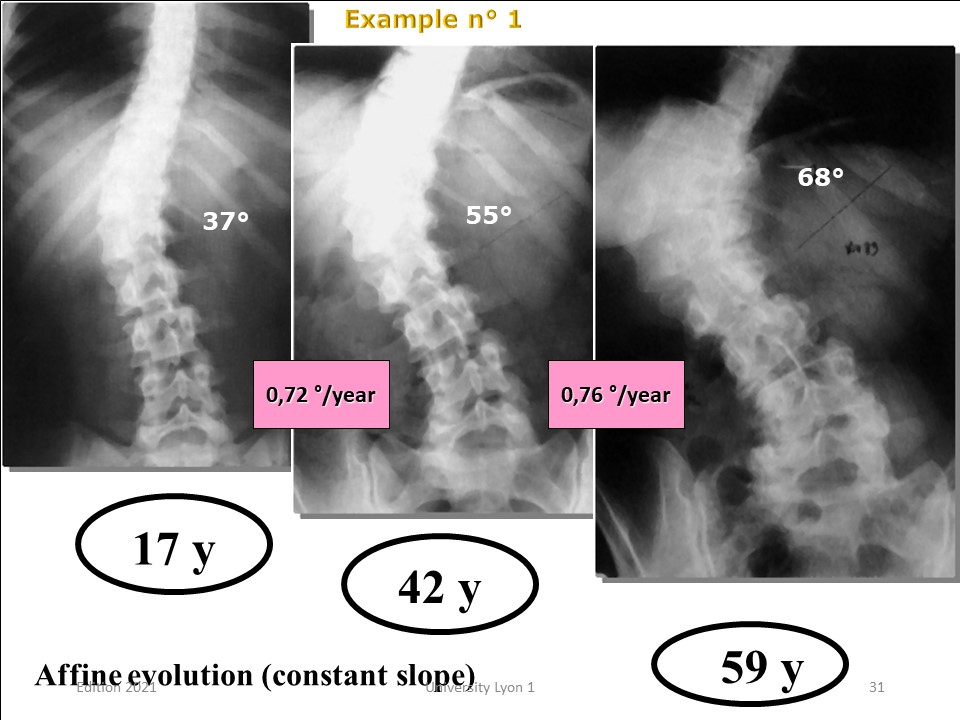 |
This example is characteristic of a Cobb angle regular affine progression of 0.72° per year
|
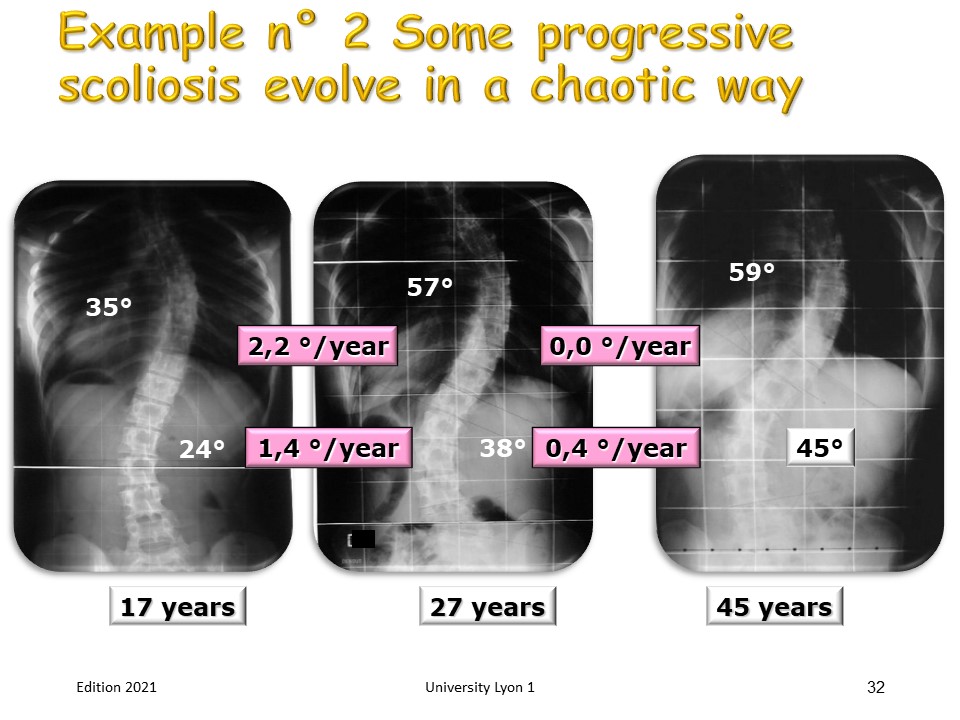 |
But not all scoliosis are progressing regularly. Some scoliosis will evolve for 10 years, then stabilize permanently. This chaotic evolution makes the surgical indication of limiting the progression of scoliosis very difficult.
|
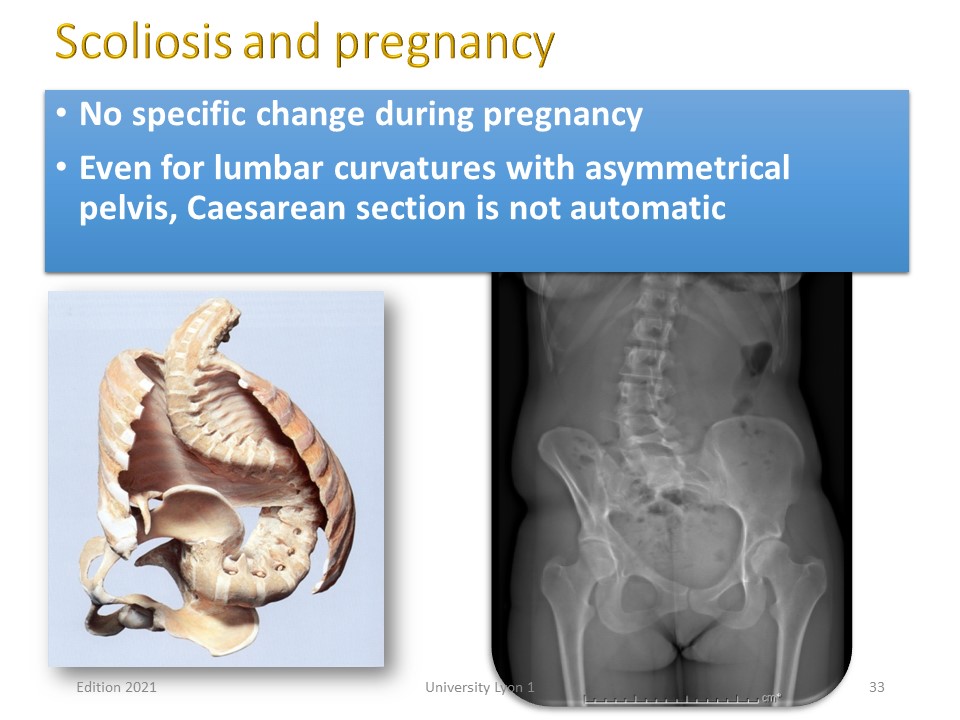 |
A frequent question is the impact of pregnancy on scoliosis. The longitudinal studies I did in 1980 with Pierre Stagnara did not show any change in the evolution of pregnancy. However, patients often consult after the second pregnancy and in general physiotherapy allows rapid recovery of lumbar and pelvic sheathing. A second problem concerns the pelvic asymmetry. They rarely require Caesarean section.
|
 |
Pregnancy does not change the progression of scoliosis in adulthood, except in cases of twin pregnancy. This patient was treated orthopedically during adolescence by Lyon Brace then Chêneau. At the end of treatment Cobb angle was 45 ° and remained stable until pregnancy.
|
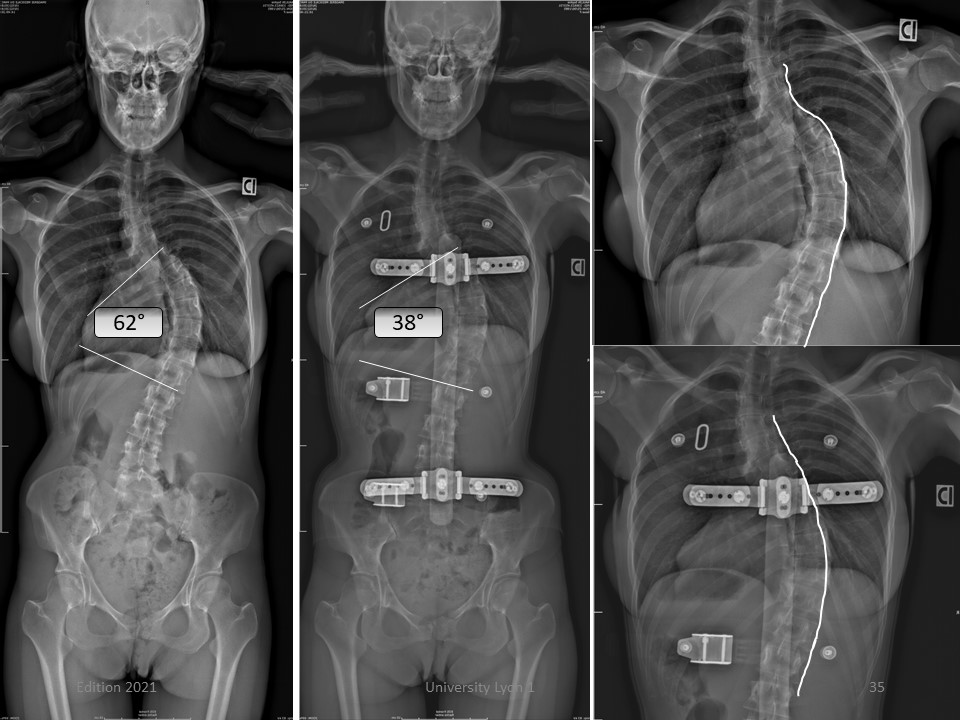 |
Cobb angle increased from 45 ° to 62 ° after childbirth. The in-brace angulation is 38 °. The sport activity was stopped during pregnancy.
|
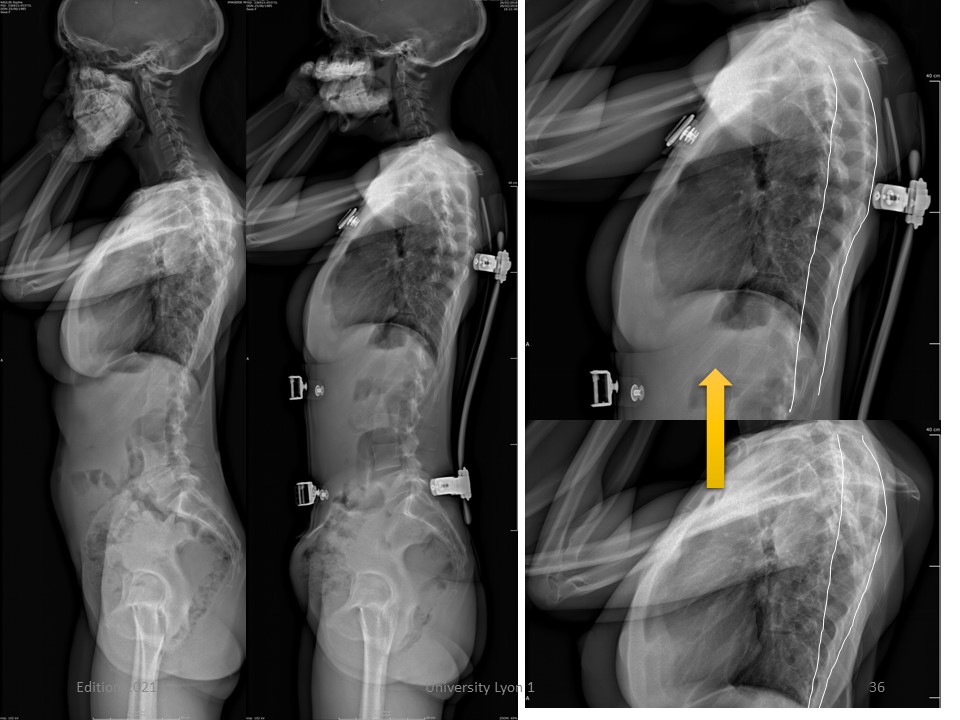 |
In the sagittal plane, the Grivas’ index that reflects the modeling of the rib hump, improves.
|
 |
Special protections have been added to the brace to facilitate breastfeeding.
