 |
.
|
 |
Final results of bracing management with initial plaster cast or total time EUROPLEX O’ bracing in adolescent idiopathic scoliosis AFTER RISSER 3. Introduction. Even though experts recommend scoliosis bracing from Risser 0 to 3 to evaluate the results of a brace, no scientific reference indicates a time limit for bracing idiopathic adolescent scoliosis. Long before Richards, the Lyon brace was used after Risser 2. In fact, in cases of painful scoliosis, late progression despite physiotherapy or surgical indication not accepted by parents, an attempt by bracing seemed legitimate. It is therefore interesting to study the results of these treatments which we call "braking bracing".
|
 |
The authors have no disclosure for this presentation.
|
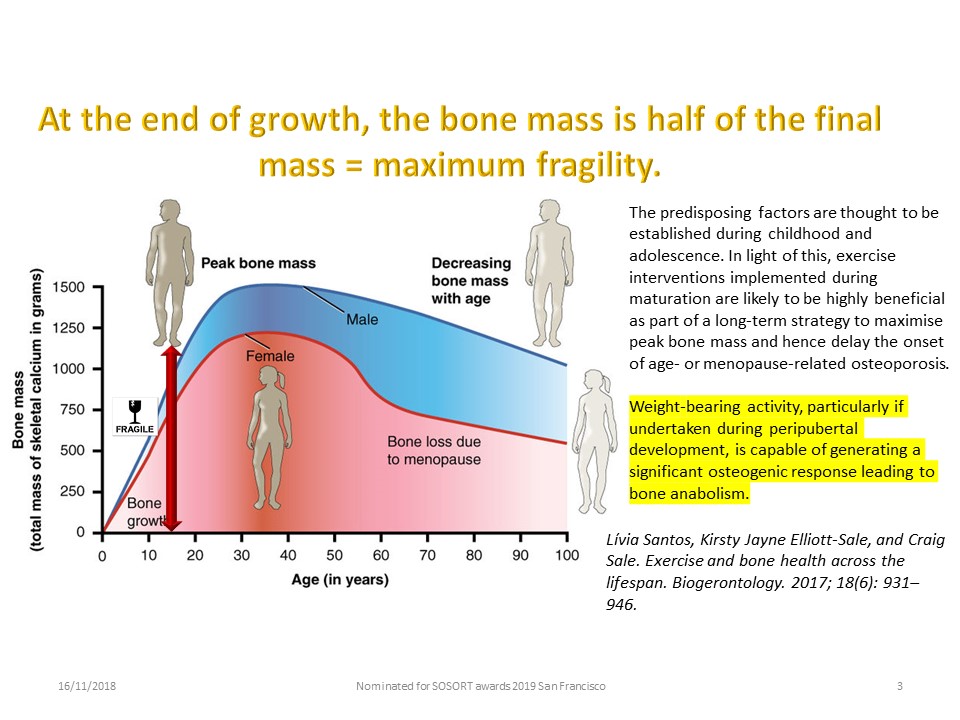 |
Even if weight bearing activity with axial heel impact is part of the Lyon method, the end of height growth is the period of maximal bone fragility of scoliosis. Bone mass will double between 14 and 21 years old in girls, and for the most important scoliotic curvatures, it is necessary to extend the wearing of the brace after 15 years.
