 |
|
 |
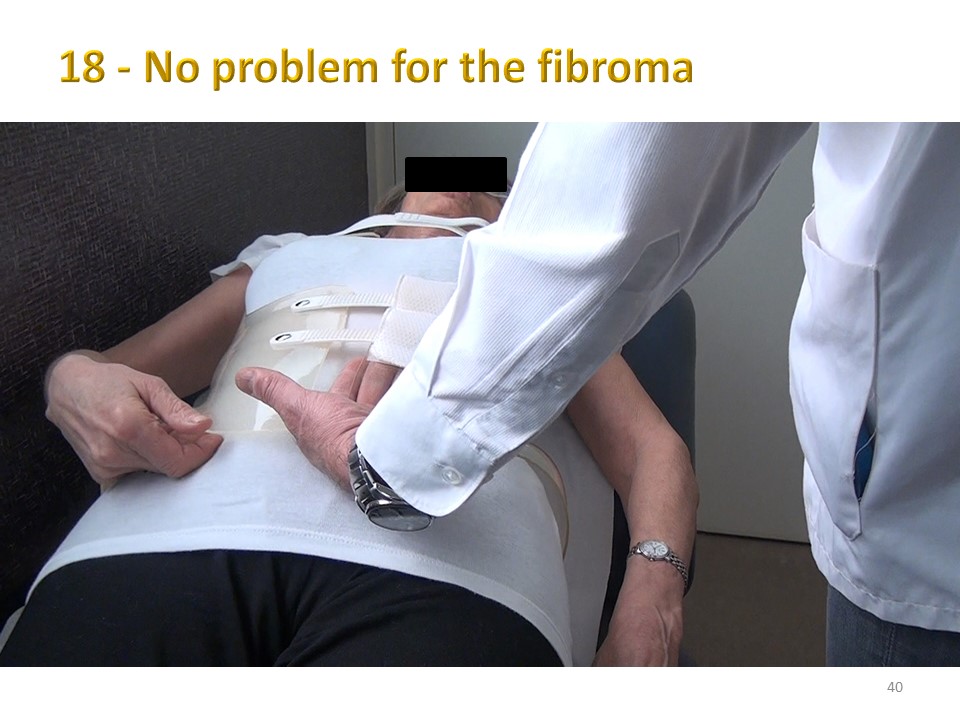
For the most important curvatures of more than 30°, we recommend a fitting independent of the delivery of the brace. This step is important for an optimal fit of the ARTbrace.
|
 |
In France, we usually give the patient T-shirts without side seams. We must insist on the necessity to wash them once in the machine to avoid allergy to fabric preservatives.
|
 |
Otherwise, this type of reaction is classic and fortunately quickly resolved with antihistamine treatment.
|
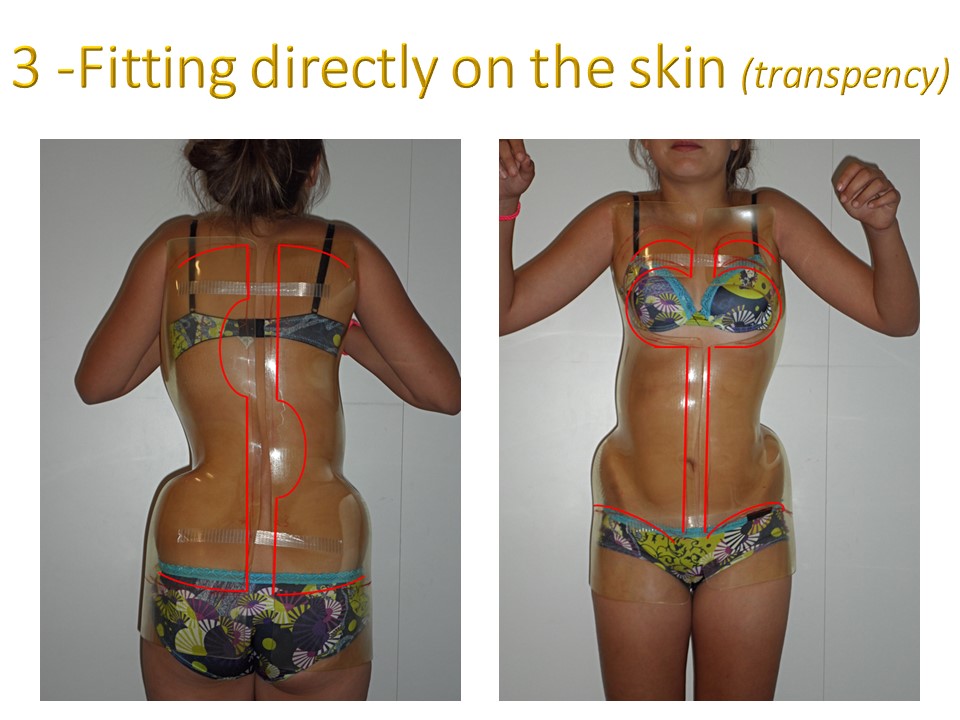 |
The fitting is done on bare skin, taking advantage of the transparency of the brace to balance the pressure on the skin in the whiter areas.
|
 |
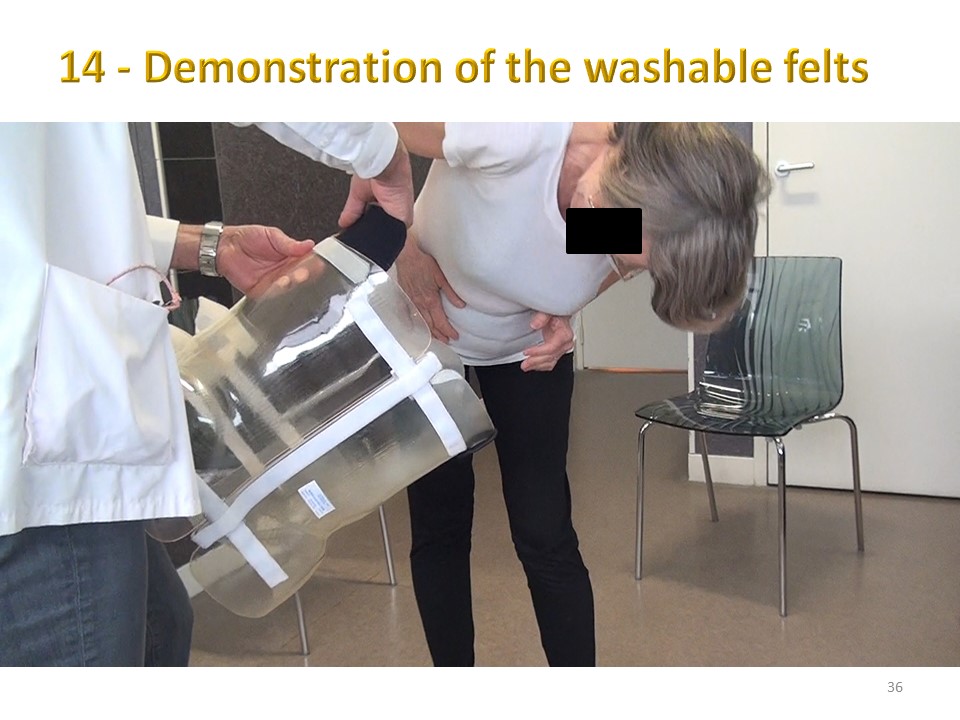
For reasons of discretion, we have recorded this sequence with jersey. The two hemi-valves are placed on the hips and stabilized under the armpits.
|
 |
The two hemi-valves are then gradually brought together from bottom to top using adhesive tape;
|
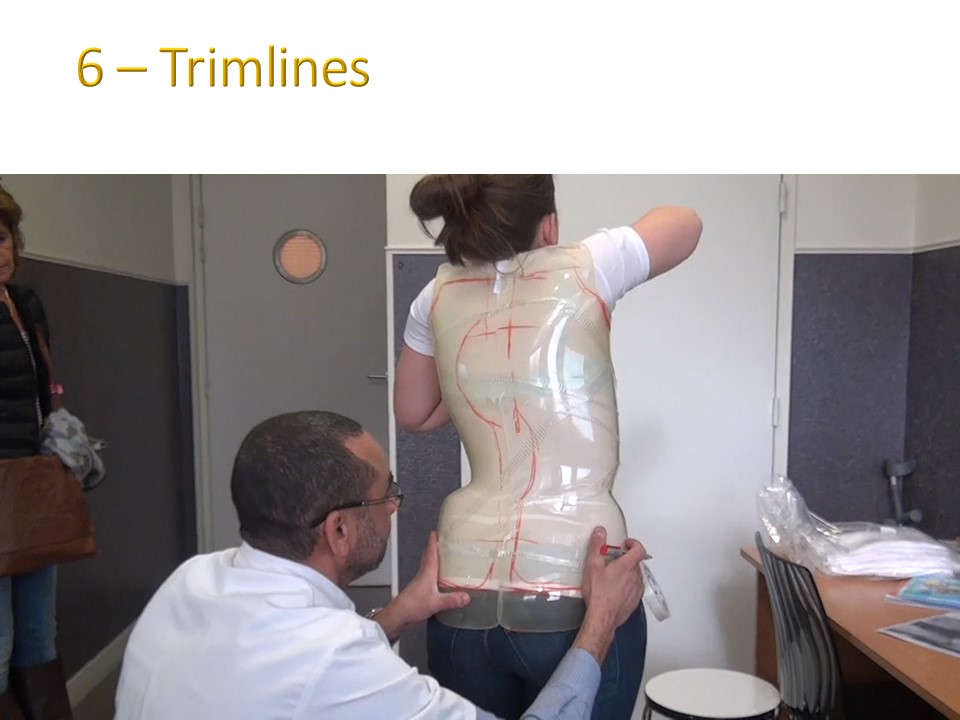 |
When the maximum tightening is obtained, the trim-lines are drawn with a grease pencil on the Europlex'O
|
 |
A large cut is made at the breast.
|
 |
At the front, the space between the two valves is about 2 cm. Overlapping of the valves is not a problem, but a larger gap is often not well tolerated.
|
 |
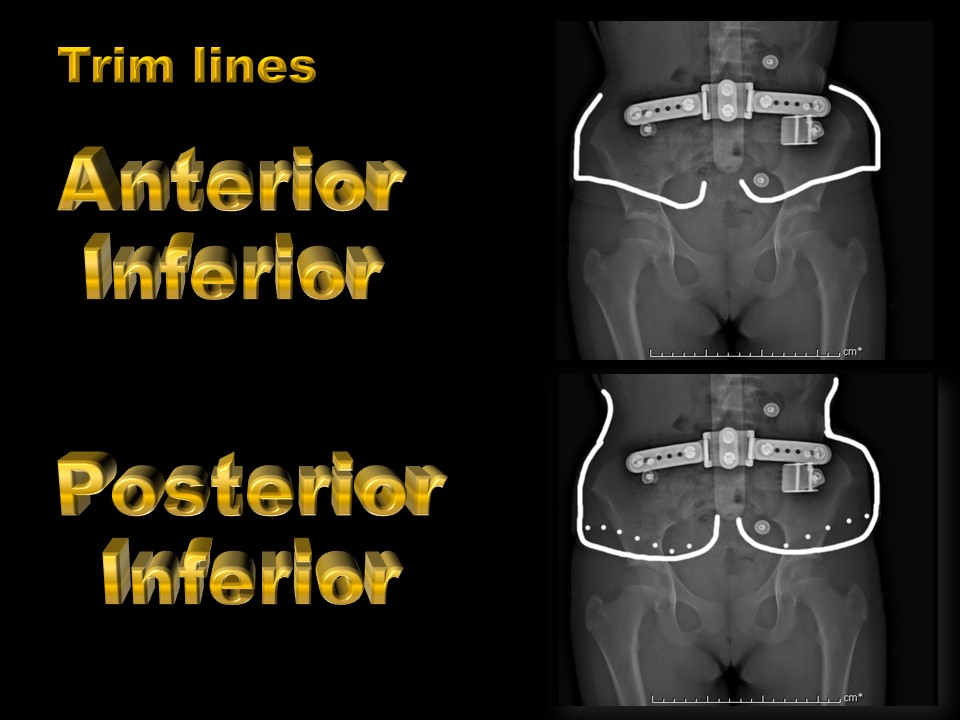
The lower cut is made approximately 2 cm below the anterior superior iliac spine, allowing a 90° hip flexion.