|
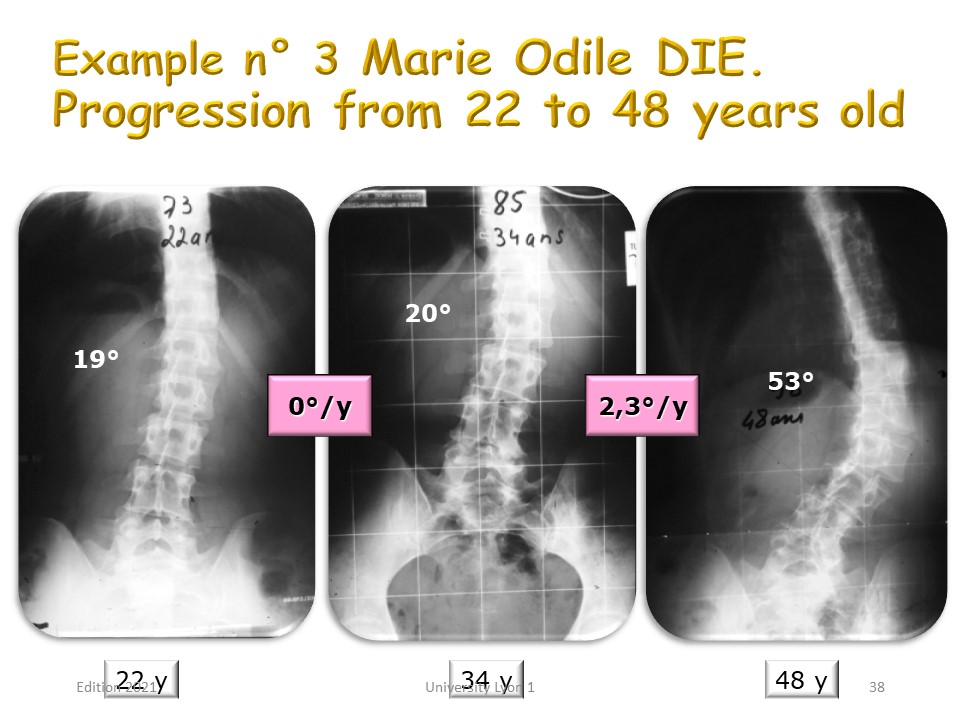 |
In this case, the progression in time is also chaotic. In this example, no progression between 22 and 34 years, then high progression of 2° per year between 34 and 48 years. Clinically, the accentuation of the rib hump, but especially the imbalance of the occipital axis will alert the patient.
|
 |
In 1987, Edgar presented the evolution of 78 idiopathic scoliosis with a follow up of more than 17 years. He notes a great progression disparity of scoliosis and only the curvatures of more than 90 ° have a linear evolution. But do all scoliosis more than 90 ° progress?
|
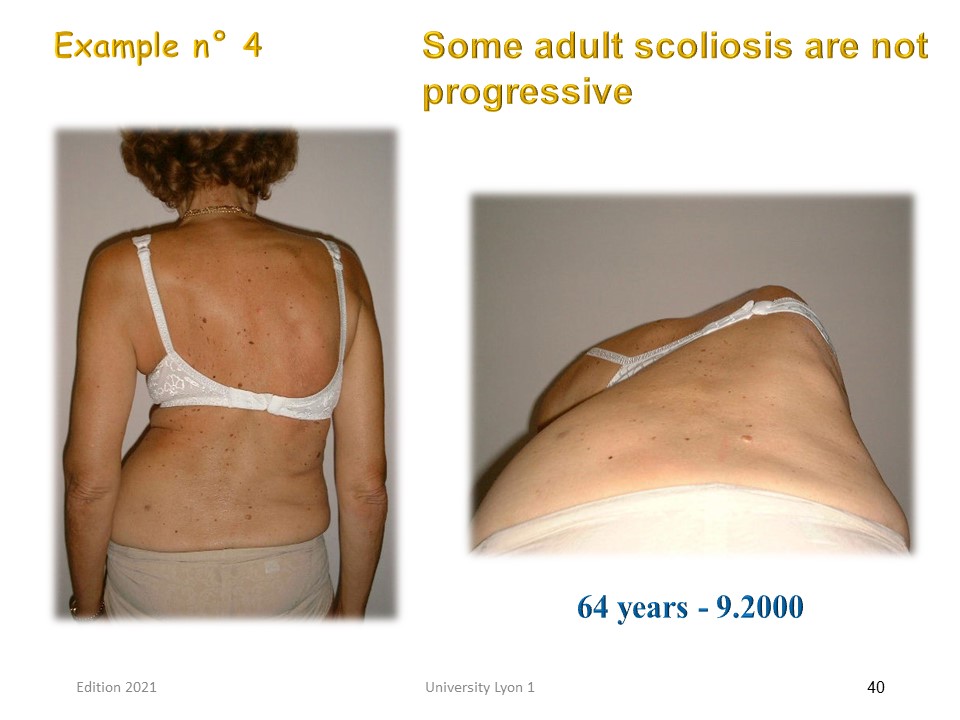 |
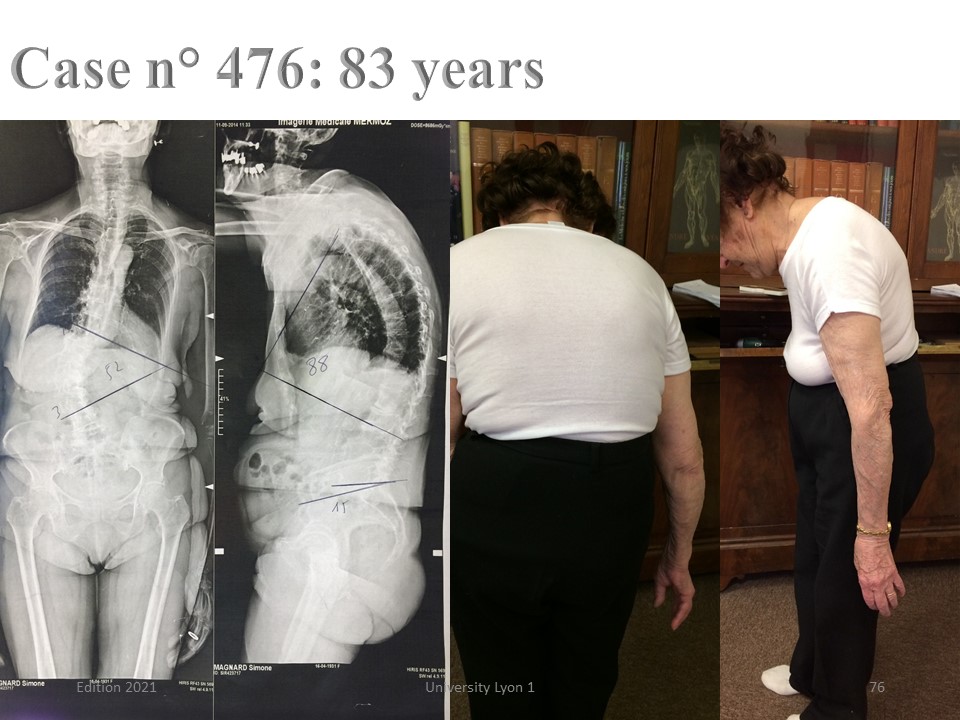
All scoliosis, even major, are not progressive. This patient with painful thoraco-lumbar scoliosis consulted at age 64 for pain without imbalance. She had been treated by plaster casts and braces during adolescence and had brought all her X-rays.
|
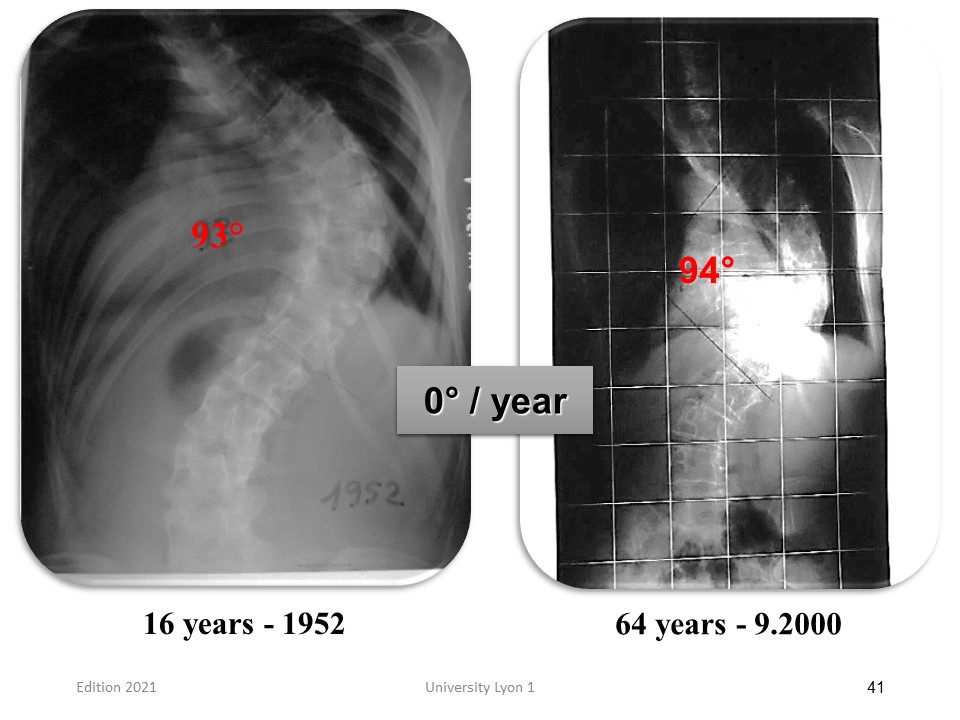 |
Here is the x-ray at the end of the non-surgical treatment and the X-ray at the time of the consultation. After 50 years, Cobb has not changed. This patient worked normally in the countryside and raised her 5 children. She consulted for some pain easily relieved by physiotherapy. If I had seen her at the end of treatment, I would have advised the surgery
|
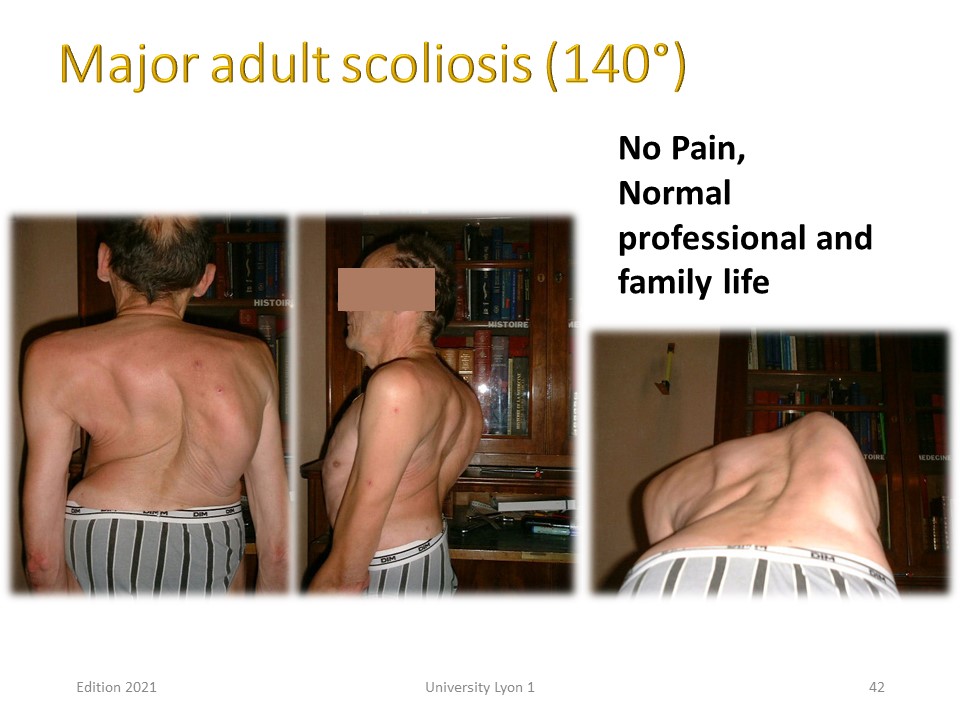 |
This patient presented an early onset scoliosis untreated during adolescence. He led a normal professional life with little pain and moderate respiratory discomfort. Angulation remains stable.
|
 |
Early works on scoliosis progression in adulthood were pessimistic, but mixed idiopathic scoliosis, especially rachitic infantile and neurological poliomyelitis that no longer exist. In 2003 Weinstein published the spontaneous evolution of 117 idiopathic scoliosis over more than 50 years. He does not observe a functional respiratory or painful repercussion below 70 °. This angular limit is currently the functional surgical limit.
|
 |
Major Risk factors have been studied by Schwab: Rotatory dislocation with lateral olisthesis. L3-L4 inclination. Hypo-lordosis. Increased thoraco-lumbar kyphosis. The Visual Analogic Score is not correlated to scoliosis and Cobb angle.