|
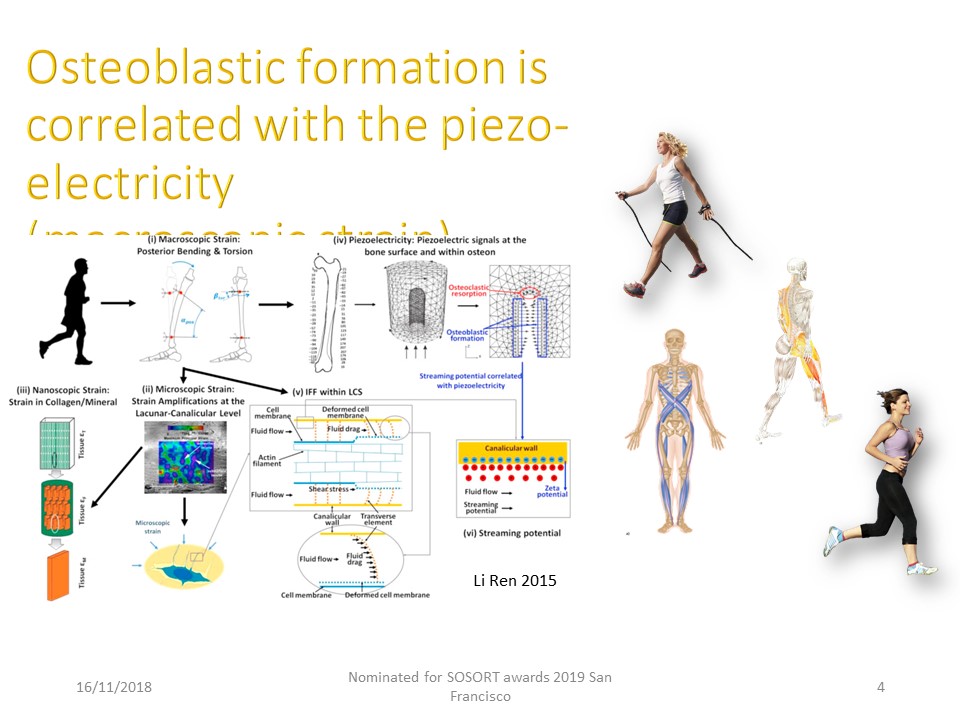 |
Since Li Ren's work in 2015, the mechanisms of calcium fixation on the bone are better known. Indeed the mechanical energy of the heel on the ground is transmitted at the level of the spine and creates a piezo-electric current that promotes the fixation of calcium on the bone.
|
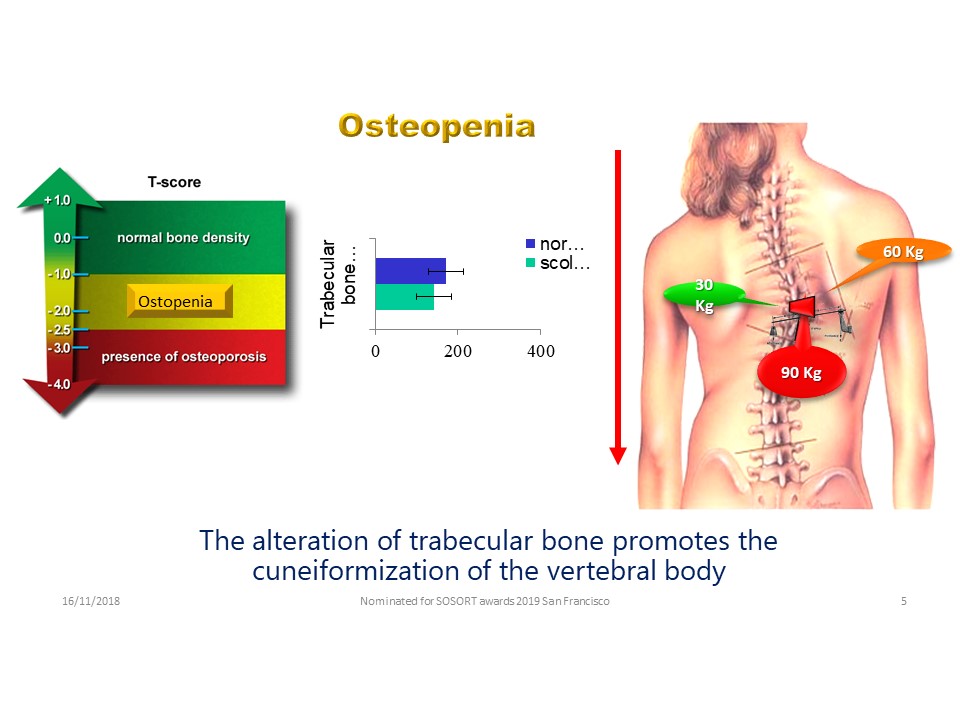 |
Cook's work in 1987 confirmed the existence of an osteoporotic state associated with scoliosis. Evaluation using dual-photo absorptiometry to estimate the trabecular bone mineral density of 44 girls (9-20 years) at lumbar spine and femoral neck confirms that the scoliotic subjects exhibited significantly lower lumbar and femoral neck bone mineral densities than the control subjects. Moreover there is at the apex of the scoliotic curvature areas of hyper and hypo mineralization due to alterations in stresses.
|
 |
The objective is to check if a plaster cast and/or a hyper-corrective brace can be effective at the end of growth. The Lyon brace and especially the Artbrace having a large contact surface with the trunk reduces the load on the spine by the effect of composite beam. The recentering of the disc by night hypercorrection also facilitates load reduction during the day. The readjustment of ligament tensions by plastic deformation characteristic of the initial period of full time is also a positive factor.