|
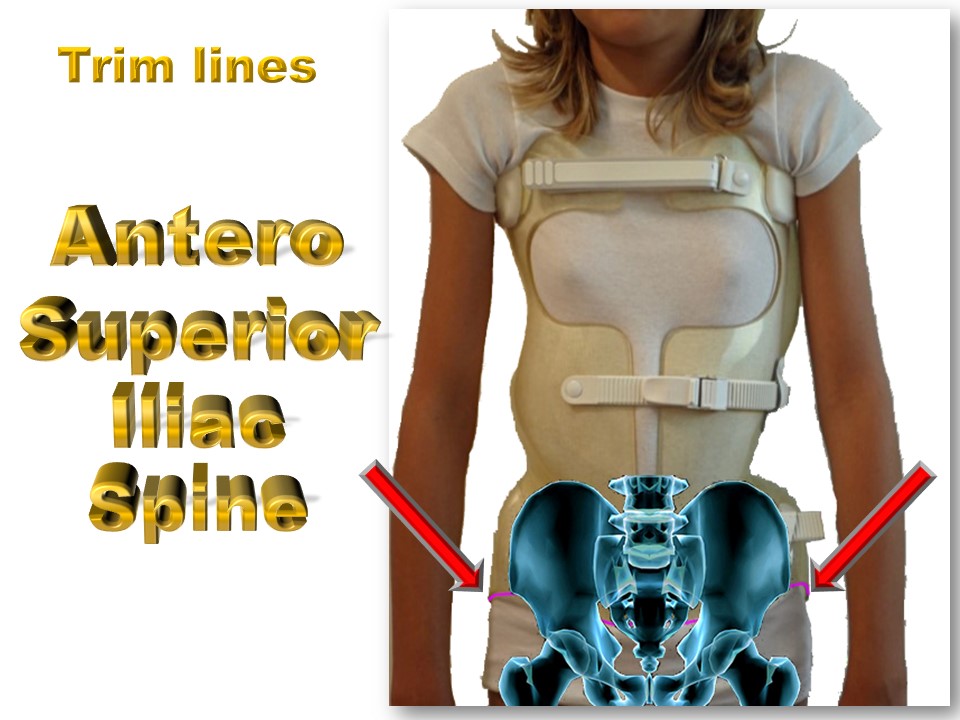 |
On this radiological superimposition, mobility is perfect at the level of the acetabular cavity.
|
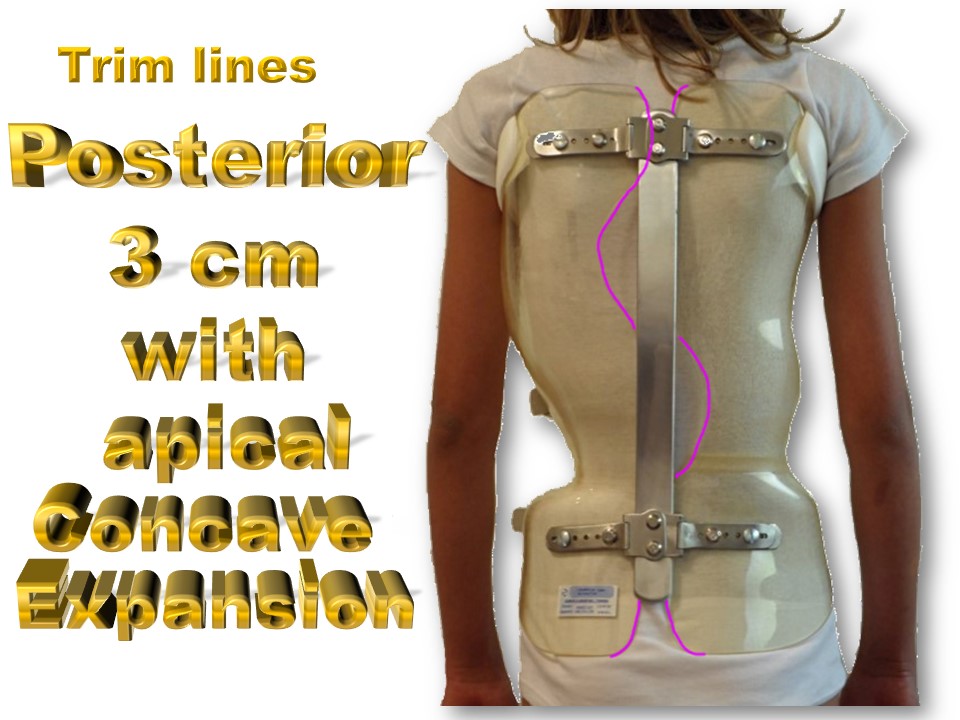 |
At the back, the spacing is about 3 cm under the rear metal bar for easy opening. The trim line is not straight, but curved into the concavity, which may facilitate untwisting. In the Lyon method, the detorsion is more in the concavity than in the convexity, which has the advantage of favouring thoracic kyphosis in the case of a flat back.
|
 |
The lower trimline is tangent to the roof of the acetabulum, lower than at the front for good control of the pelvic version. In the sitting position, a gap of 5 to 10 cm is usual between the lower end of the brace and the chair.
|
 |
With EOS X-rays, the contour of the Europlex'O is visible and allows excellent control.
|
 |
The upper extremity is much higher than in the old Lyon brace, which favours the control of kyphosis and allows the management of the high thoracic counter-curvature.
|
 |
In children, the under-axillary tilt is about 20° from low front to high back. The inclination is reversed in adults, with the posterosuperior cutting being lower at the apex of kyphosis.
|
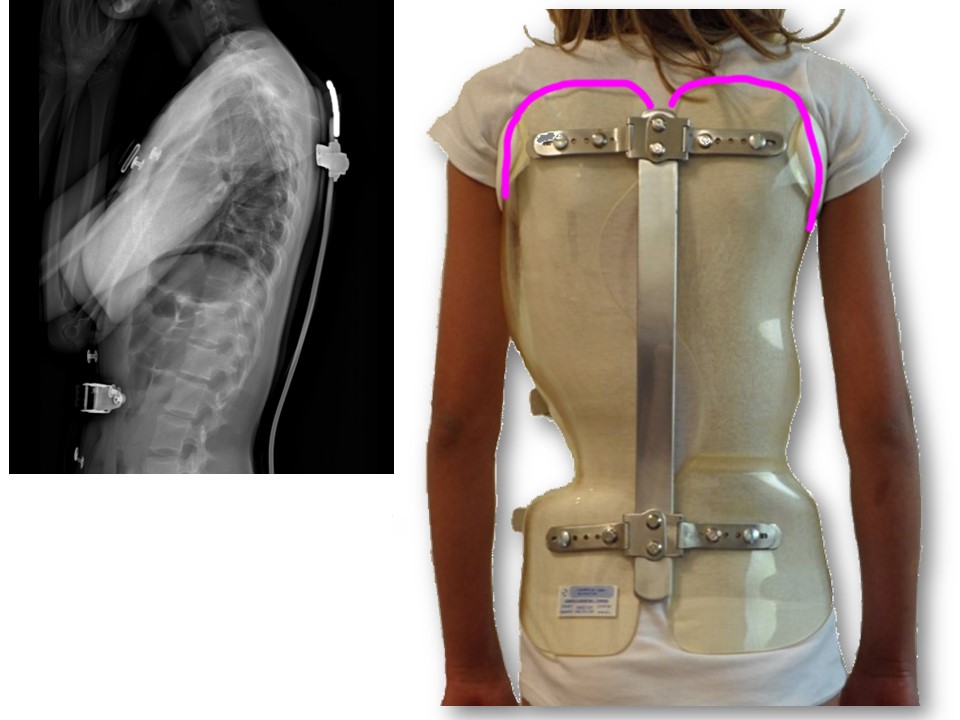 |
Initially, despite the curvature of the posterior metal bar in the direction of the kyphosis, a median rigidity at the level of the scoliosis is noted, on the other hand the high thoracic curvature has a satisfactory kyphotic curvature.
|
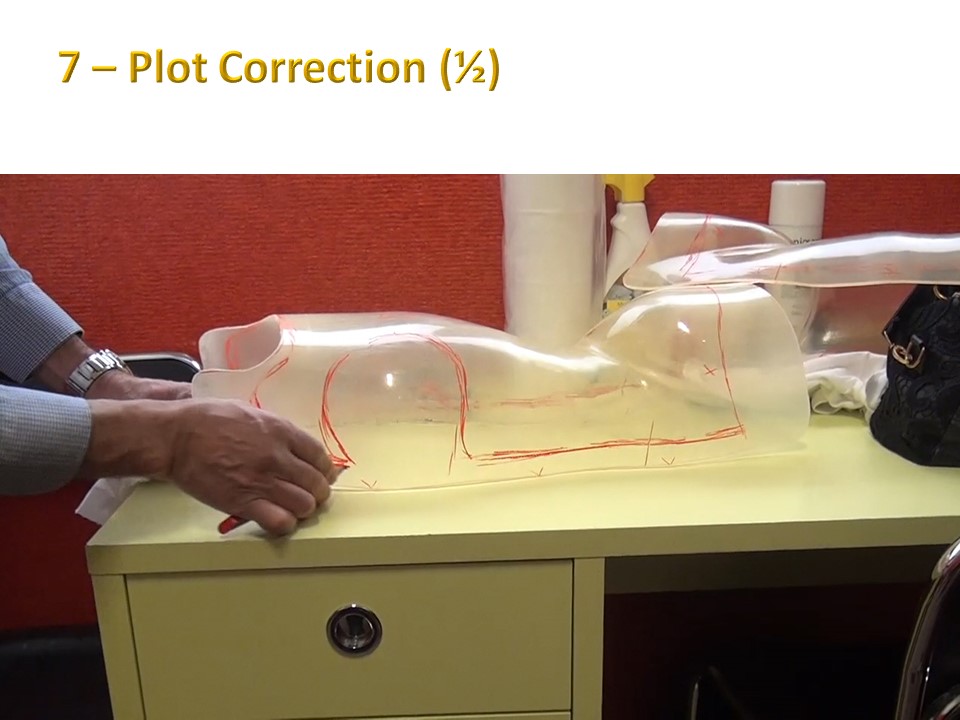 |
The two hemi-valves are then removed and the horizontality with respect to the plane of the table is checked.
|
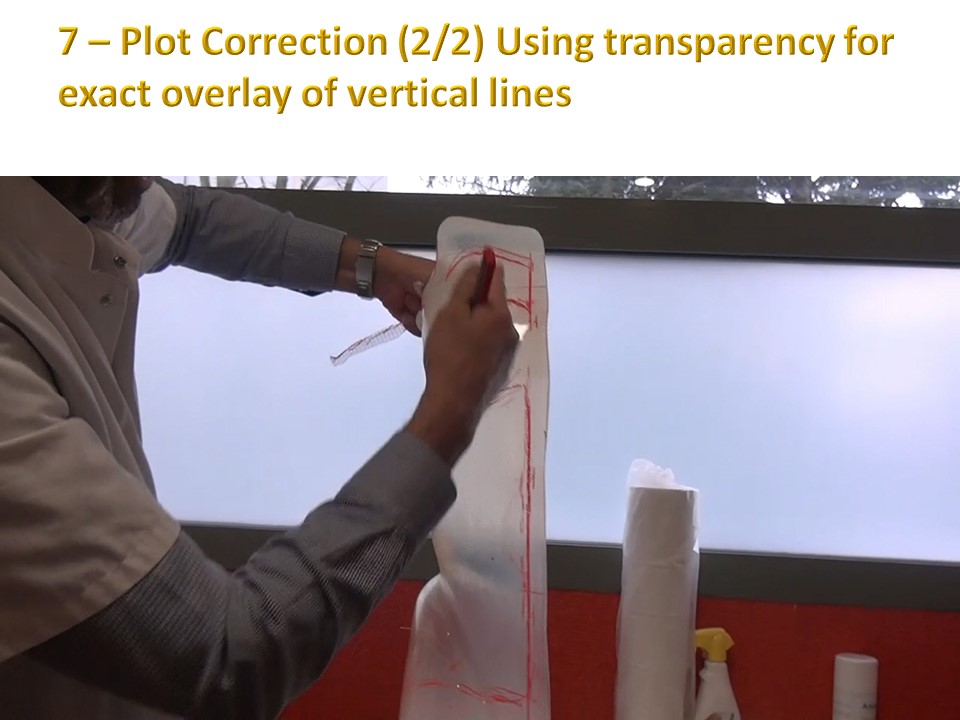 |
The transparency of the plastic allows simultaneous visualization of the anterior and posterior trim-lines.