|
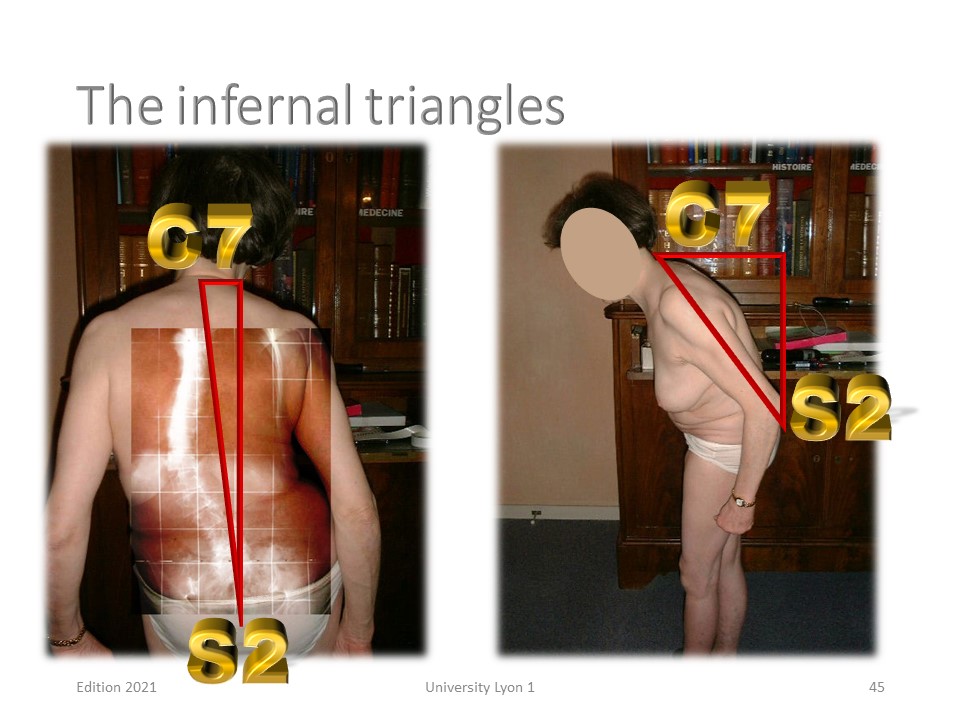 |
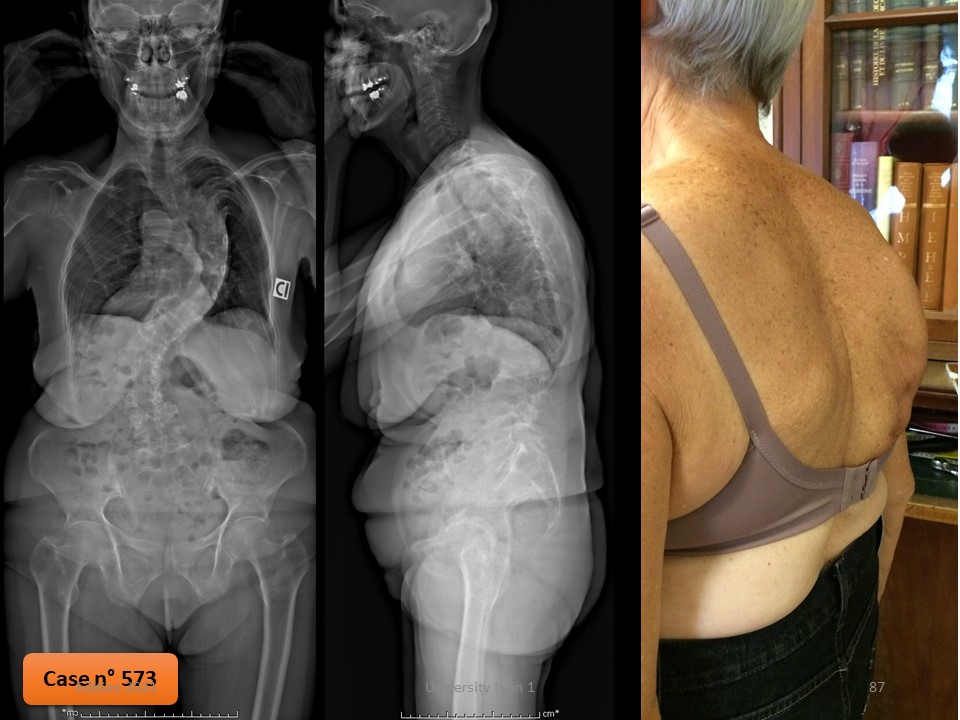
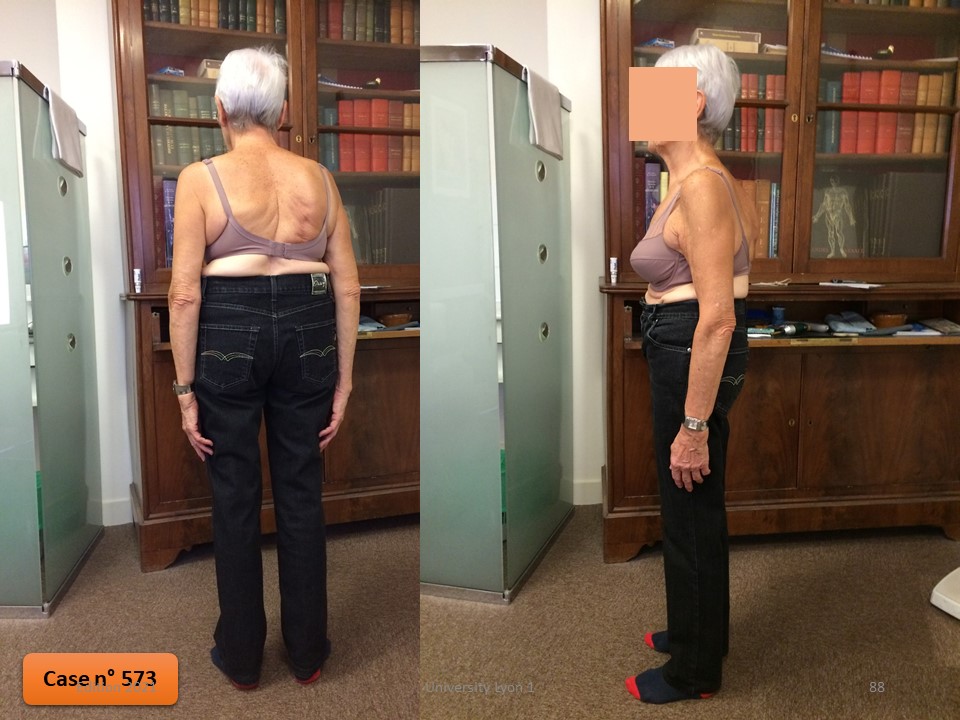
One of the most characteristic features is the imbalance of the spine. In this patient, the imbalances in the sagittal plane and in the frontal plane are clearly visible.
|
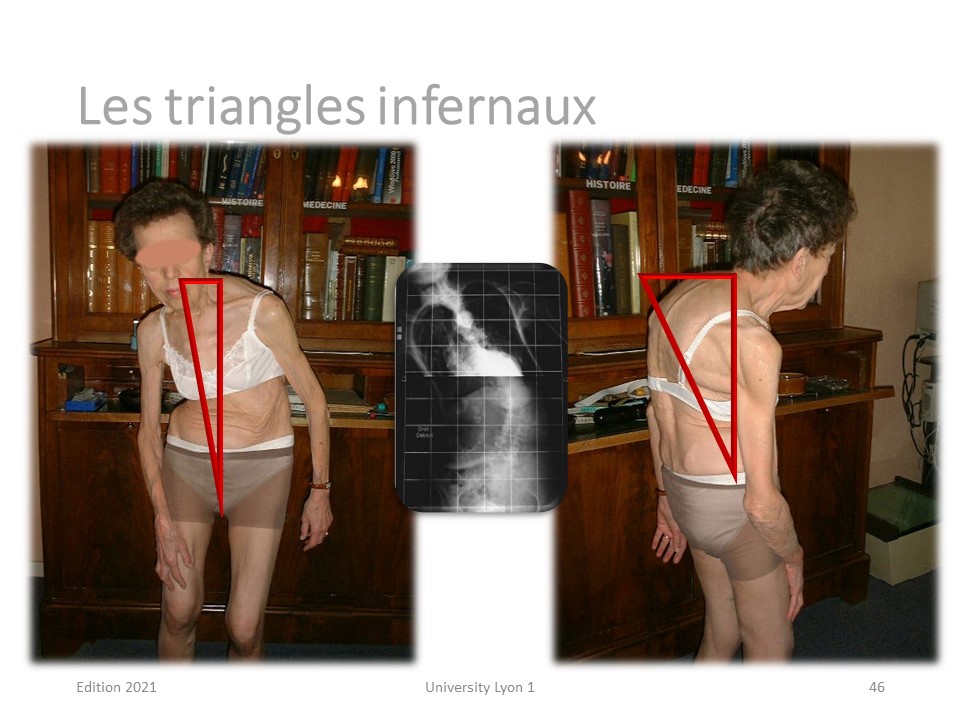 |
The patient is balanced only at the cost of stabilization with support on the right thigh. In addition to scoliosis, this patient presents with a high thoracic kyphosis of the osteoporotic type.
|
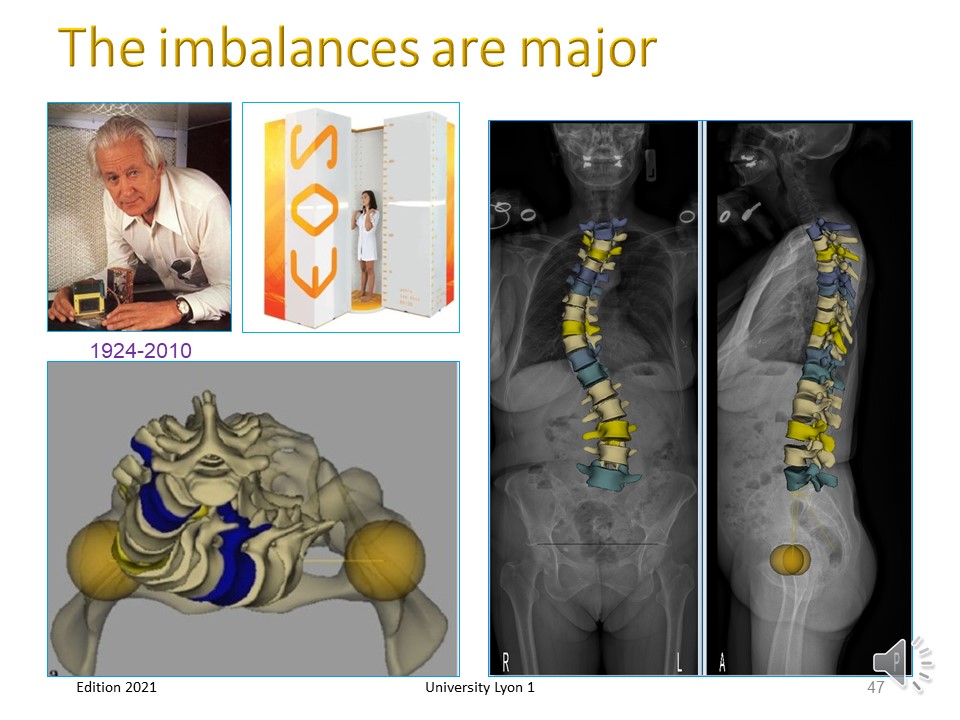 |
The current EOS 3D radiological technology with Ultra Low Dose, due to the invention of the Nobel laureate Georges Charpak, allows us to better reproduce these imbalances of frontal and sagittal plane, but also in Da Vinci View (above on the left)
|
 |
Rotational dislocation is the fundamental biomechanical element in the chaotic evolution of de novo degenerative scoliosis.
|
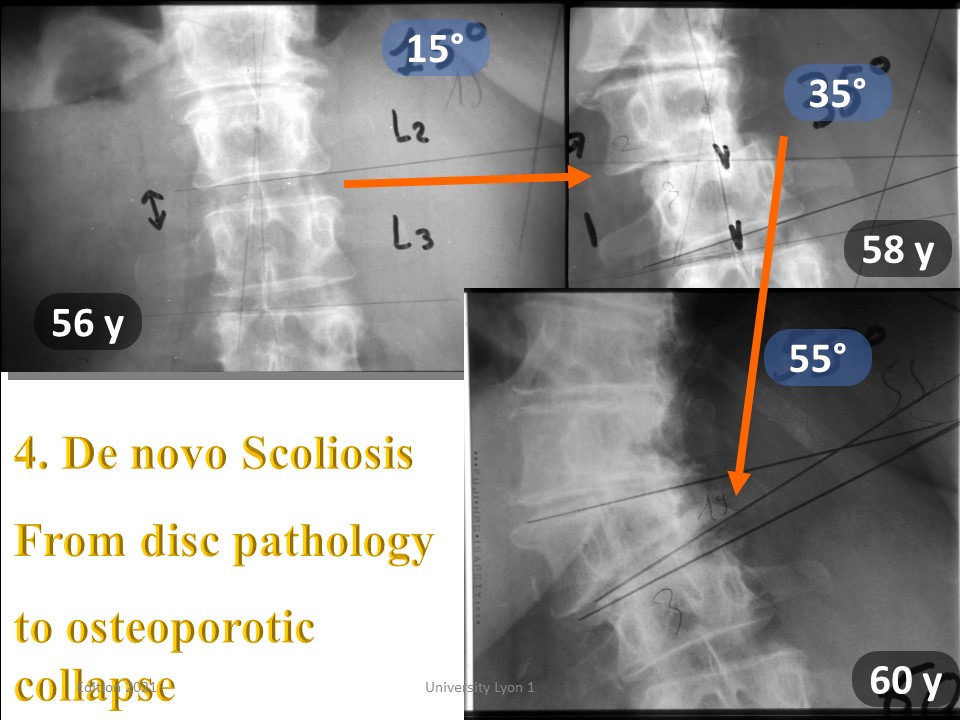 |
Here is a typical example of de novo scoliosis with late-onset and rapid evolution associating discopathy and probably osteoporosis. The progression of 40 ° is linear between 56 and 60 years.