|
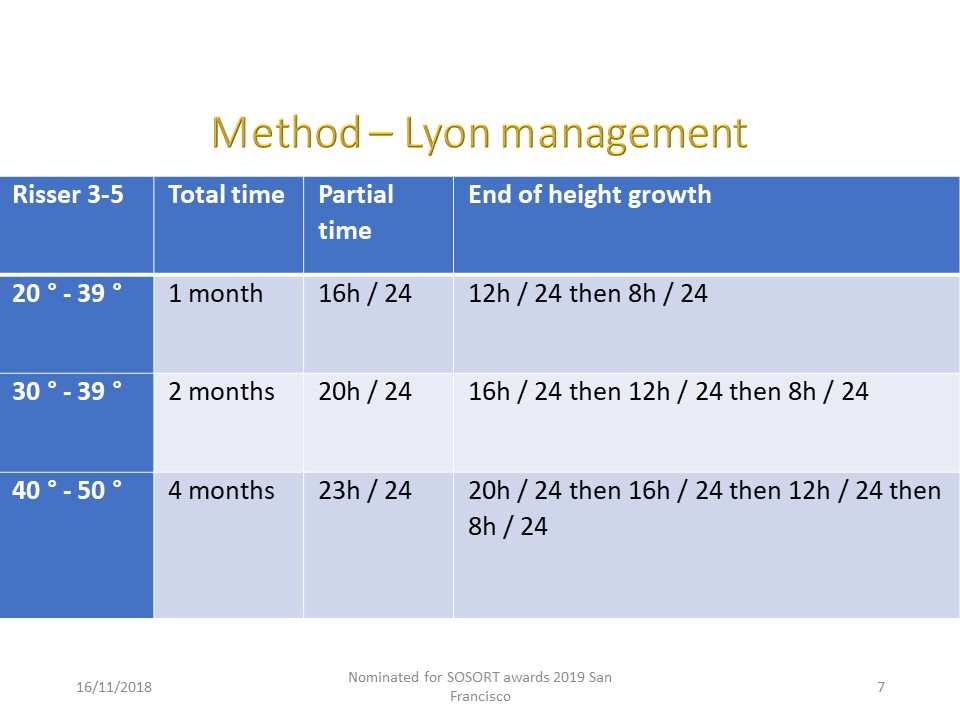 |
At Risser 3-5, the total time is identical, because it is at the soft tissue level that we work. It is no longer a question of guiding growth. The wearing time for the first 6 months is also identical to that of the protocol before Risser 3, however the progression of the ablation time during the day (4 hours every 6 months) no longer depends on the end of growth. The average duration of treatment varied from 18 to 30 months if the initial angulation exceeded 40°. We can therefore specify the duration of the treatment from the day of the consultation. All classical parameters have been studied, but only Cobb (gold standard) angulation will be presented.
|
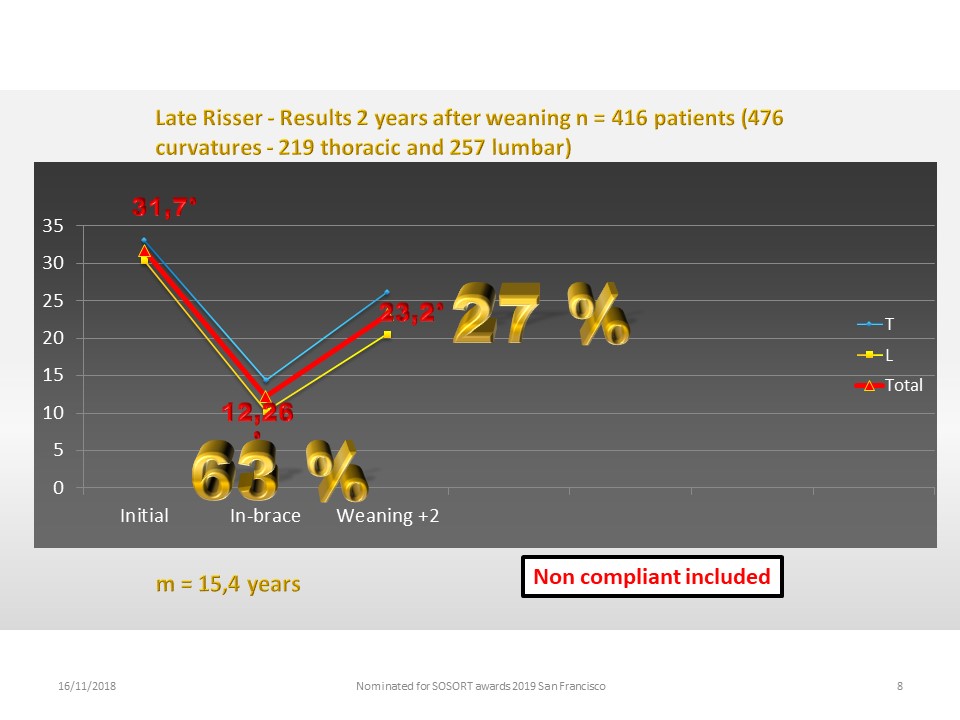 |
Methods: Retrospective study of all 416 consecutive patients reviewed 2 years after brace weaning were retrospectively extracted from our prospective database started in 1998. 476 curvatures: 219 thoracic and 257 thoracolumbar and lumbar were listed. The average age at the start of treatment is 15.4 years. The initial average angulation greater than 30 °. The reduction in plaster cast or ARTbrace is 63%, which allows good plastic deformation of the paravertebral ligament structures. The final correction 2 years after brace weaning is 27% strictly corresponding to plastic deformation.