|
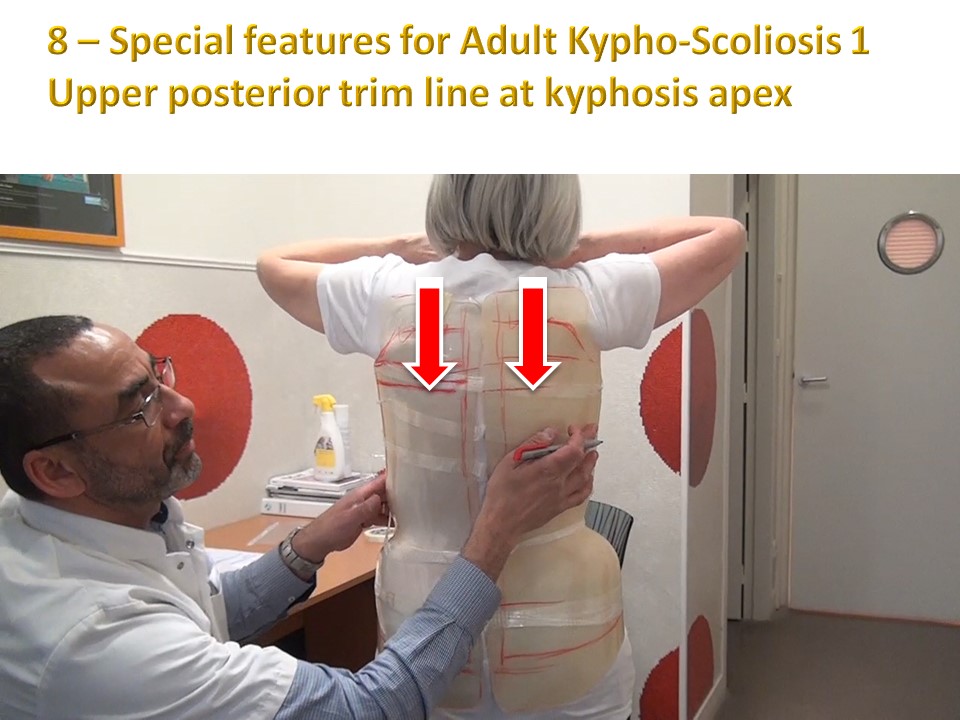 |
In this adult patient, we see the posterior cut-out much lower than in the child because of the hyperkyphosis.
|
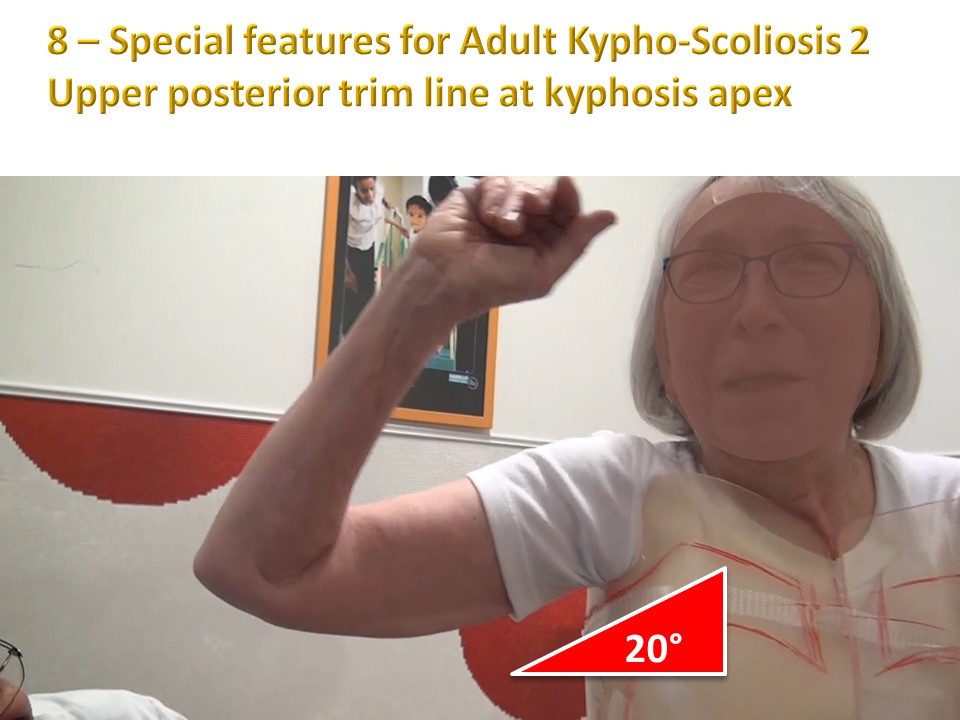 |
In this case, the anterior part will be higher than the posterior part, with an inclination of 20° from high front tolow back.
|
 |
The day after the fitting, the brace is delivered to the patient, assembled, but the finishing touches are not yet applied. The date is usually at the weekend so that the patient can test at home.
|
 |
The brace is presented to the patient with the anterior rack-and-pinion closures.
|
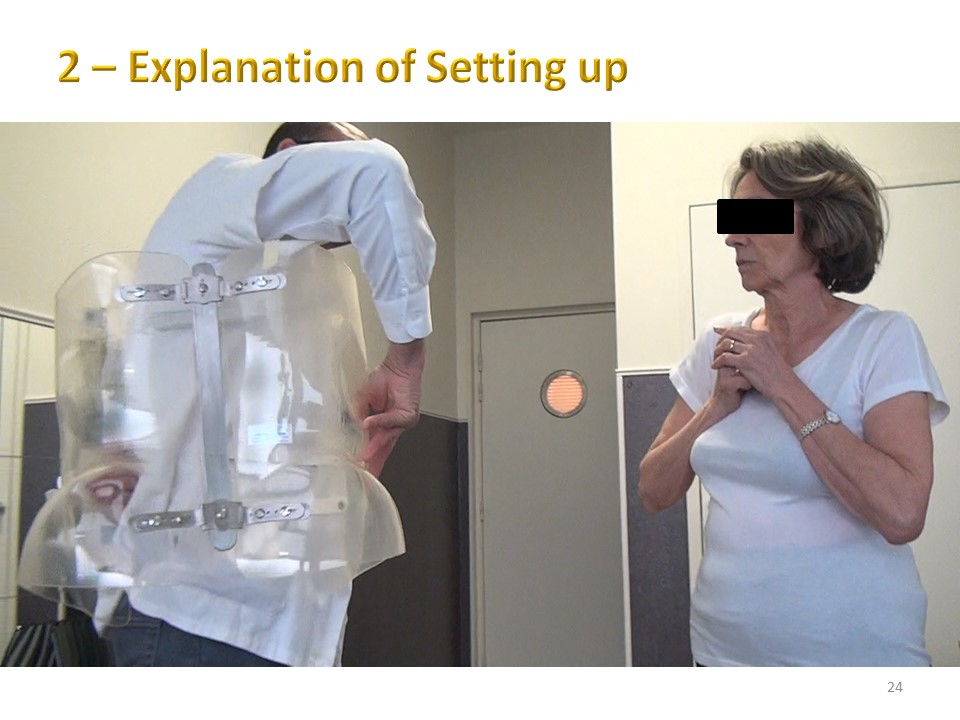 |
The orthotist is going to show on himself, the setting of the brace which opens like a book.
|
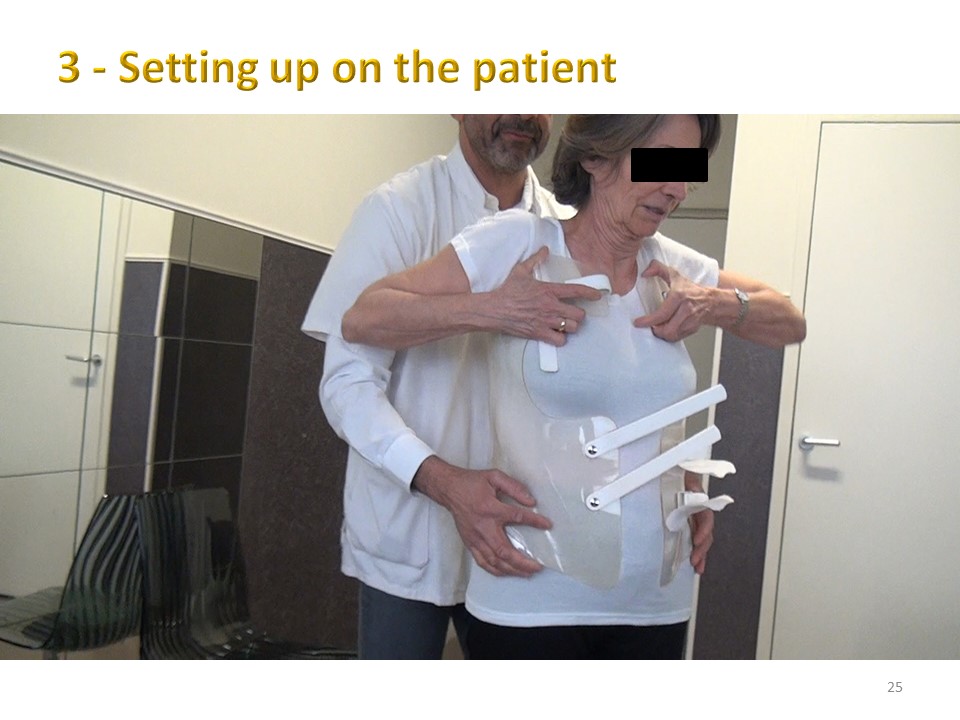 |
Then he's going to put it on the patient, asking her to shrug her shoulders a little.
|
 |
The final positioning will take place in the lying position, which is much more precise than the standing position. The patient is more relaxed.
|
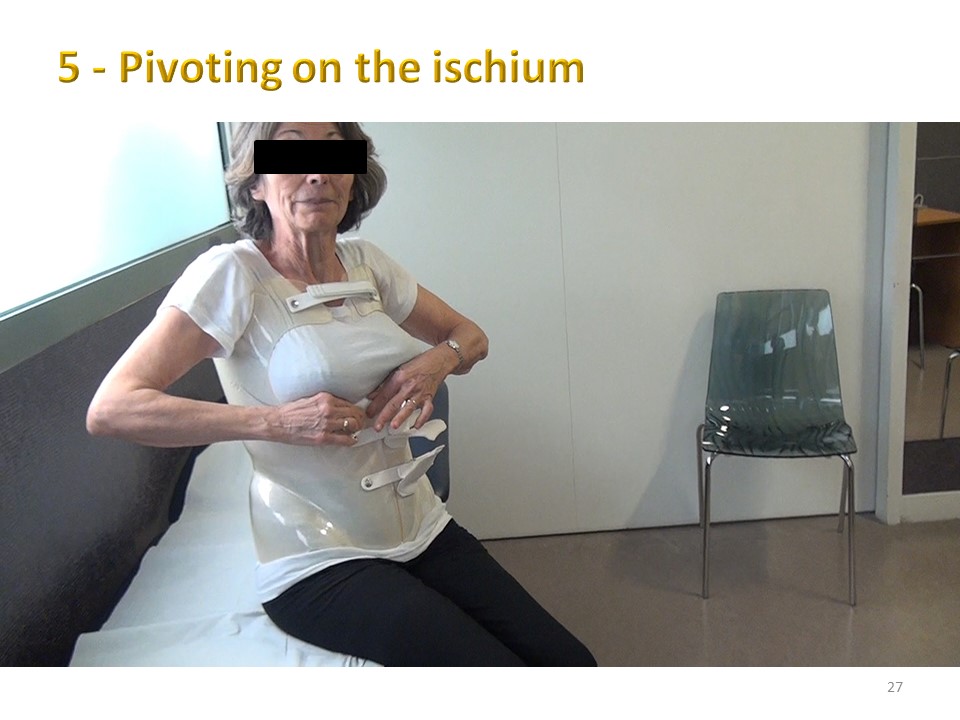 |
She then moves from the decubitus to the sitting position, and we take the opportunity to explain to her how to perform this transfer by pivoting on the ischium. The patient helps herself with the upper limbs and the lower limbs play the role of a pendulum.