|
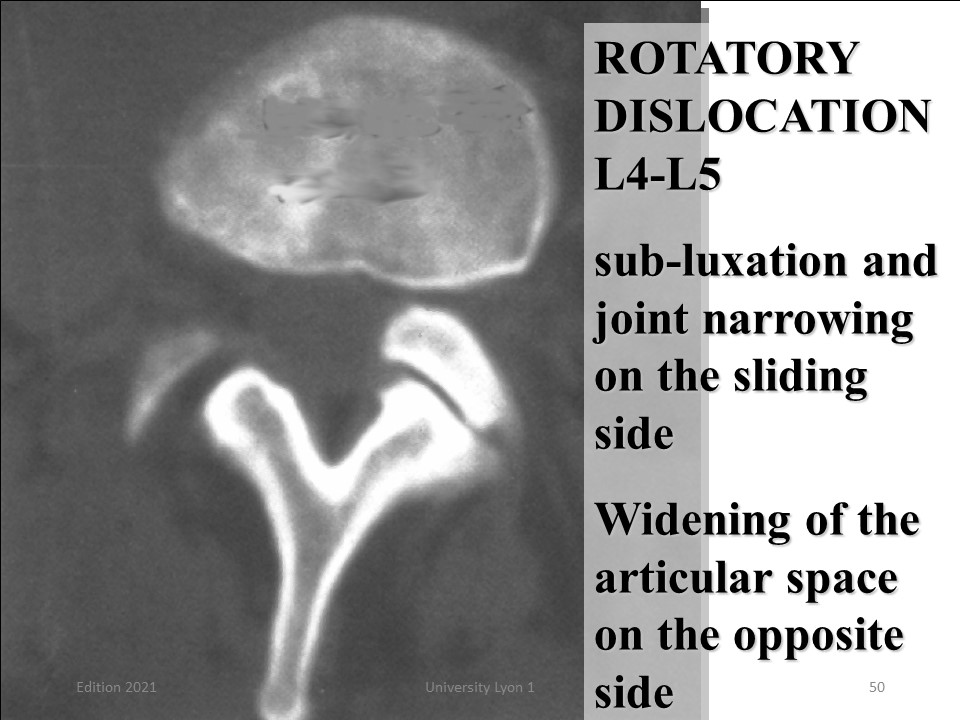 |
The usual mechanism is of intervertebral disc origin. It is the rotary dislocation visible on this cross section with. sub-luxation and joint narrowing on the sliding side, Widening of the articular space on the opposite side.
|
 |
The majority of patients consult during periods of rotatory dislocation or disc instability. Non-operative treatment may also be useful for instability under surgically treated scoliosis. Nonsurgical treatment is not effective for lumbar stenosis.
|
 |
Physiotherapy care is different from adolescent scoliosis. As the patient is seen in painful periods, analgesic techniques such as massage will be favoured. The techniques will be specified in the workshops. During adolescence, the frontal plane is corrected in sagittal isostatic balance, whereas in adulthood, exercises in the sagittal isostatic plane are given priority. Spinal mobilisation is very limited by rigidity. The pyramidal musculature will be strengthened after the age of 40. The geometrical detorsion is carried out in a square between the trunk and lower limbs. Rectus femoris and iliac psoas will be reinforced to limit retroversion.
|
 |
The technology will be specified in the workshops. Here, some special features are presented. In addition to the 90° square between the trunk and the lower limbs, the physiotherapist will ensure that the lumbar lordosis is maintained during the exercises.
|
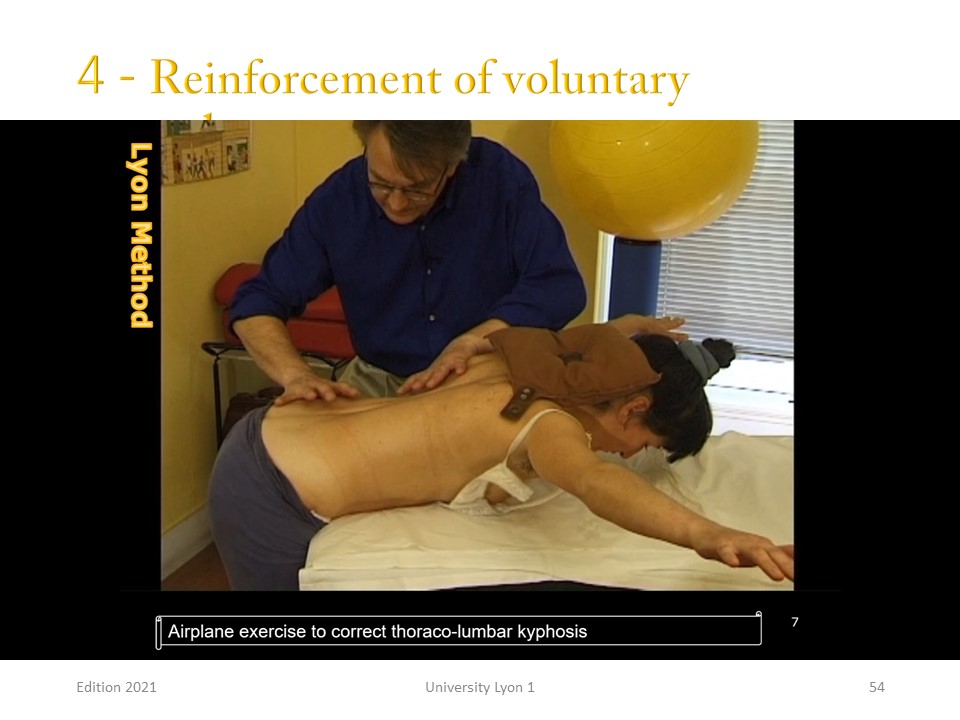 |
More sandbags and small dumbbells will be used to strengthen the pyramidal muscles with respiratory control in deep exhalation to promote aerobic metabolism.
|
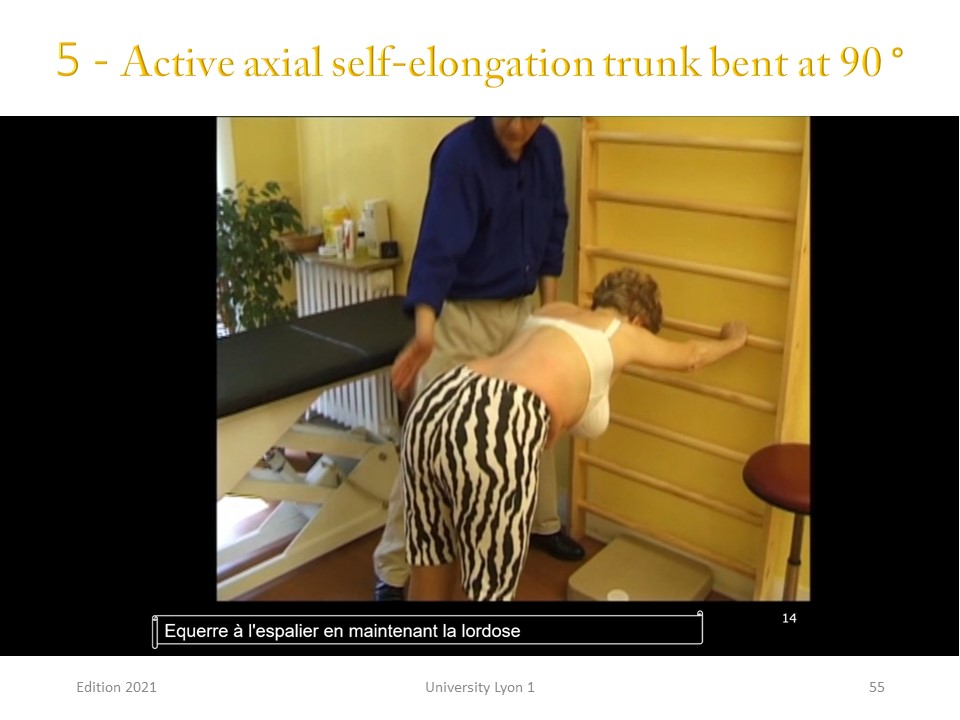 |
The active axial elongation takes place in a closed kinetic chain, which facilitates the control of the sagittal plane with reduction of upper thoracic kyphosis and maintenance of lumbar lordosis.
|
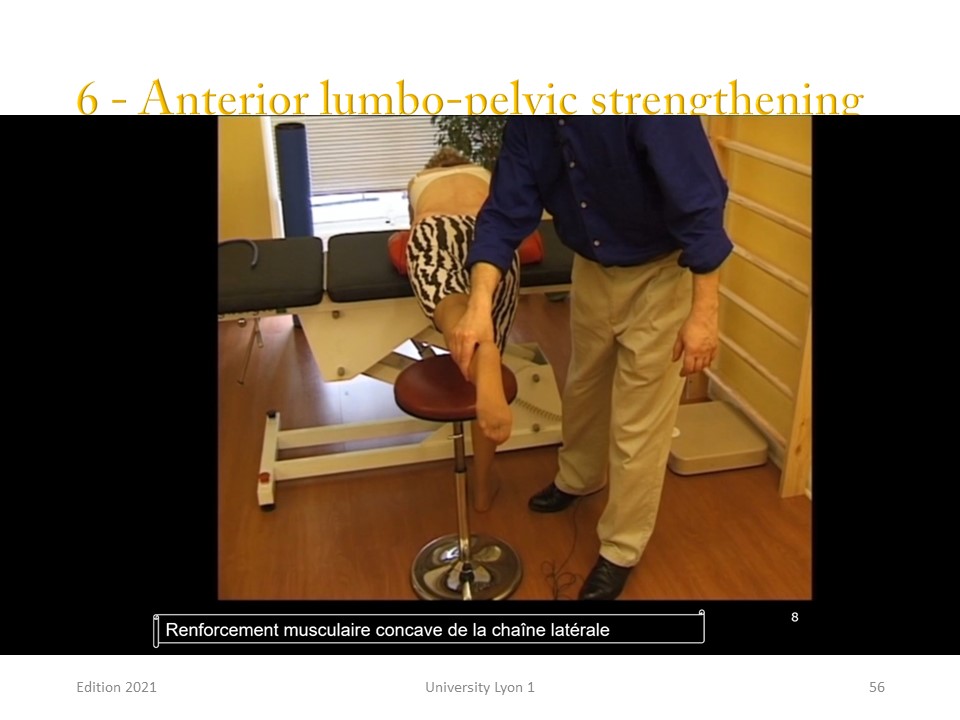 |
The lumbo-pelvic anterior chain will be stretched and reinforced in hold-relax.
|
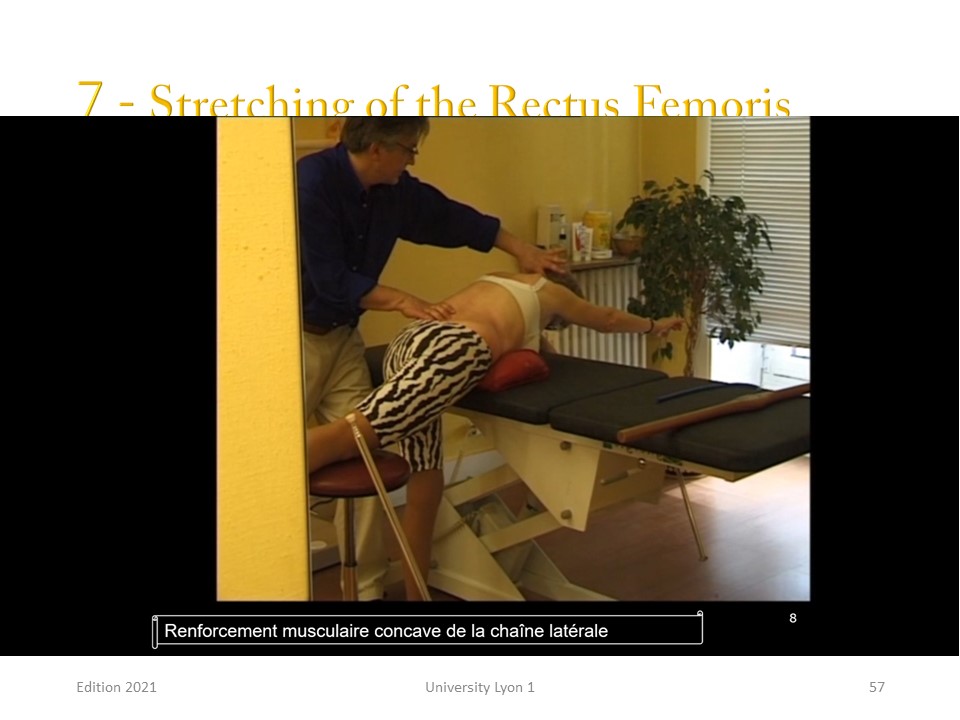 |
At the level of the hips, we work in an open kinetic chain to avoid pelvic retroversion of the psoas on the reflection pulley.