|
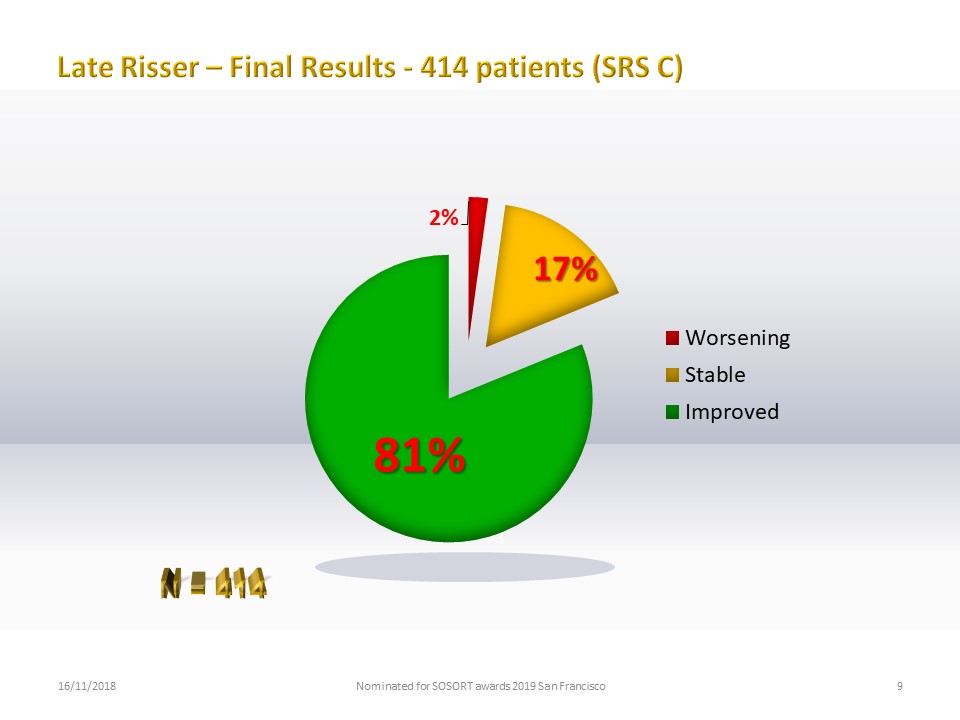 |
While there was still a risk of worsening the curvature at this stage, only 2% worsening is noted, mostly for non-compliant patients. 17% are stable and 81% are improved by more than 5 ° according to the SRS criteria.