|
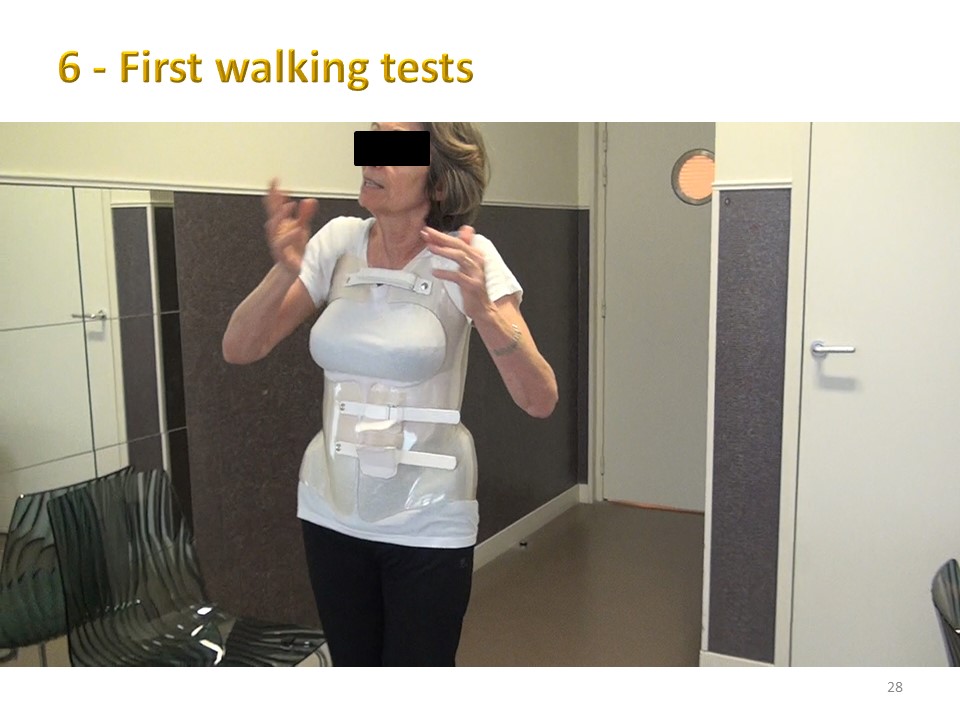 |
She will then carry out the first tests while walking, which allows her to control her balance.
|
 |
Spontaneously the patient tries to get out of her brace by alternately shrugging one shoulder to the right and then to the left like a duck dance.
|
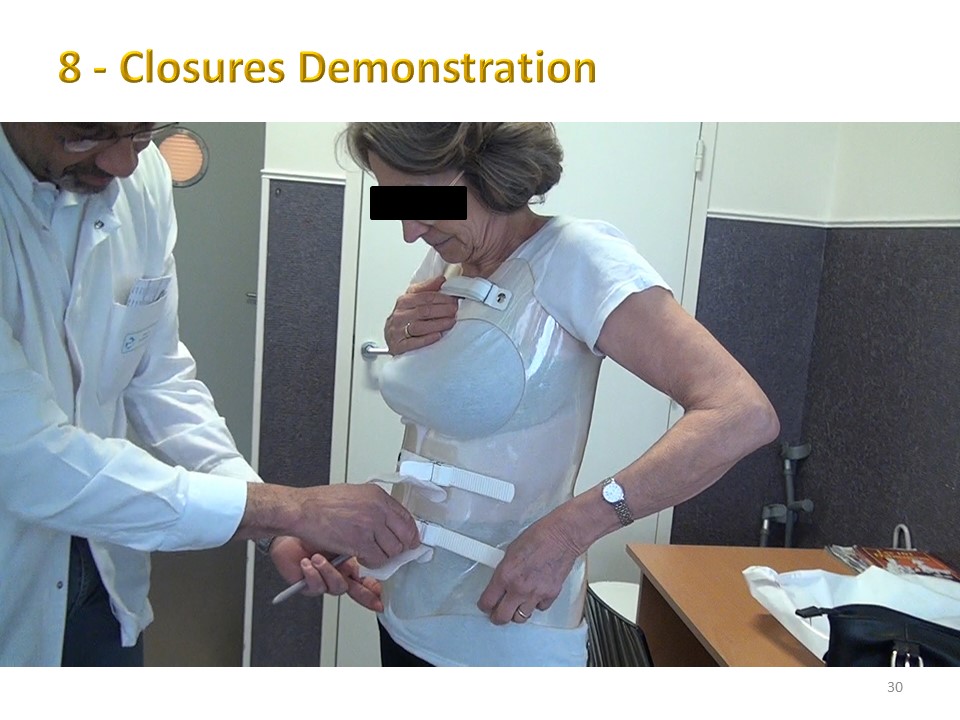 |
The orthotist then shows how to use the rack and pinion closures which are identical to those used for ski boots.
|
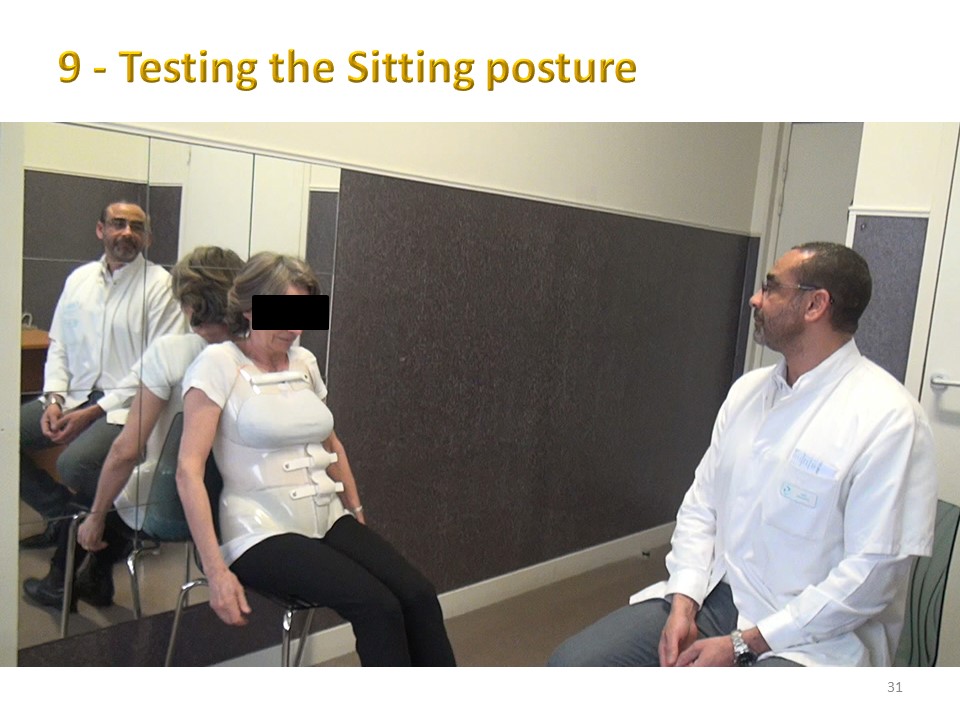 |
Then the sitting position on a chair is tested starting with a trunk/thigh angle of 120°. During this test patients often ask for an additional cut-out and it should be explained to them that this cut-out will possibly be made after the X-ray check-up on the following Monday.
|
 |
The brace is then removed for the first finishing touches.
|
 |
Cutting is carried out using a jigsaw with a special Bosch T101 blade.
|
 |
Particular attention is paid to the under-axillary region due to the "pull-baby lift" effect of the brace. The black protections are detachable and washable.
|
 |
The metal parts are also protected by an adhesive that prevents the patient's clothing from coming into contact with the metal edge.
|
 |
The orthotist demonstrates the removability of the sub axillary pads.
|
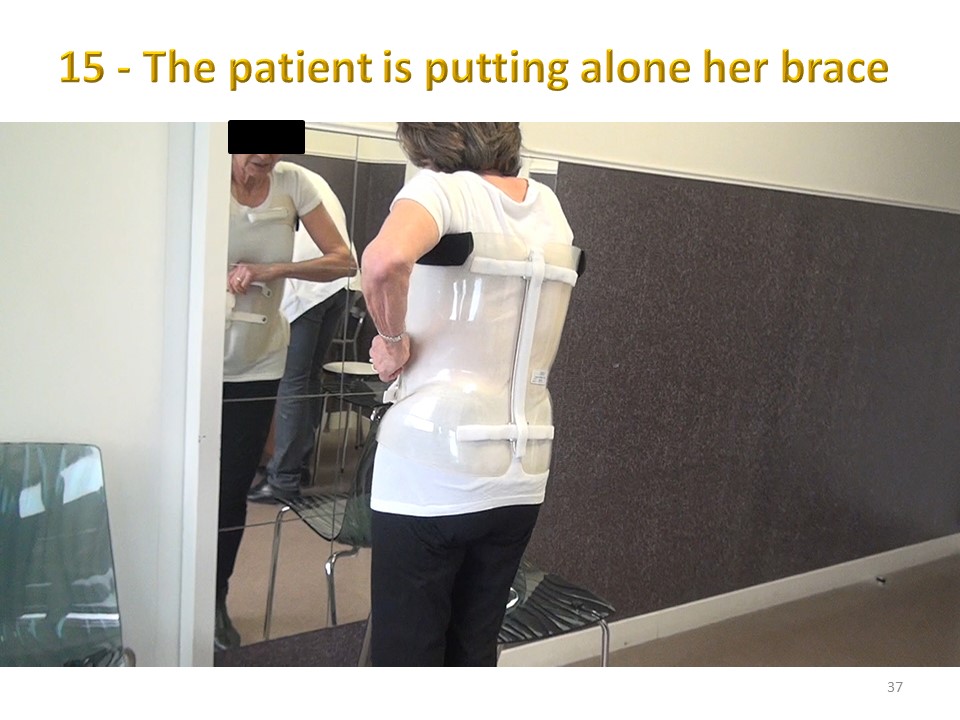 |
The patient will fit the brace by herself.