|
 |
For adults, new technologies have accentuated the precision of the brace's construction, allowing the use of high rigidity plastics with a correction equivalent to that of plaster casts.
|
 |
The corrective position is derived from the Schroth. The sagittal and frontal planes are corrected simultaneously, taking into account the overall balance of the spine. The spine is placed in maximum extension to promote lumbar lordosis and reduce thoracic hyperkyphosis. Digital moulding has replaced the traditional plaster cast. The advantages are multiple: 1. the patient can maintain the maximum corrected position in an upright position for a few seconds. 2. Breathing is controlled, and the patient can be asked for maximum inspiration. 3. The accuracy of the 8 sensor structures is less than 1mm. 3. mm polycarbonate with very high rigidity can be used instead of polyethylene. The treatment, which is carried out here in real time, is very fast. The green trace corresponds to the infra-red which calculates the depth. The cleaning of the image is carried out automatically. It is possible to work bare-skinned, but the optical jersey makes it possible to use reference points for the superposition of the 3 blocks if necessary. The processing allows for the creation of the positive which will be milled by milling machine. The CPO has all the tools required to modify the captured shapes.
|
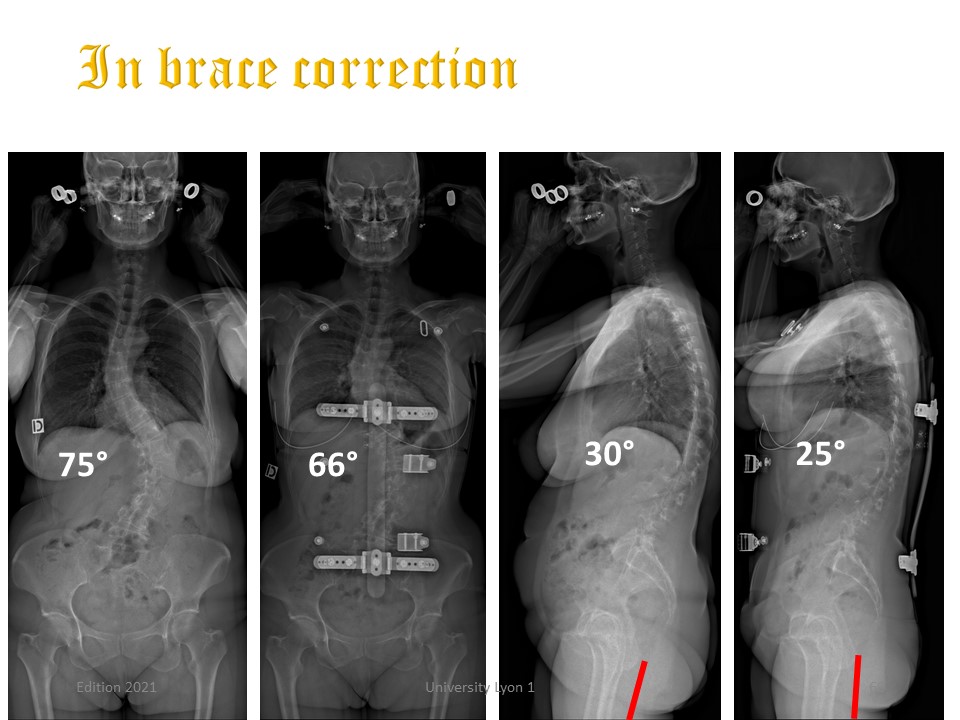 |
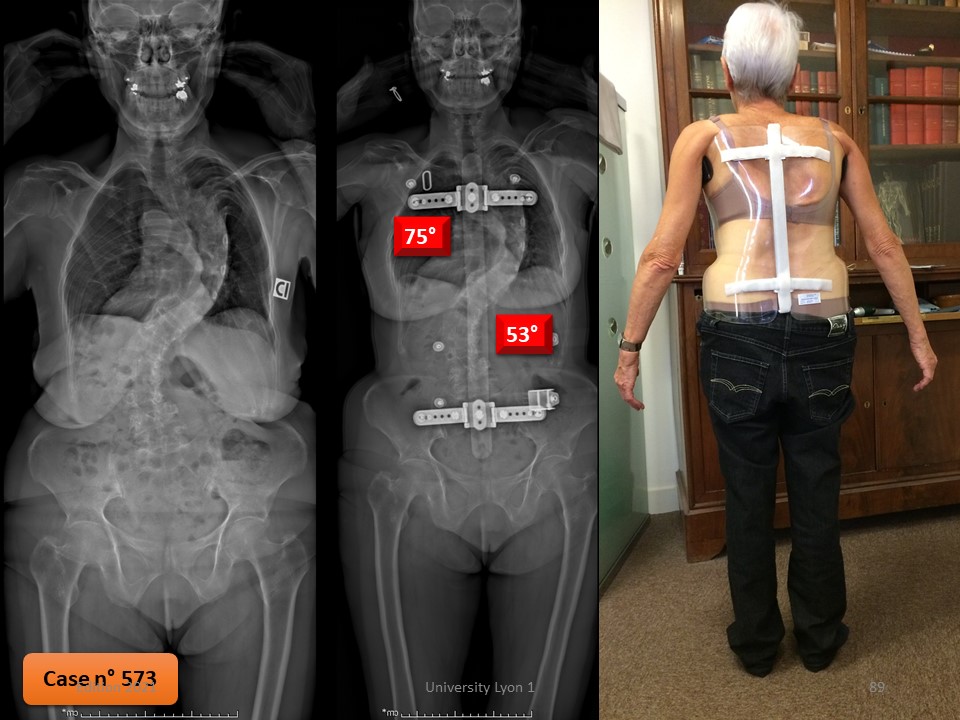
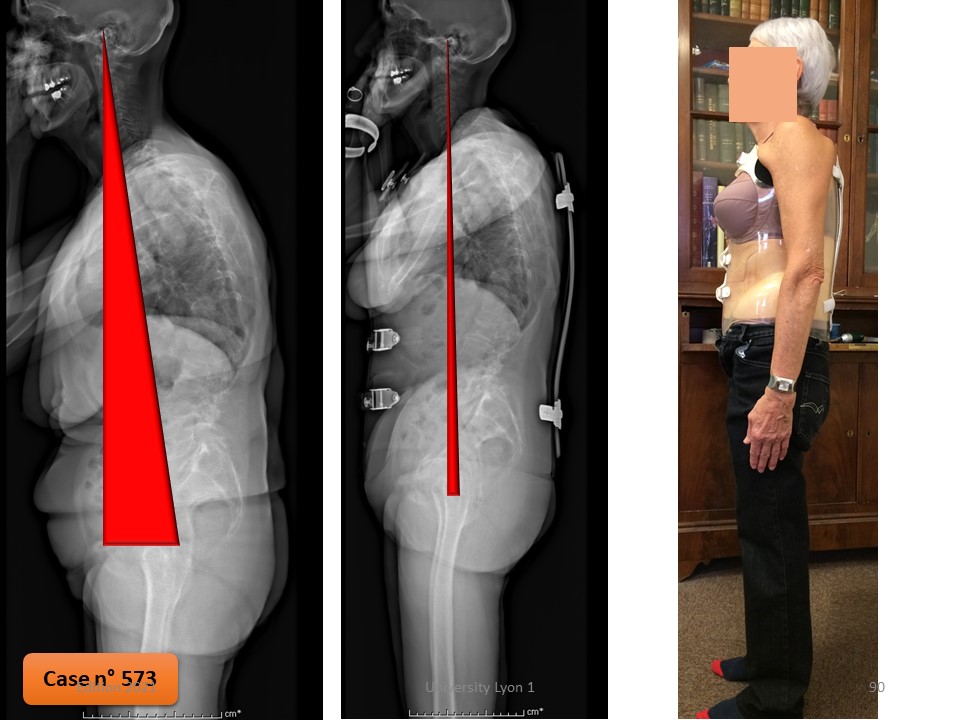
The important thing is the rebalancing of the occipital axis, which is controlled perfectly on the computer screen, allowing to choose the best corrective posture. Angular correction in the brace remains limited, but small improvements are generally sufficient to restore stability od balance of the scoliotic spine.
|
 |
This technological improvement was recently evaluated 2 years after fitting the brace
|
 |
The polyethylene brace used in adulthood does not correct scoliosis to such an extent that the brace is not radiologically controlled.
|
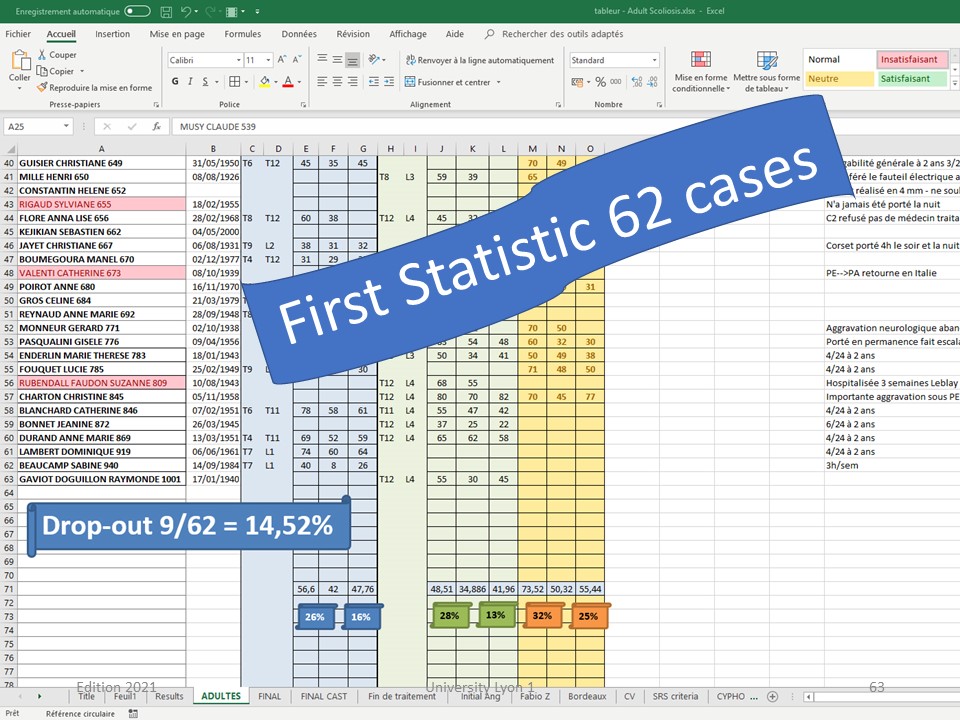 |
The first statistic was carried out on 62 patients. The drop out rate of 15% is low.
|
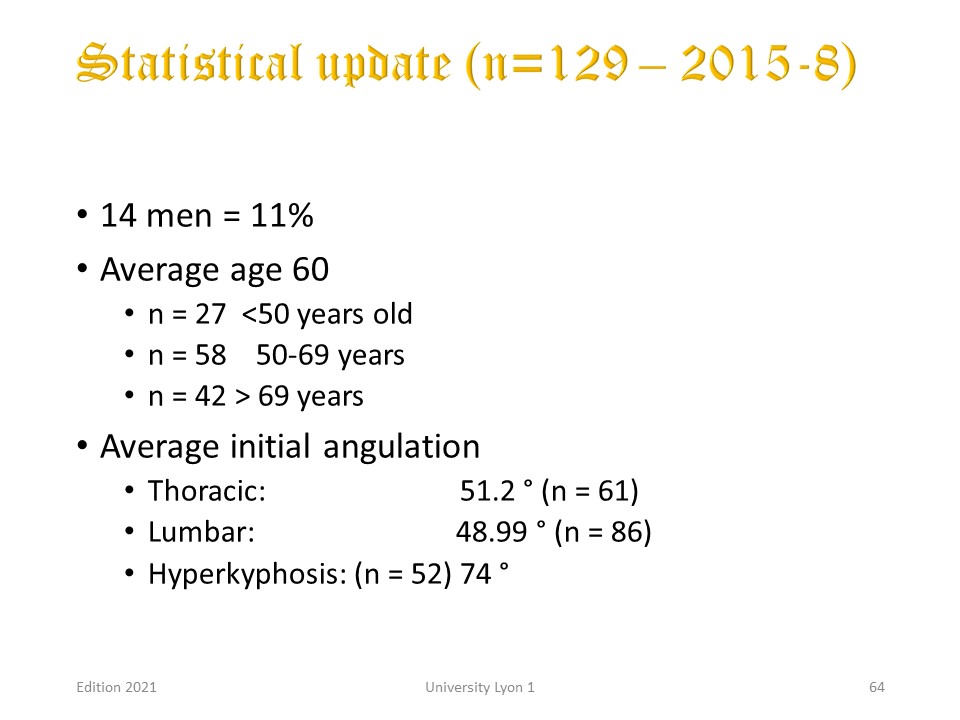 |
The last statistic was carried out on 129 patients treated on average at 60 years of age for an average scoliosis of 50° with thoracic hyperkyphosis of 74°.