|
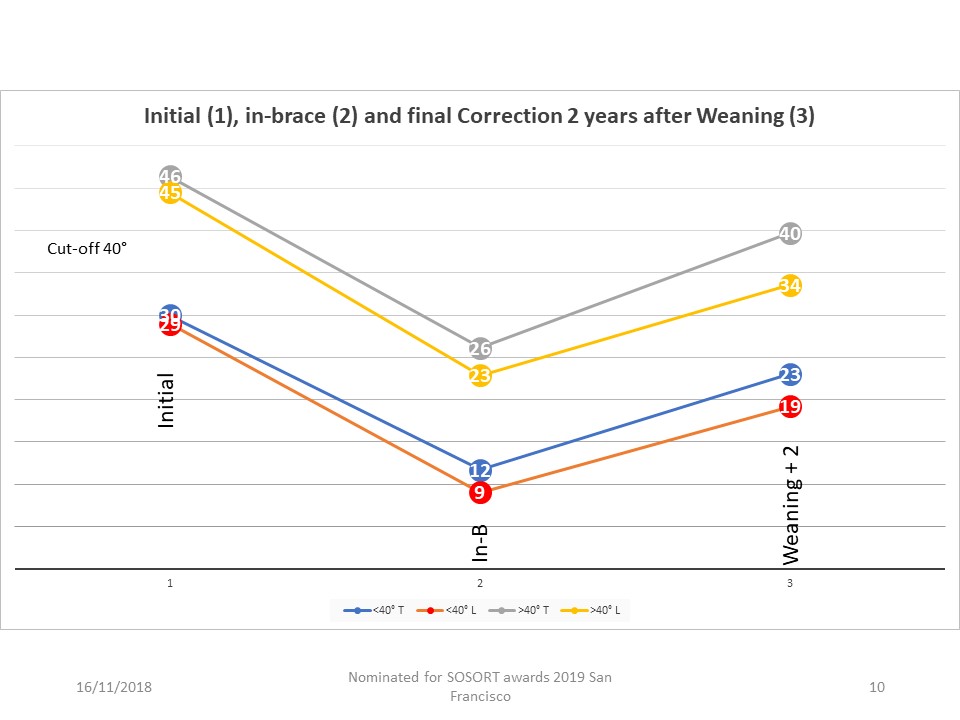 |
The patients were divided into two groups with a 40 ° cut off. All the curves are superimposable. The angulation does not modify the effect of the brace on the level of the soft tissues. There is also no difference between thoracic and lumbar curvatures.
|
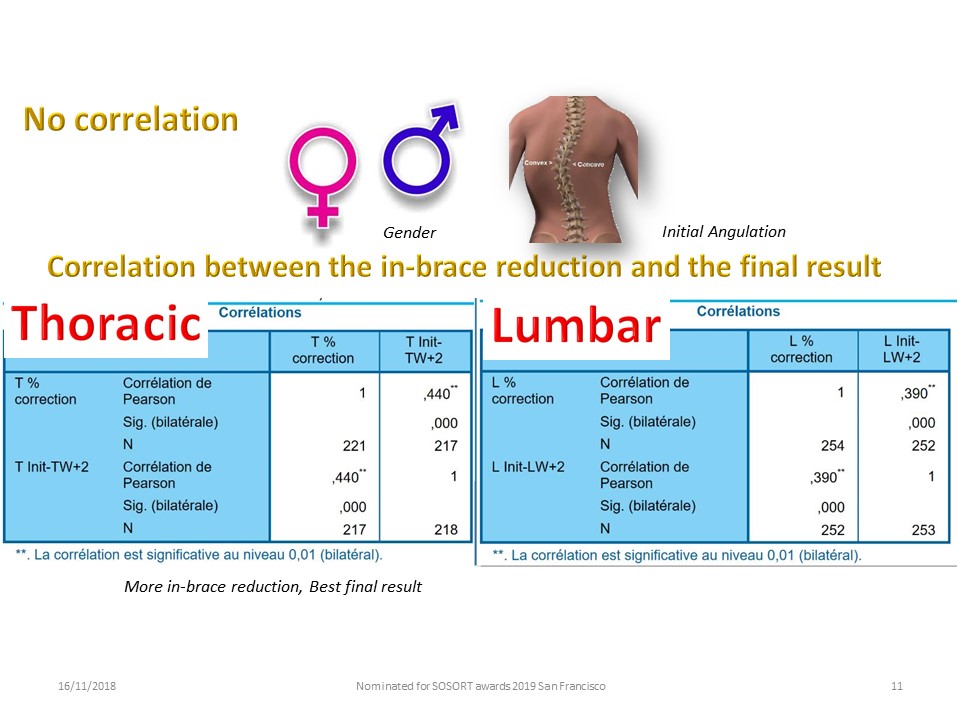 |
There is no correlation based on gender and initial angulation. A Pearson product-moment correlation coefficient was computed to assess the relationship between in-brace correction and Cobb angulation 2 years after weaning There was a good positive correlation between the two variables the initial in-brace correction and the final result 2 years after the brace weaning is found. This correlation allows for borderline surgical cases to ensure the effectiveness of our treatment, which encourages patients. When the in-brace correction is less than 20%, we immediately advise surgery. Between 20 and 50% correction we insist on compliance.