|
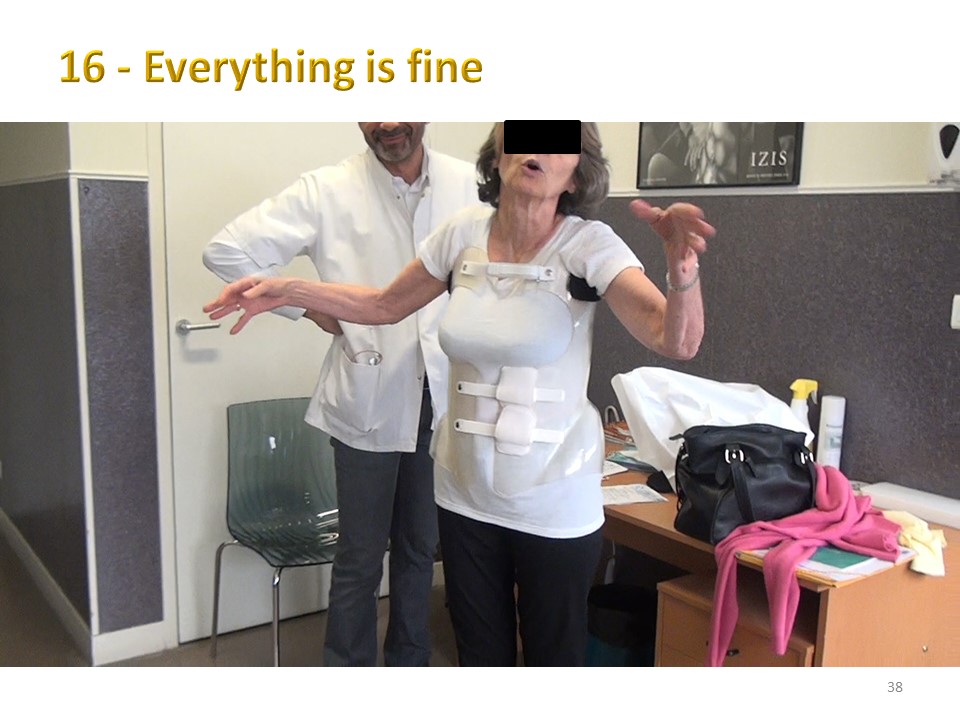 |
Looks like everything's okay.
|
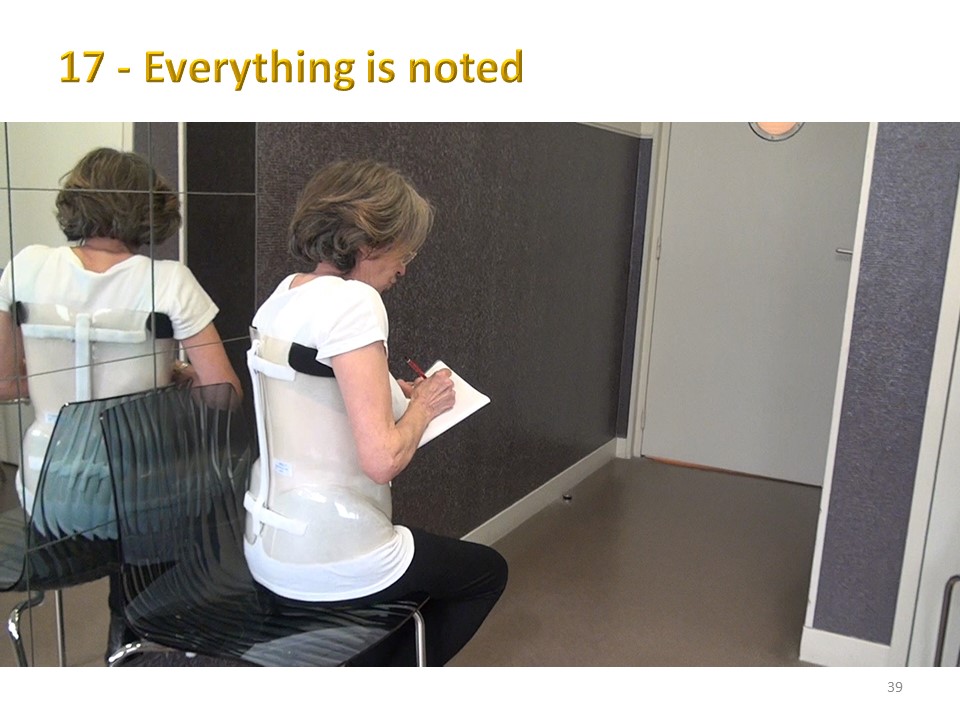 |
As a teacher, she writes down all the details in her notebook.
|
 |
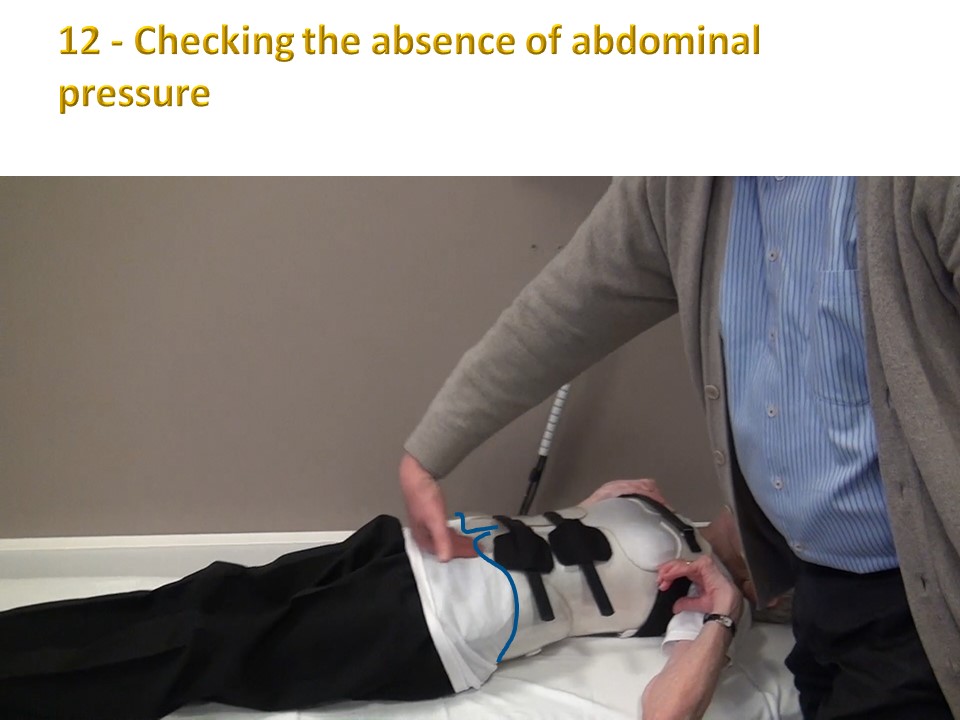
While lying down, she realizes the absence of abdominal compression due to the lordosis moulding. There is usually a space of two to three centimetres between the plastic and the skin.
|
 |
She then completes the final delivery document for the brace.
|
 |
Even at the age of 94, it is possible to make a brace as long as the reducibility is good and the upper limbs allow patients to straighten up. The upper limb strengthening is specific to these scoliosis at risk of brace. The fontal balance is improved.
|
 |
And in the sagittal plane, the hip flexion decreases. In conclusion, the management of adult patients remains possible despite the rigidity of the structures. The most important thing remains the patient's motivation.
|
 |
Due to the high rigidity, the brace check-up takes place 3 days after delivery, as it is impossible to leave the patient in a poorly fitting brace.
|
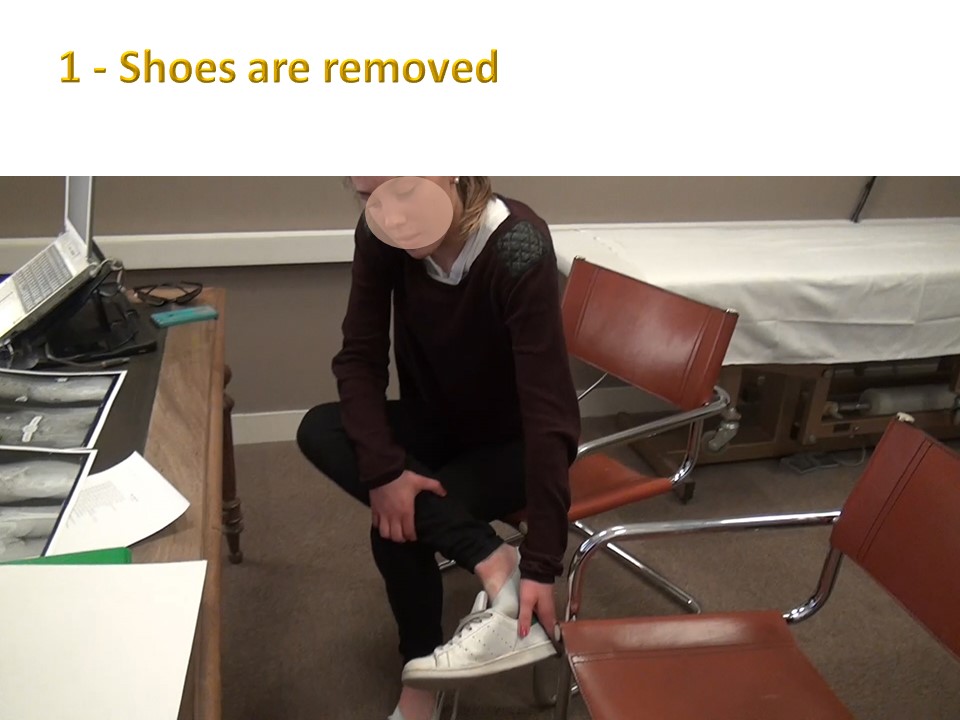 |
The first step is the removal of the shoes. The child is taught to place her leg on the opposite knee. Seats with armrests make the task more difficult, but not impossible.
|
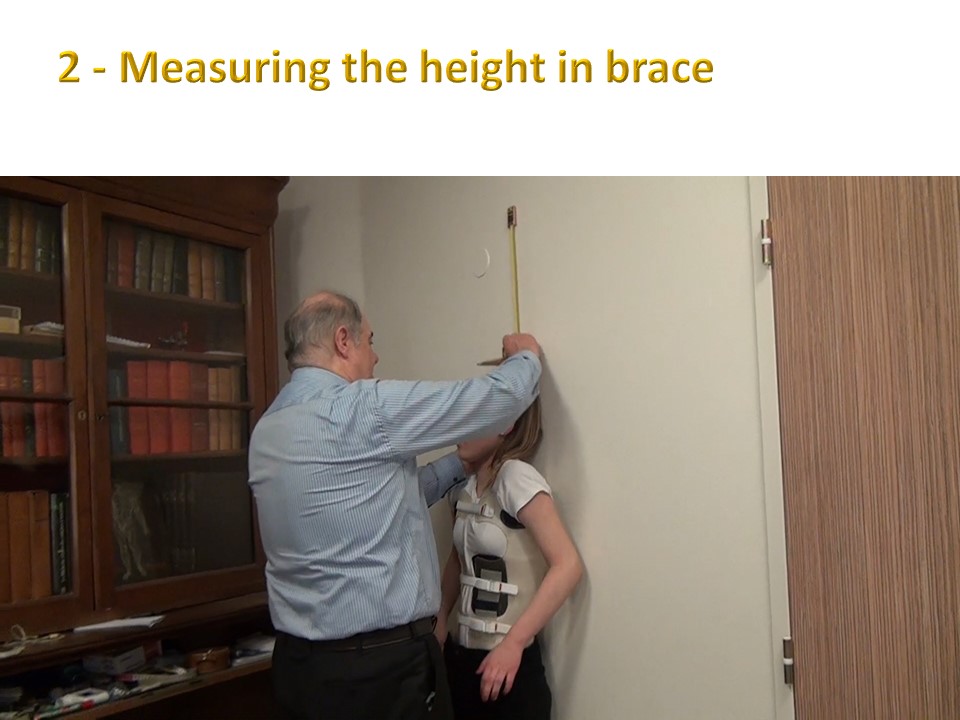 |
Height and weight are measured in the brace, which makes it possible to check the size in brace of about 1.5 cm and the weight in brace slightly over 1 kg.
|
 |
Weight variations are much less frequent than under plaster cast, which presented greater digestive risks.
|
 |
The balance of the occipital axis is measured with a plumb line, which remains a reference in the Lyon method.