|
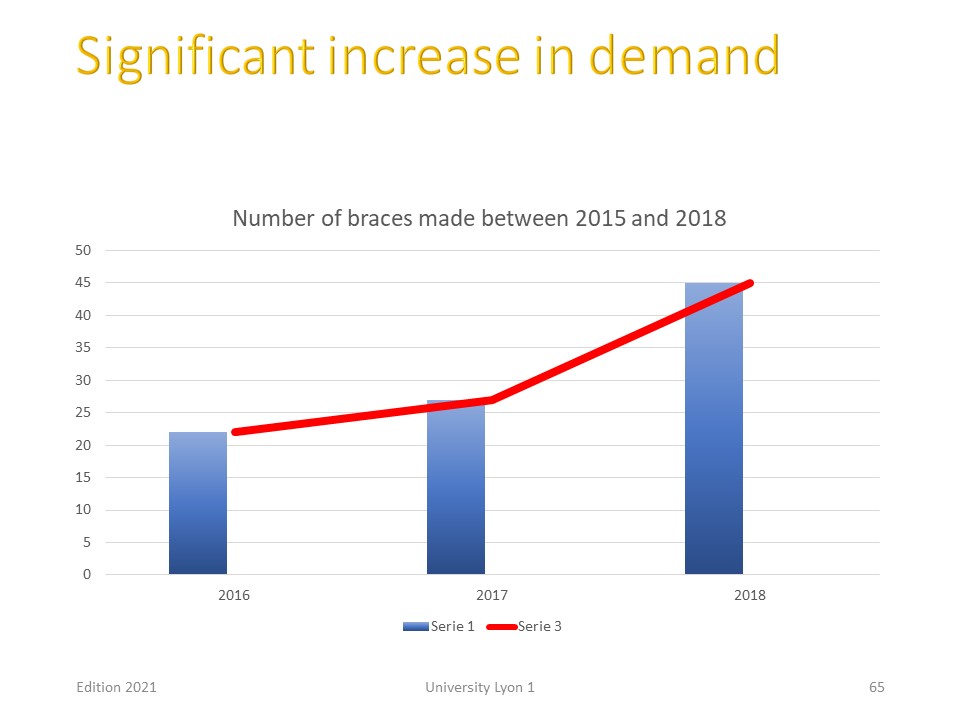 |
We have seen a strong increase in the number of patients in recent years, which seems to us to be in favour of the effectiveness of treatments that are frequently evaluated by patients on social networks.
|
 |
The drop out rate is identical to that of the first statistic. The patients concerned are older and above all present multiple associated pathologies.
|
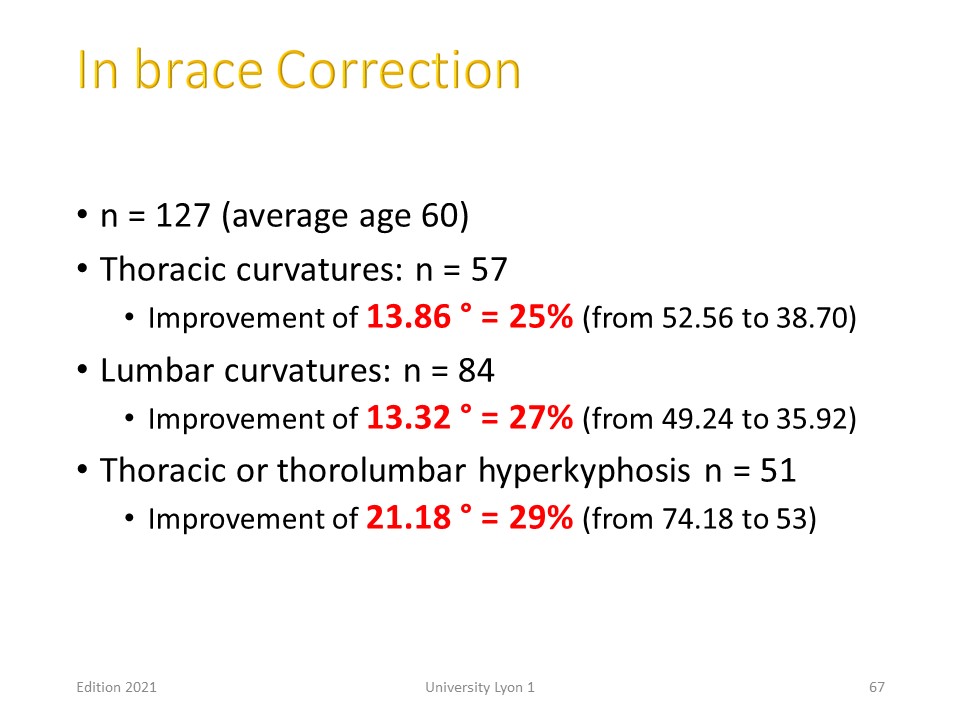 |
The correction in the frontal plane is 25%, it is of the order of 30% in the sagittal plane. Such a correction has never been published to date.
|
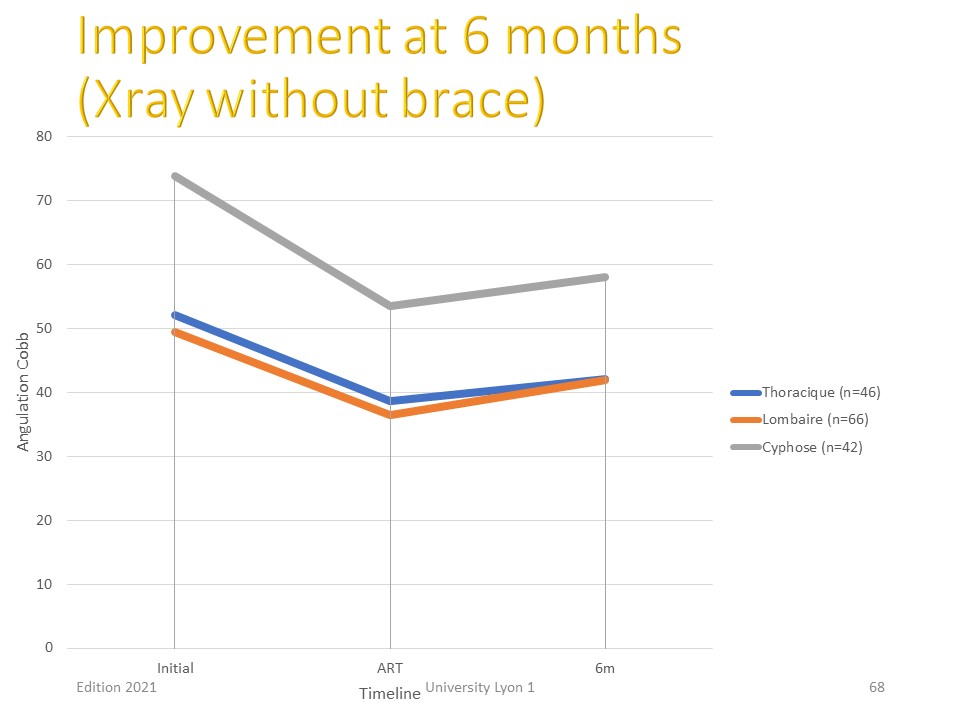 |
This correction is obtained in the first 6 months of treatment with a brace worn for an average of 4 hours a day.
|
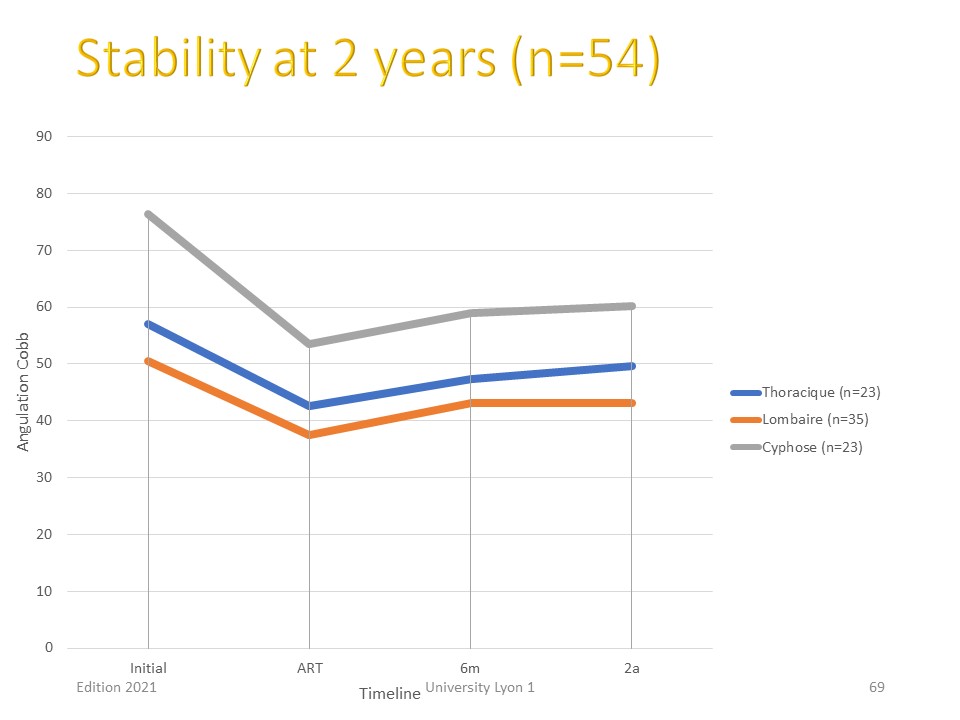 |
It holds well in the two years following the application of the brace.
|
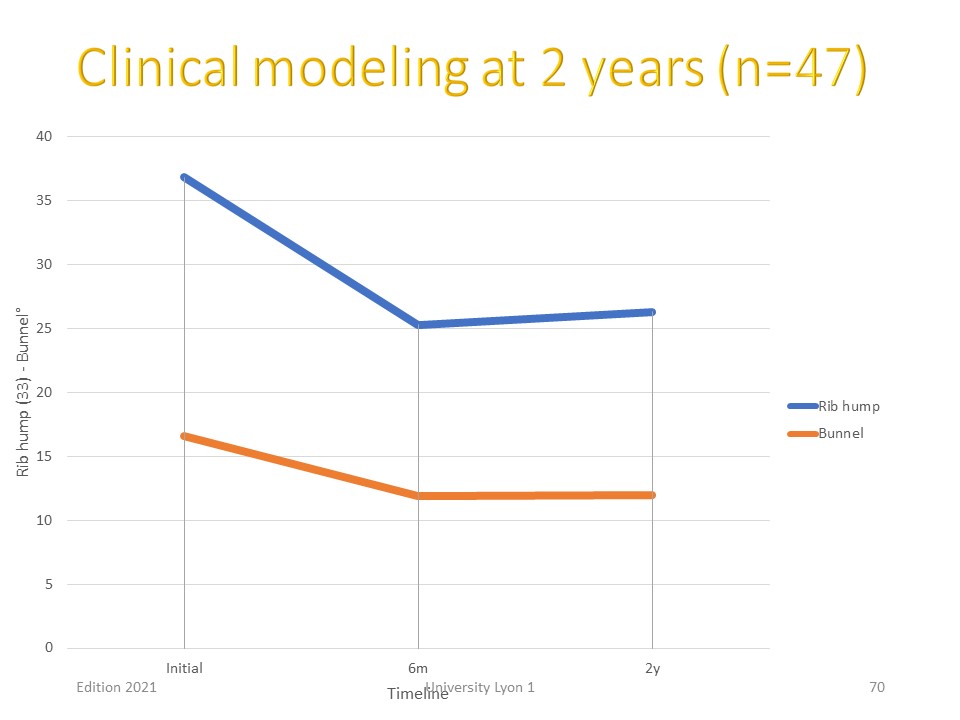 |
The shaping of the rib hump follows the same evolution with a morphological improvement which completes the general balance of the spine.