|
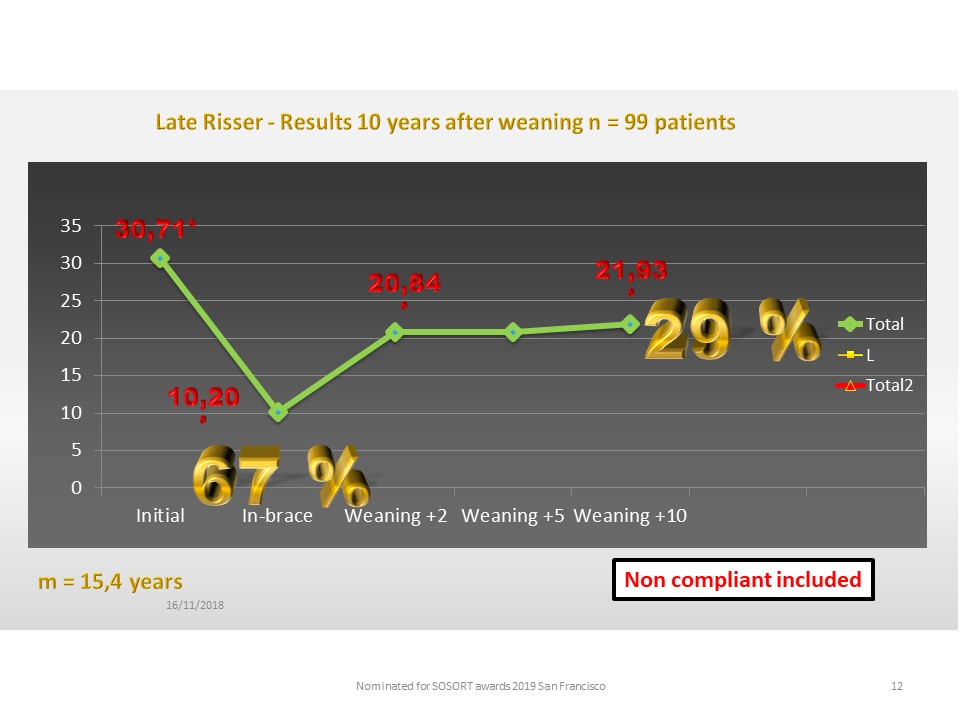 |
A second part of this study concerns long-term stability. 99 patients were seen 10 years after brace weaning. The curve is identical to that of the general statistics and perfect stability for 10 years is observed.
|
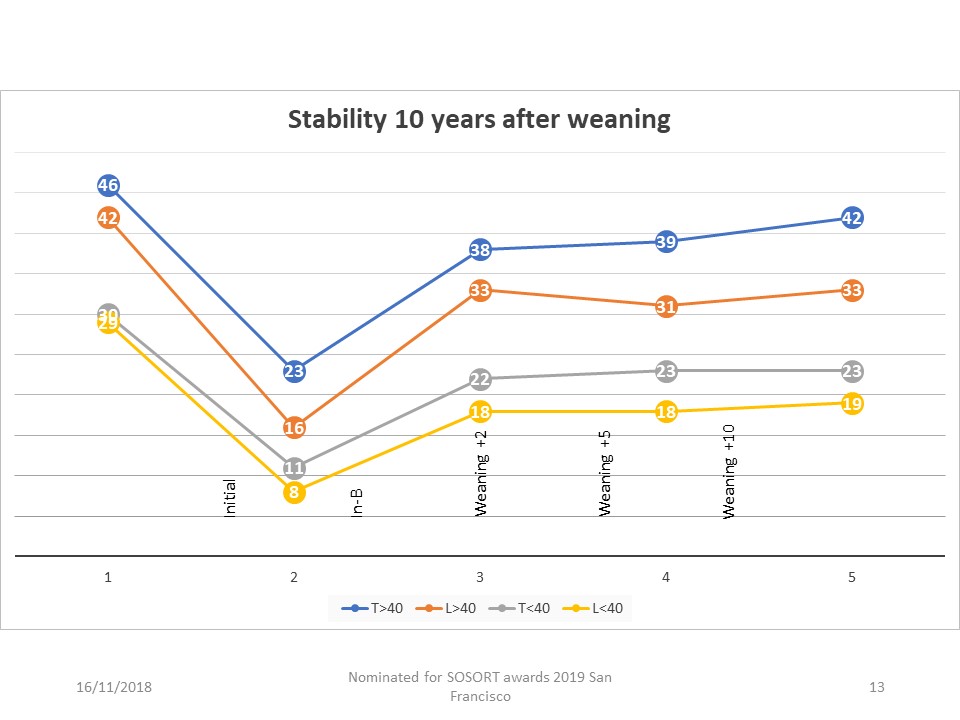 |
With the same 40 ° cut off, the appearance of the stability curve is identical whatever the initial angulation and the type of thoracic, thoraco-lumbar or lumbar curvature.