|
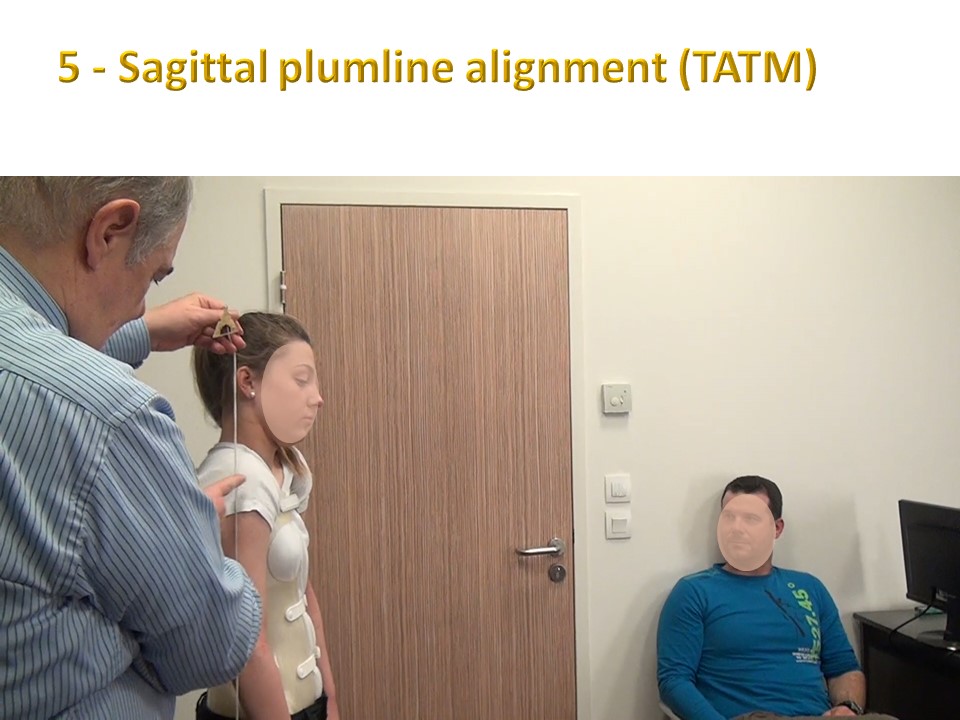 |
The measurement is carried out in the frontal plane, but also in the sagittal plane with the line Tragus-Acromion-Trochanter-Malleoli.
|
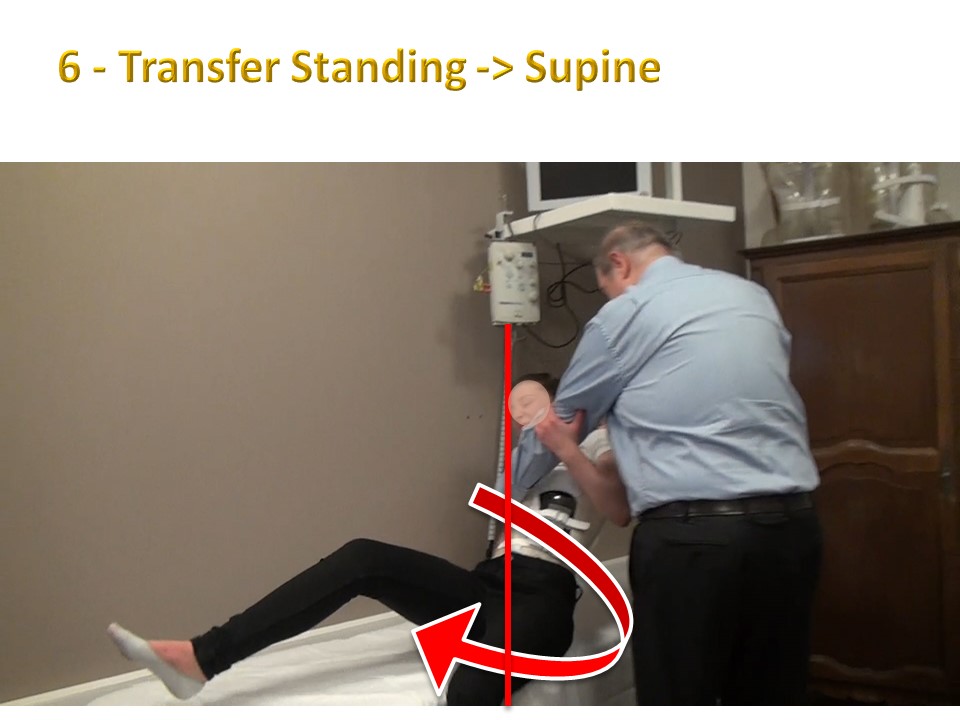 |
The transition from standing to lying down is always difficult on the first days of a brace. The child pivots on the ischium but must be helped in the transfer by supporting the brace.
|
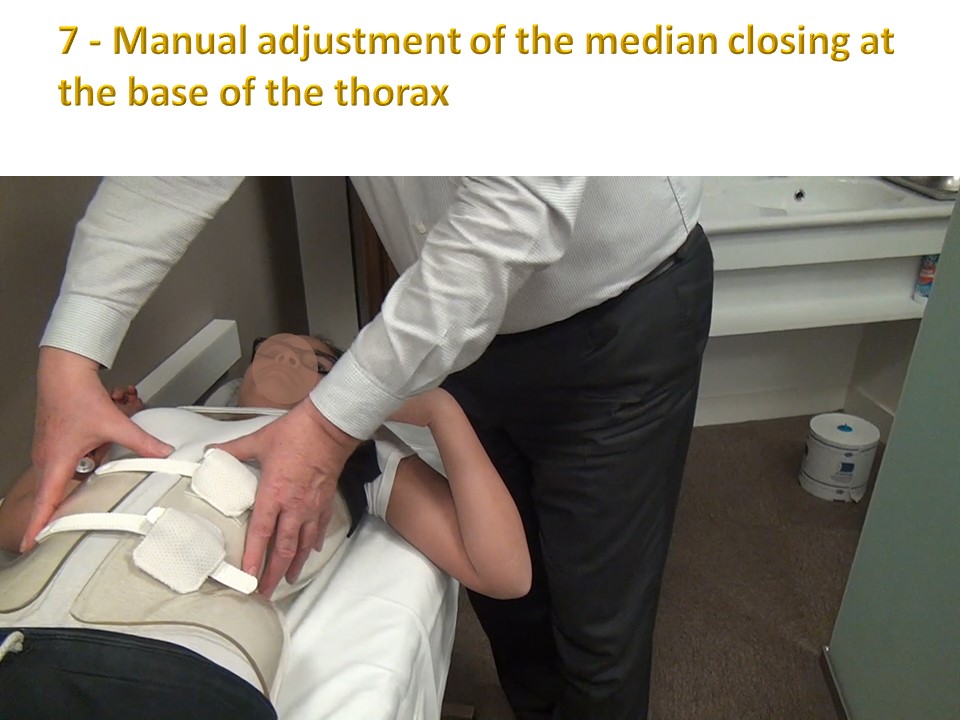 |
The final adjustment of the anterior closure is carried out and there is usually a difference of 1 to 2 centimetres from the delivery of the brace.
|
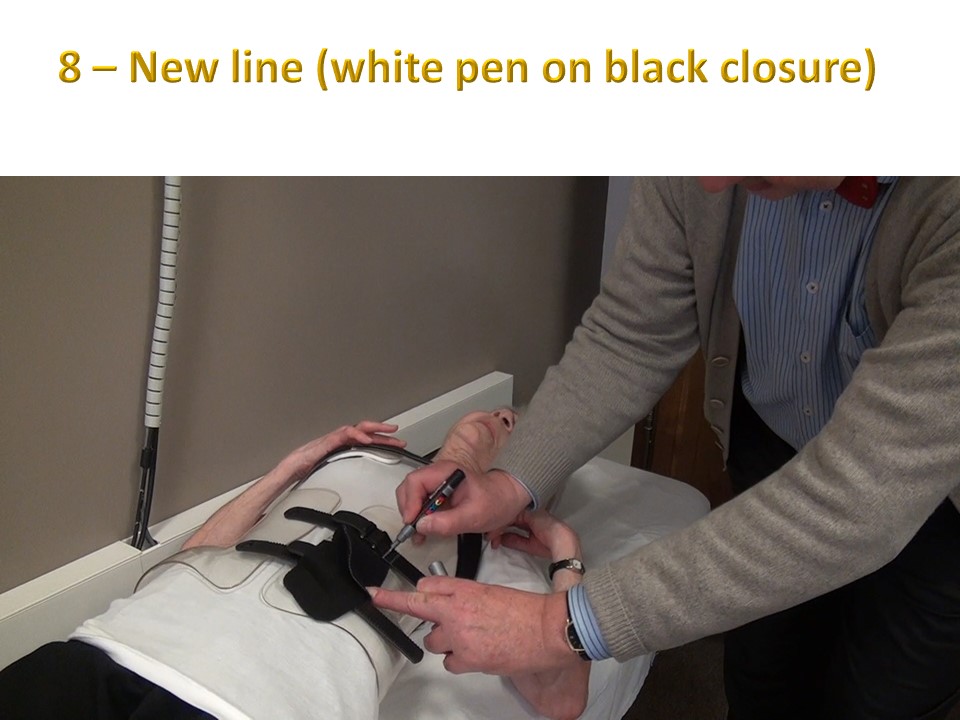 |
An indelible marker is used on both sides of the closure on the strap.
|
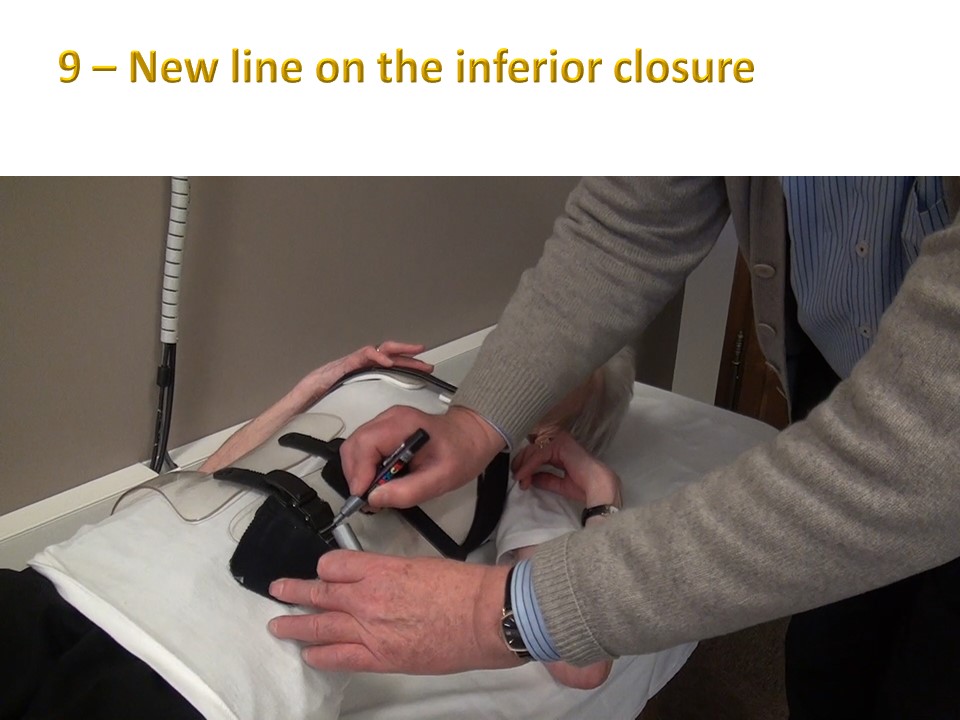 |
The most important closure is the median. The lower closure is often loosened when sitting at school or when using the toilet. Usually the anterior cuts are parallel
|
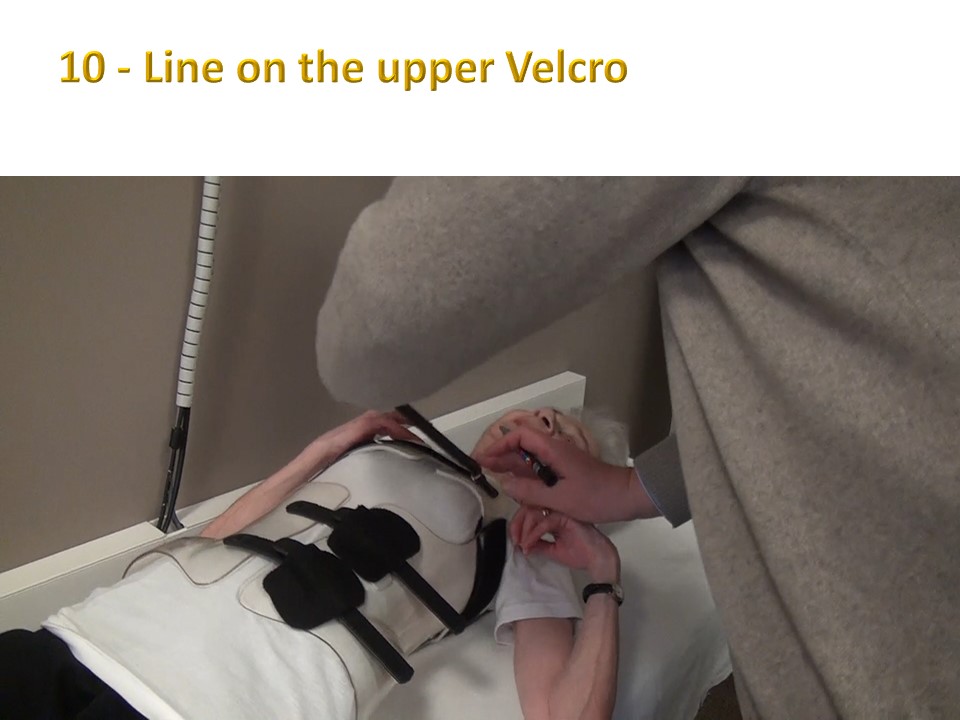 |
The upper Velcro has no particular mechanical action. It can be detached for sports.