|
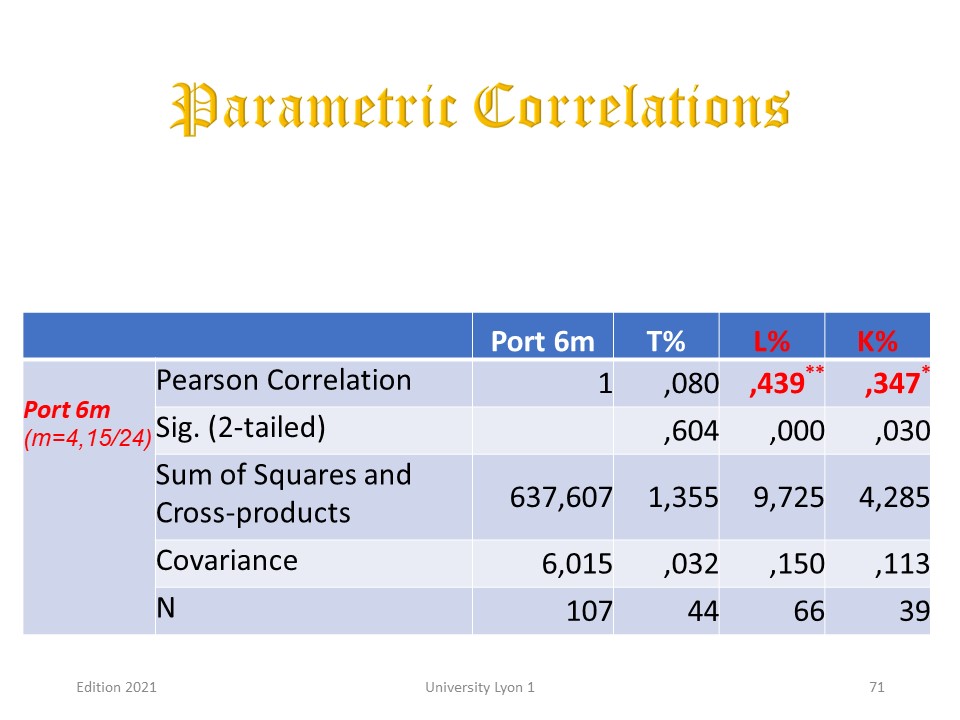 |
There is a correlation between the wearing time of the brace and the correction obtained after 6 months for lumbar scoliosis and kyphosis. The longer the brace is worn during the day, the greater the correction.
|
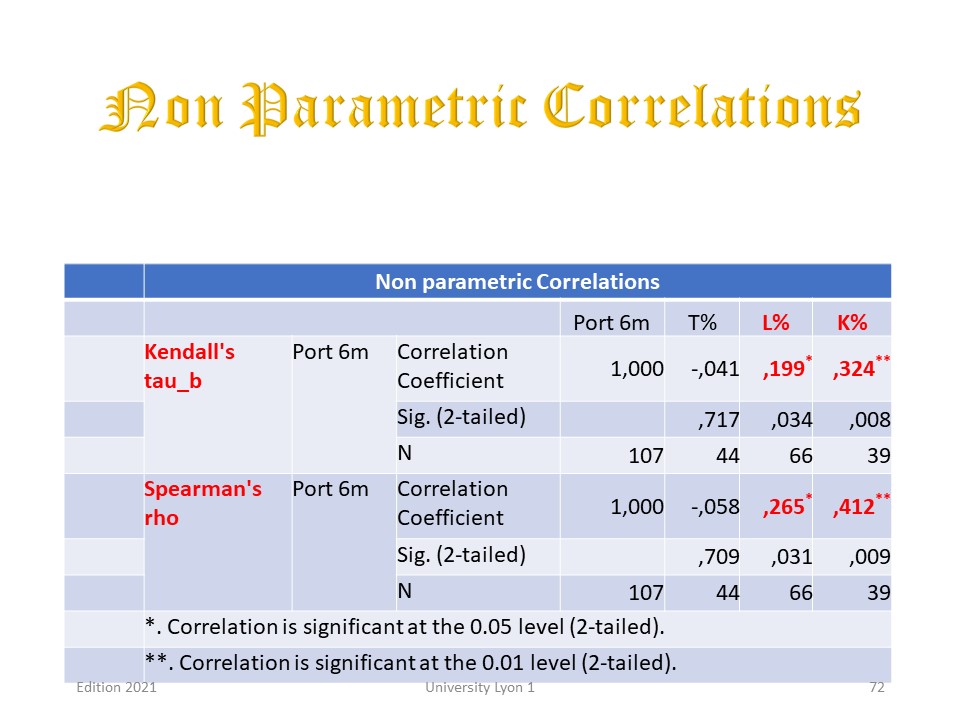 |
The results are confirmed by the non-parametric tests. It is therefore no longer just an analgesic immobilisation brace, but a real corrective brace.
|
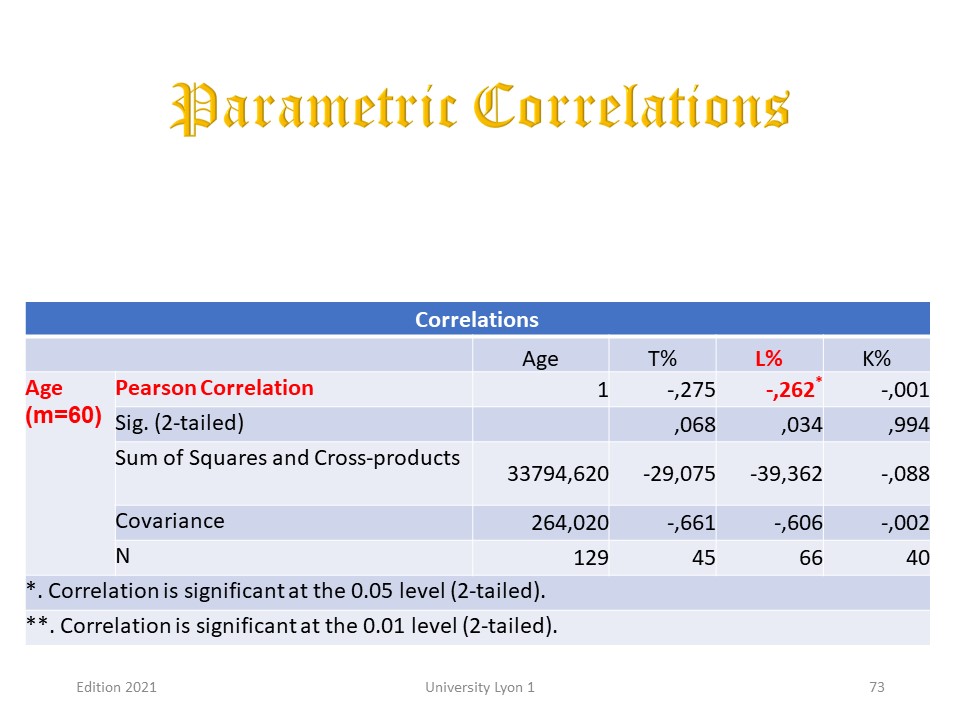 |
The age of the patient at the time of treatment is not an exclusion criterion, although correction in the frontal plane is somewhat greater in younger patients.
|
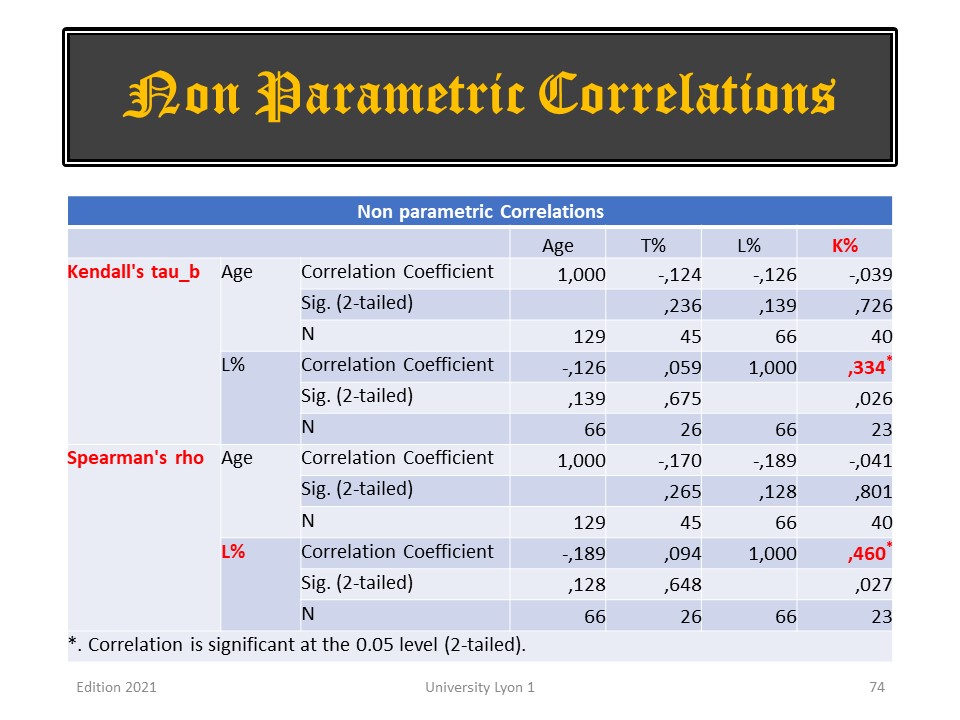 |
Non-parametric tests confirm that there is no correlation for correction in the sagittal plane.
|
 |
We have already presented some clinical cases in the chapter concerning the evolution of scoliosis throughout life. Here we will complete this presentation.
|
 |
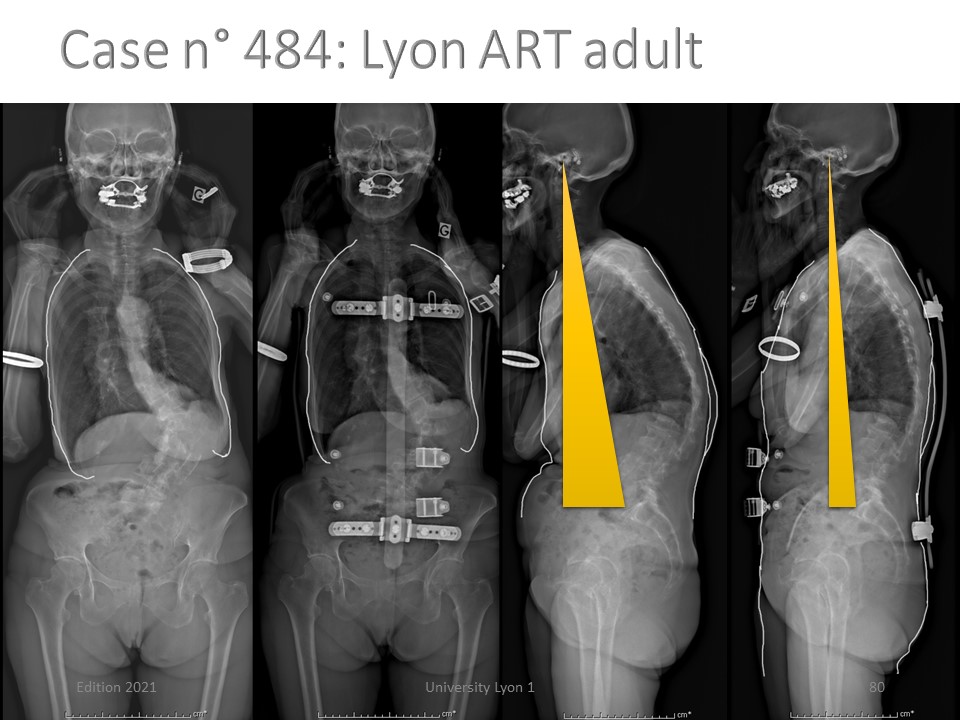
This is the first adult patient treated by ARTbrace. She lived near the Clinic. She consults for walking difficulties related to the imbalance of the occipital axis to the left and the accentuation of her kyphosis.
|
 |
In the sagittal plane, the spine is better balanced. The inclination of the sacral slope increases from 15 ° to 27 °, lordosis and kyphosis improve. The posture of the head is significantly improved.
|
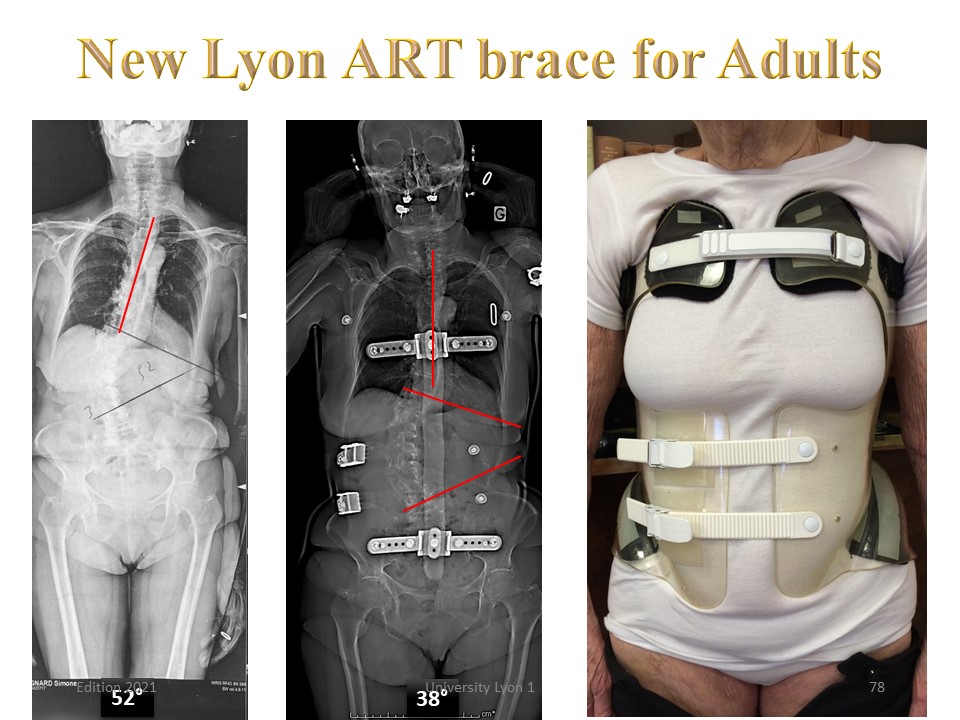 |
In the frontal plane, we note a significant improvement in scoliosis, but especially a rebalancing of the thoracic spine above. The brace is well tolerated and the patient can put it alone.