|
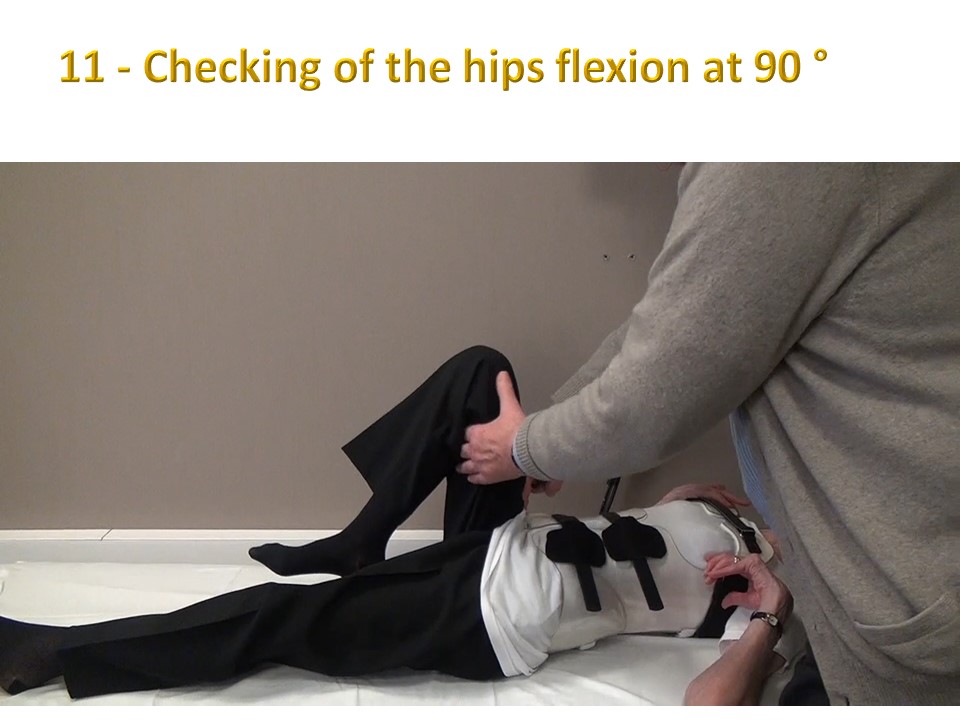 |
Hip flexion at 90° is controlled, but the patient is reminded that the 120° trunk-thigh angle is preferable in the sitting position.
|
 |
There should be no abdominal pressure when lying down, as the maintenance of the lordosis is a construction principle.
|
 |
The transfer in the opposite direction from lying down to standing will also be helped, but the grip is wider between the shoulder and the opposite thigh.
|
 |
Tightness at the under-axillary supports is checked. The doctor must be able to pass one or two phalanges between the skin and the plastic without difficulty.x
|
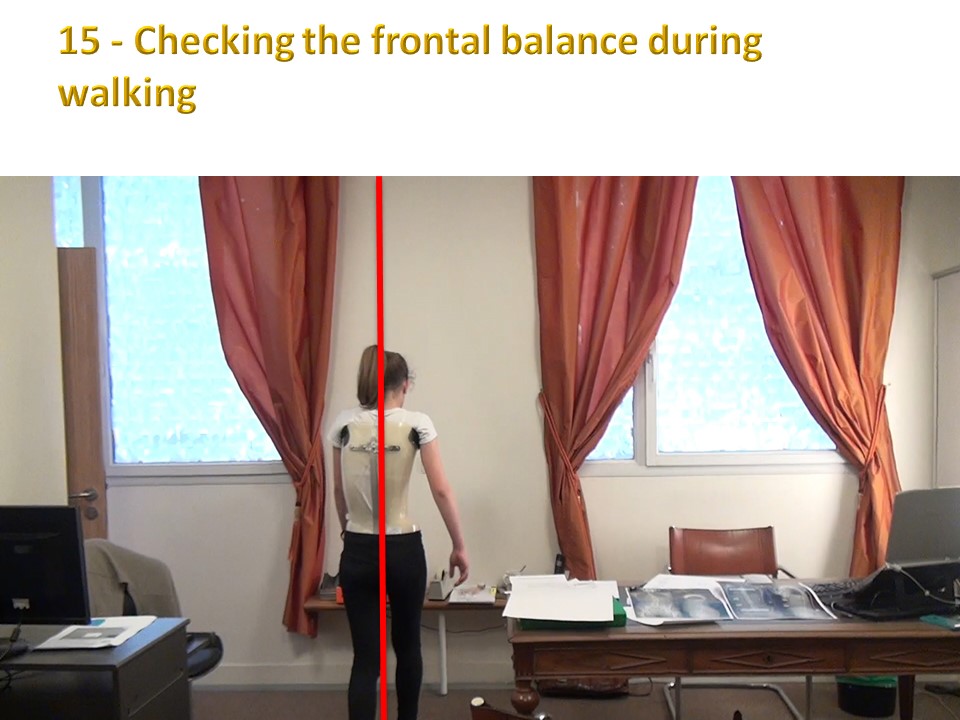 |
The child is then asked to walk to check the balances, here in the frontal plane.
|
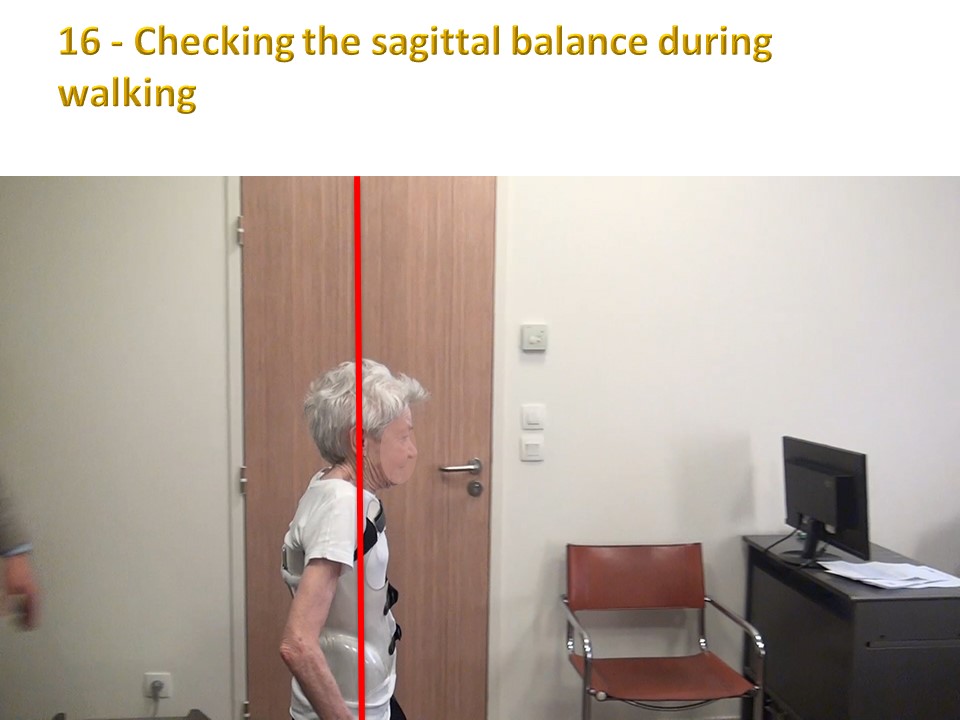 |
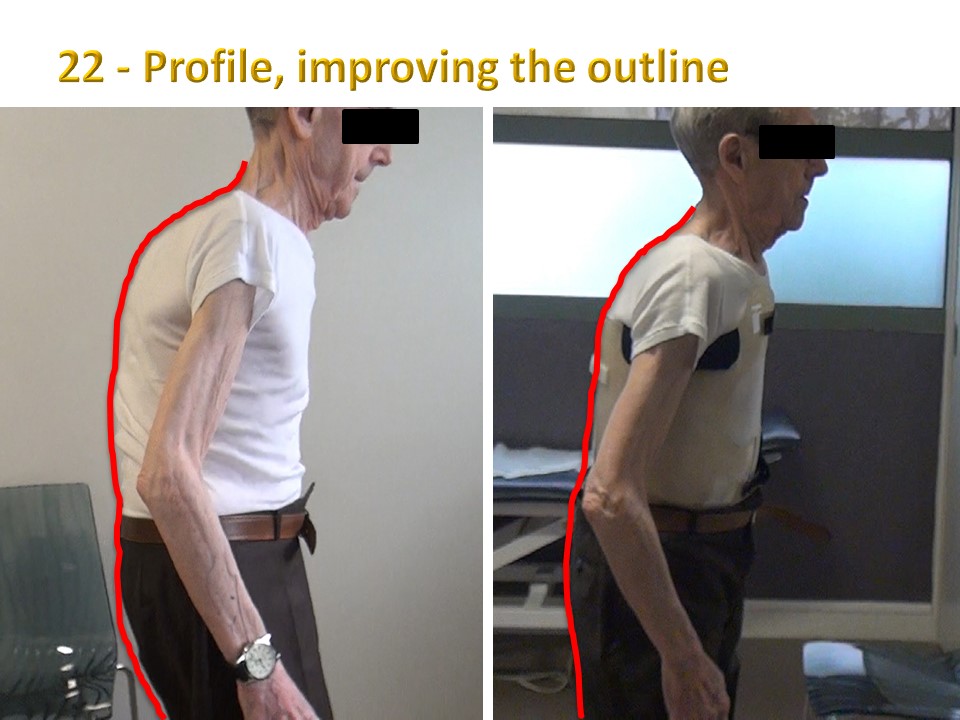
But also in the sagittal plane, especially in adults.
|
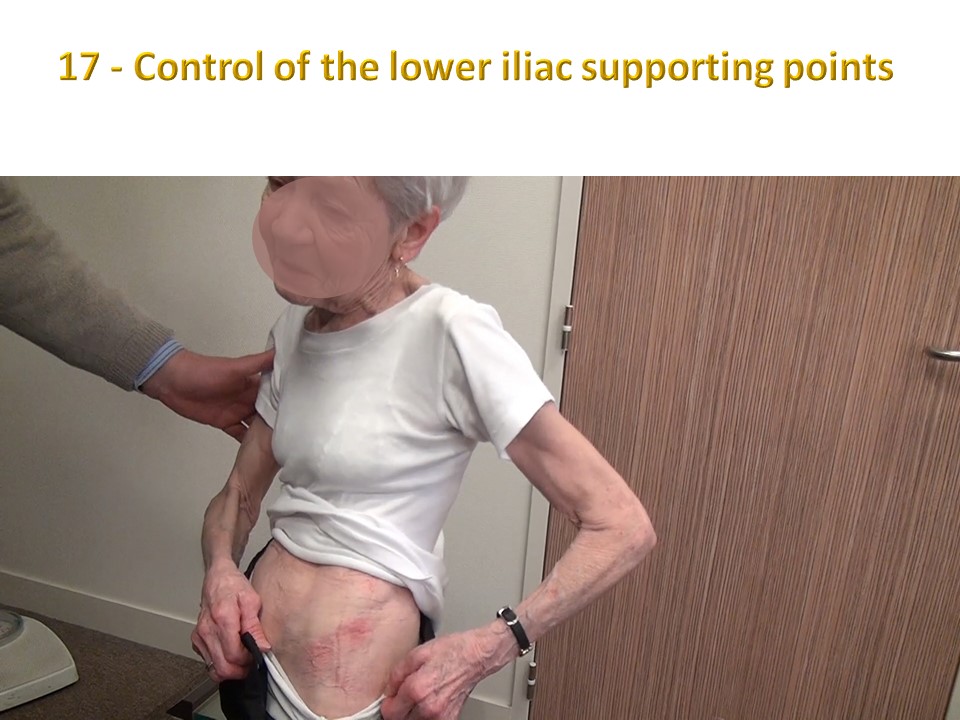 |
Redness at the level of the iliac crest is frequent in adults, especially in skinny patients for whom, it will have been advised at the time of delivery, the use of two superimposed shirts for a few days.
|
 |
The subaxillary skin here is perfect, knowing that the "pull" effect is less marked in adults.
|
 |
Vital capacity control is carried out with and without a brace. In ARTbrace, the vital capacity is only slightly reduced (7%). A low initial vital capacity is considered for physiotherapy.
|
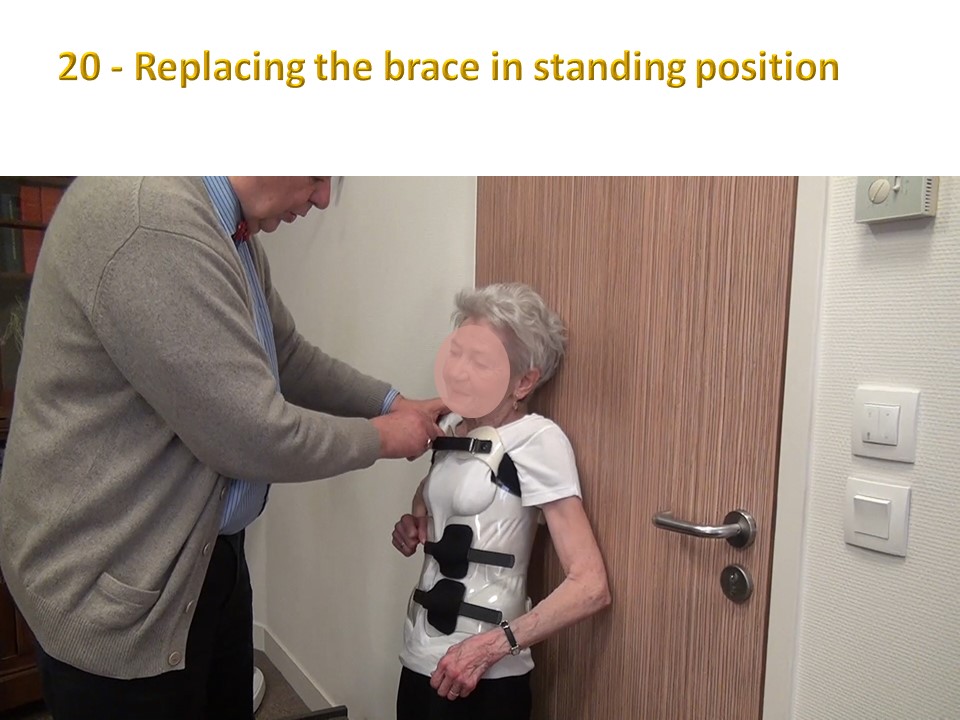 |
The brace is also put back in place while standing with the back against a wall.
|
 |
In the case of camptocormia, the brace is first positioned at pelvic level, then after straightening of the spine, closed at the level of the upper strap and finally fixed at the bottom.
|
 |
The important thing is to be well positioned in the brace. The patient can perform an active axial self-elongation to facilitate the positioning in the brace.
|
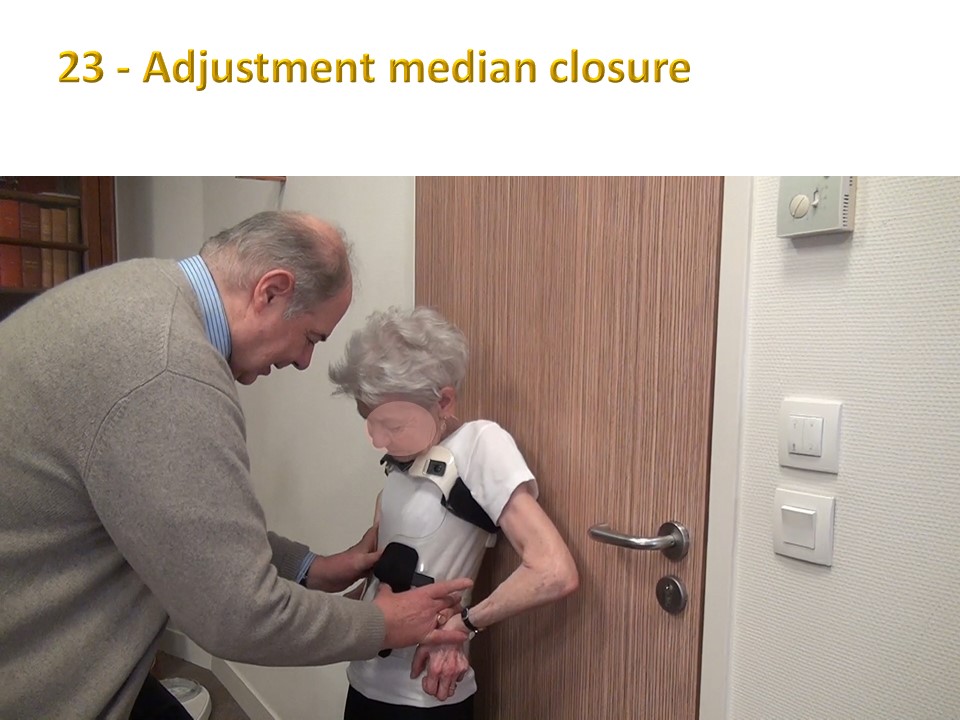 |
The middle thoraco-lumbar closure is adjusted first.
|
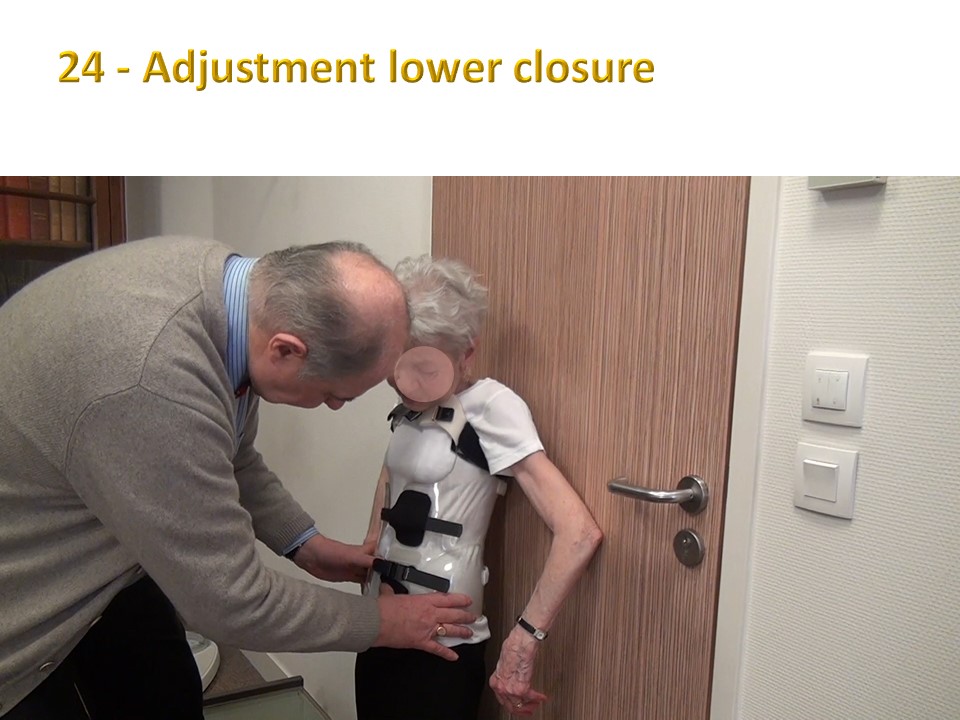 |
Then the lower closure trying to balance the pressures.
|
 |
Vital capacity is re-controlled with the brace. The best of the 3 trials is selected.
|
 |
In the sitting position, the seat-brace distance here is 10 cm, slightly above average.
|
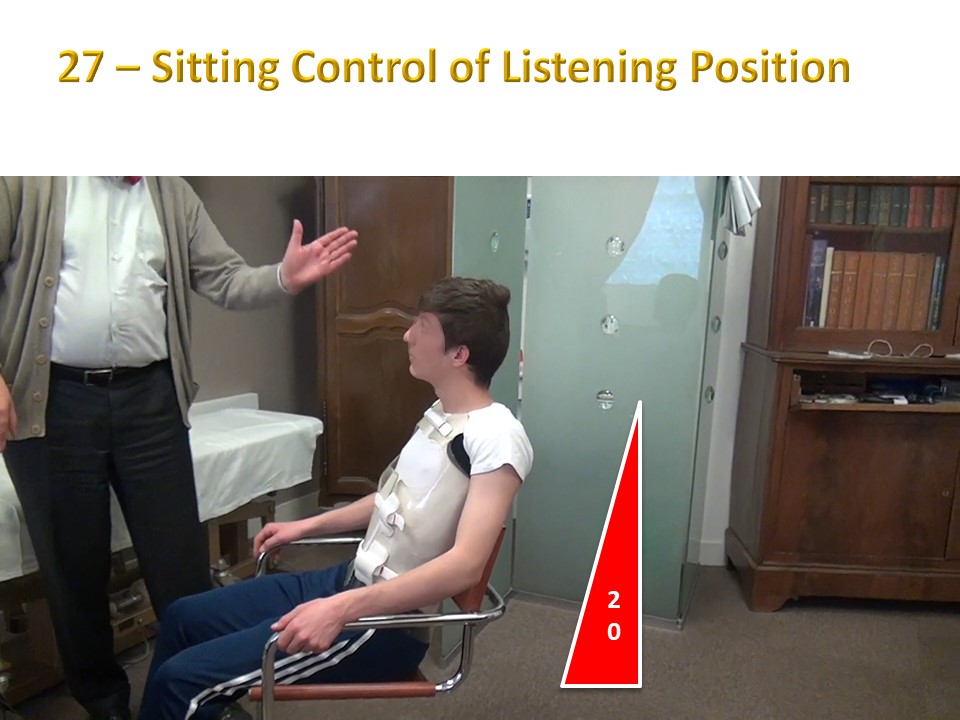 |
In the listening position, the trunk is tilted back about 20°.
|
 |
In the writing position, the trunk is tilted forward, the ischium rest on the front part of the seat, the thighs plunge forward, the feet are positioned under the chair and the forearms are on the work surface.
|
 |
Putting the shoes back on is done in the same position as removing them in external hip rotation, knee flexion at 90°, the lower part of the leg rests on the opposite knee.
|
")
")
")
")
")