|
 |
The realization of the brace is very similar to that of children. The main differences are: 1. use of a 3 mm polycarbonate. 2. The thoracic scan is done in maximum inspiration. 3. At the back, the brace stops at the apex of the kyphosis. 4. In front, the clavicular support is expanded.
|
 |
On these EOS radiographs highlighting the shape of the torso, we see better the changes made by the brace. The spine seems to unfold. The tube mayonnaise effect, the baby lift, and the high rigidity of polycarbonate probably explain this result.
|
 |
When the kypho-scoliosis is at the thoraco-lumbar level, it is possible to fill the posterior bar with a foam to improve tolerance.
|
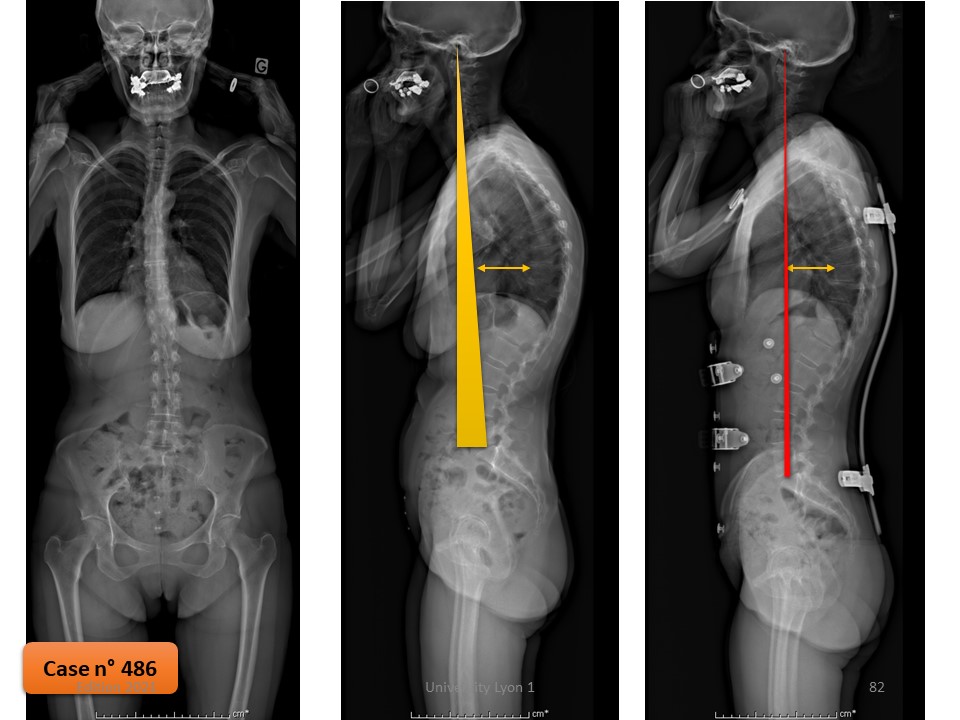 |
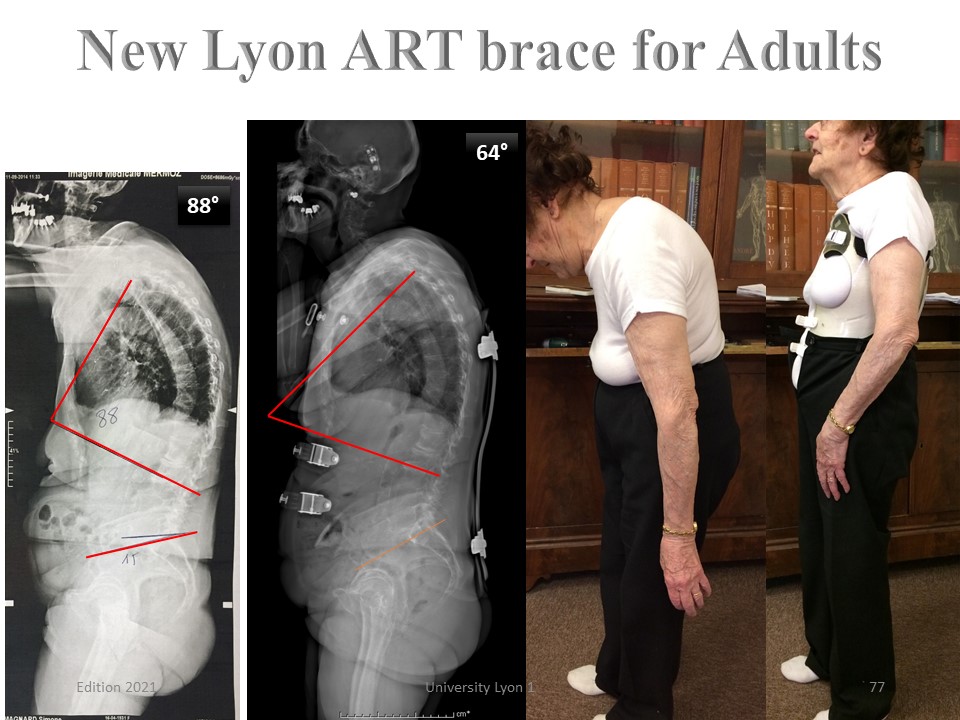
This 58-year-old patient consults for left-sided lumbosciatalgia and upper cervicothoracic pain. The X-ray allows hyperkyphosis to be measured at 85 °. There is also lumbar scoliosis of 26 °. She had an L5-S1 hernia surgery 12 years ago. Classical physiotherapy and palliative treatments are ineffective. In brace kyphosis is reduced to 55 °.
|
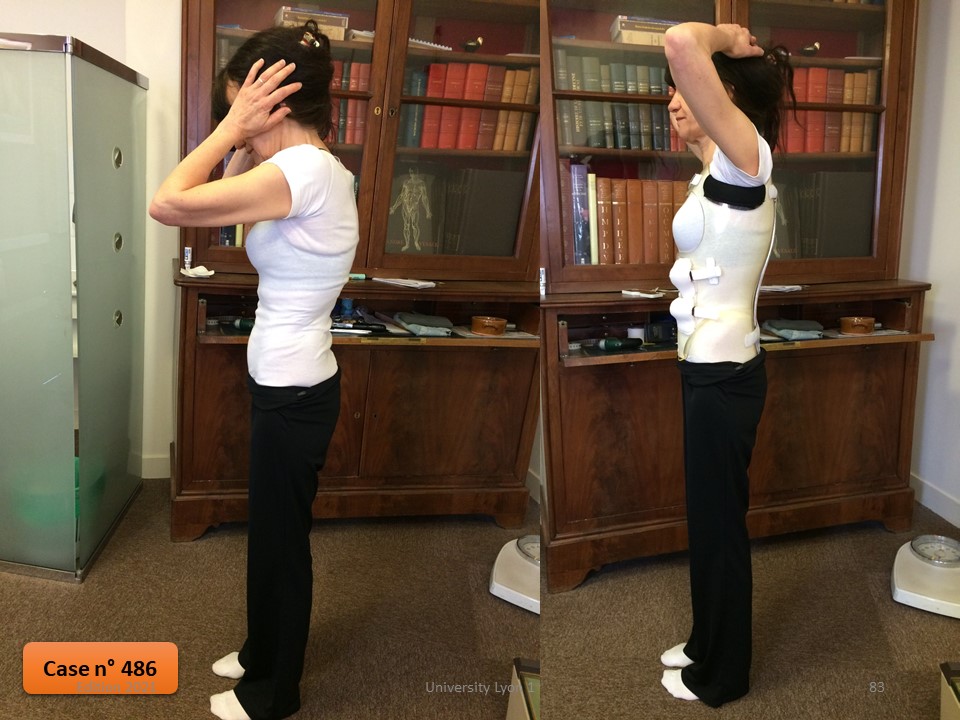 |
But above all, the lumbosacral pain disappear in one week, whereas she had suffered for 15 years. 6 months after, the angulation of kyphosis is 62 ° without race. The brace is worn for 6 to 8 hours a day, because the pain reappears when she is without brace. 2 years after, it is still worn. The angulation of kyphosis without brace is 59 ° against 85 ° at the beginning of treatment.
|
 |
This patient had been wearing a polyethylene brace for over 20 years. Despite the brace, scoliosis angulation has evolved from 27 ° to 52 ° and angulation of thoracic kyphosis is 70 °. Wishing to be more sustained, polycarbonate is tried. The angulation of kyphosis is reduced to 48 °.
|
 |
The in-brace correction of is 52 ° to 30 °. At 6 months, the brace is worn for 8 hours a day and the patient feels better than in the old polyethylene brace. At 2 years, she can not stay without the brace. The angulation of scoliosis without brace is 40 °.
|
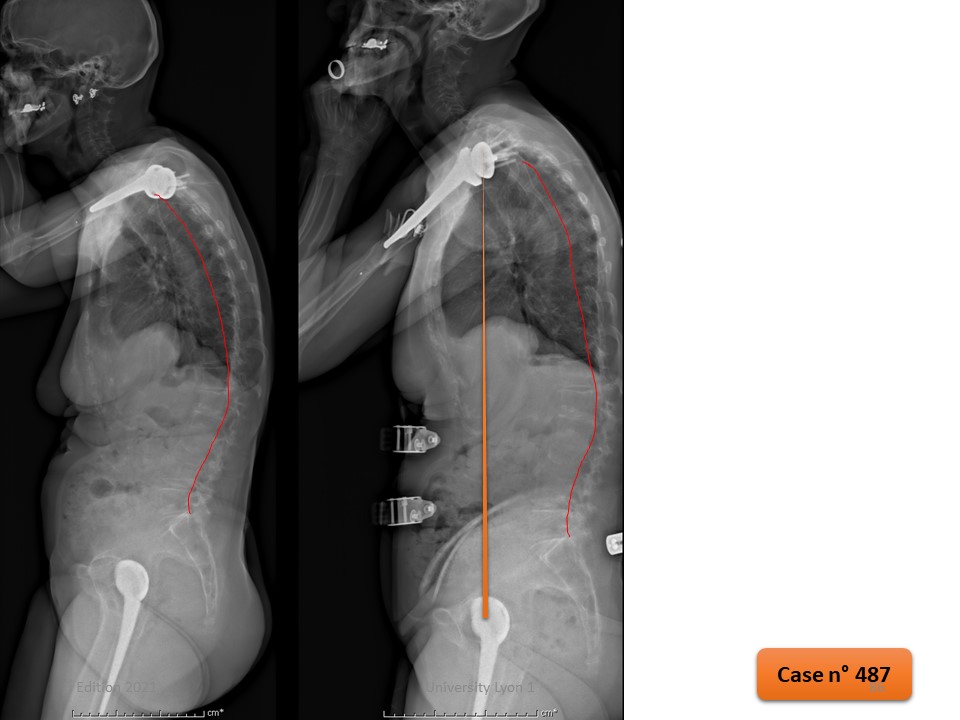 |
The correction of kyphosis is maintained with an angulation measured at 40 ° and a disappearance of the forward projection of the neck.
|
 |
This patient had Adolescent Idiopathic Scoliosis treated with Chêneau brace. Surgery is evoked at the age of 17 years. No problem until the age of 58 when she consults for pain, loss of height and greater fatigability. Scoliosis T5-T12 was 80 ° and T12-L4 60 °. A polyethylene brace worn for 2 years stabilizes the angulation of scoliosis, but thoraco-lumbar kyphosis continues to increase.
|
 |
A polyethylene brace worn for 2 years stabilizes the angulation of scoliosis, but thoraco-lumbar kyphosis continues to increase.
|
 |
In brace, the patient no longer feels the impression of trunk rotation. She can go up the 3 floors without difficulty.
|
 |
In the sagittal plane, thoraco-lumbar kyphosis is well corrected. At 2 years follow up, the patient reports that she can walk again without difficulty.
|
 |
In Conclusion, the new Lyon adult ARTbrace results from the technological evolution, but especially from the fantastic research work carried out during the last 15 years within the SOSORT. In addition to the technicality of the orthotist, thank the physiotherapist permanently encouraging the child and potentiating the results of the brace.
|
 |

To register for Certification, please contact SSOL

|
")
")
")
")
")