|
 |
The results of this study confirm us in the interest of these treatments after Risser 3. However, they require an in-brace hyper-correction and the strict initial total time to act effectively on the soft tissues.
|
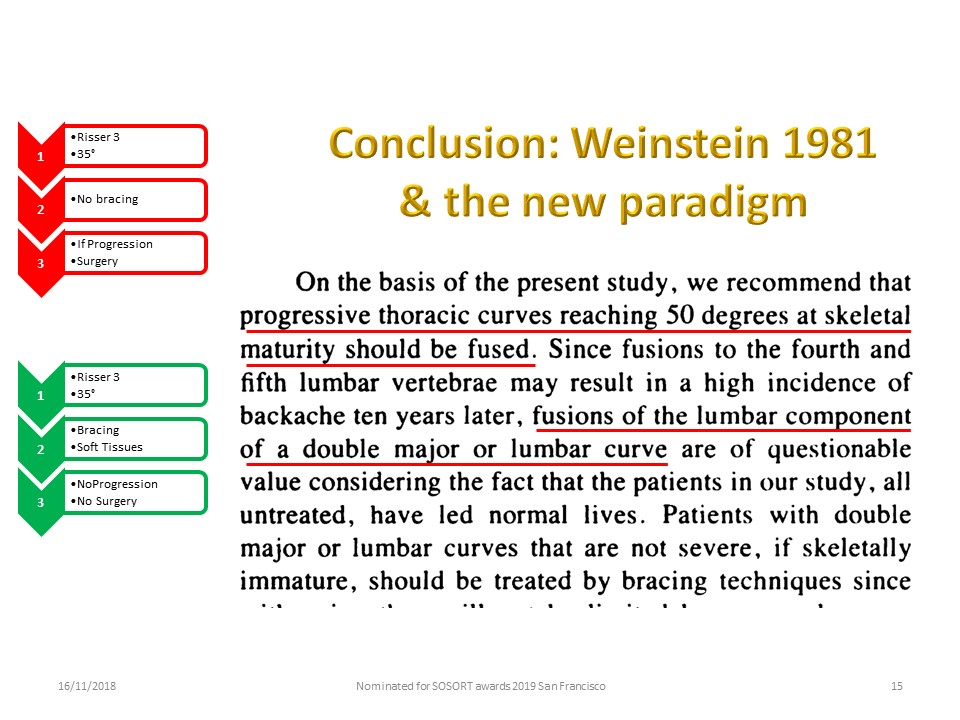 |
40 years later, Stuart Weinstein's conclusions remain valid and systematic surgery for a curvature of more than 40 ° at Risser 3 is an overtreatment. However, not all ortho-prosthetists are currently equipped to manage very high rigidity and the current braces which guide growth are not adapted to plastic deformation. The new paradigm will depend on the evolution of technology.
|
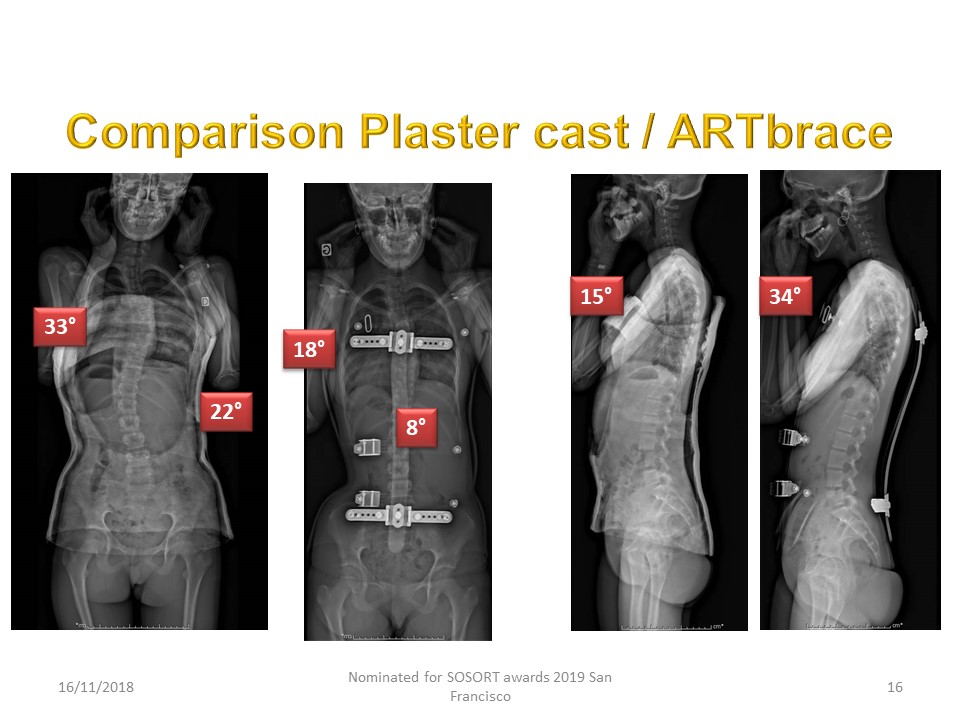 |
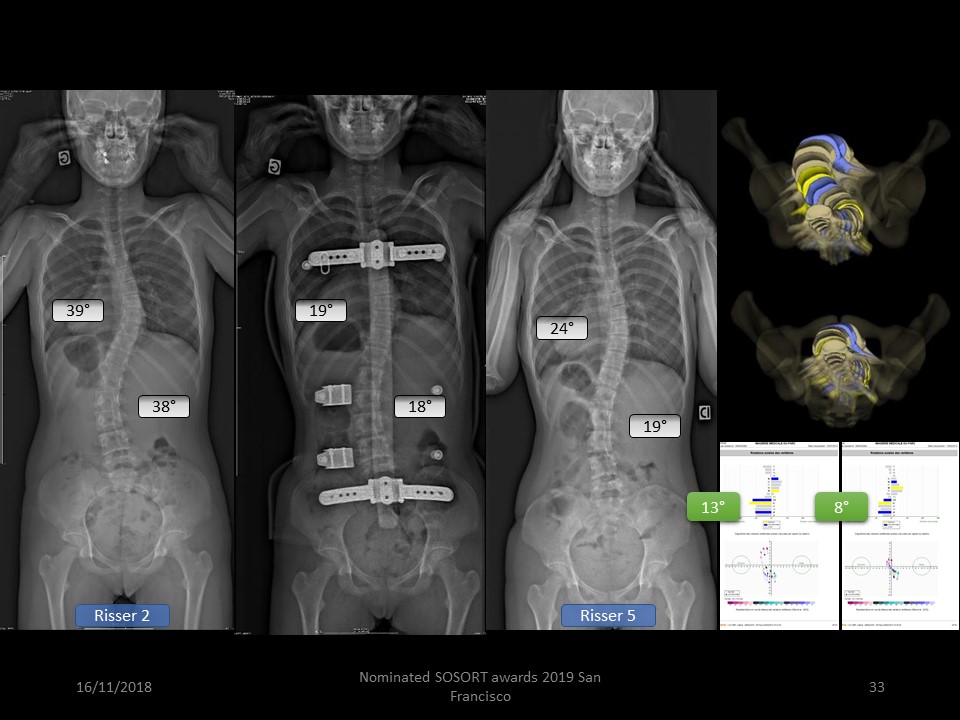
On this example we understand better the interest of new technologies for this type of patient.
|
 |
In conclusion: This statistic is the largest published to date. The night and day hyper-corrective bracing remain effective after Risser 2; the correction being slightly lower than that of younger adolescents, which proves the interest of the creep of the concavity and disc modelling. There is a definitive correlation between the final result and the in-brace correction. Stability in adulthood is identical to that of long-term outcomes with initial plaster cast. The results of the treatments with Risser 3-5 confirm the efficacy of the Plaster cast with plastic deformation on the soft tissues and are an important element of adult stability.
|
 |
Final result of asymmetric polyamide detorsion brace: case series of 110 ADOLESCENT IDIOPATHIC scoliosis according to the SOSORT-SRS recommendations. Background: The initial plaster cast allows plastic deformation or creep of the soft tissues surrounding the vertebral body. Polyamide can replace cast and be used throughout the treatment, especially if it is asymmetrical. The association asymmetry and high rigidity is the most corrective in the frontal plane. It is the coupling of this frontal correction and the restoration of an isostatic sagittal balance thanks to the regional block moulding which performs the Detorsion. The brace is like a bobsleigh track in the opposite direction to the torso column replacing the 3 points system by a global soft contact.
|
 |
Jean Claude de Mauroy and Sophie Pourret are the inventors of the ART brace.
|
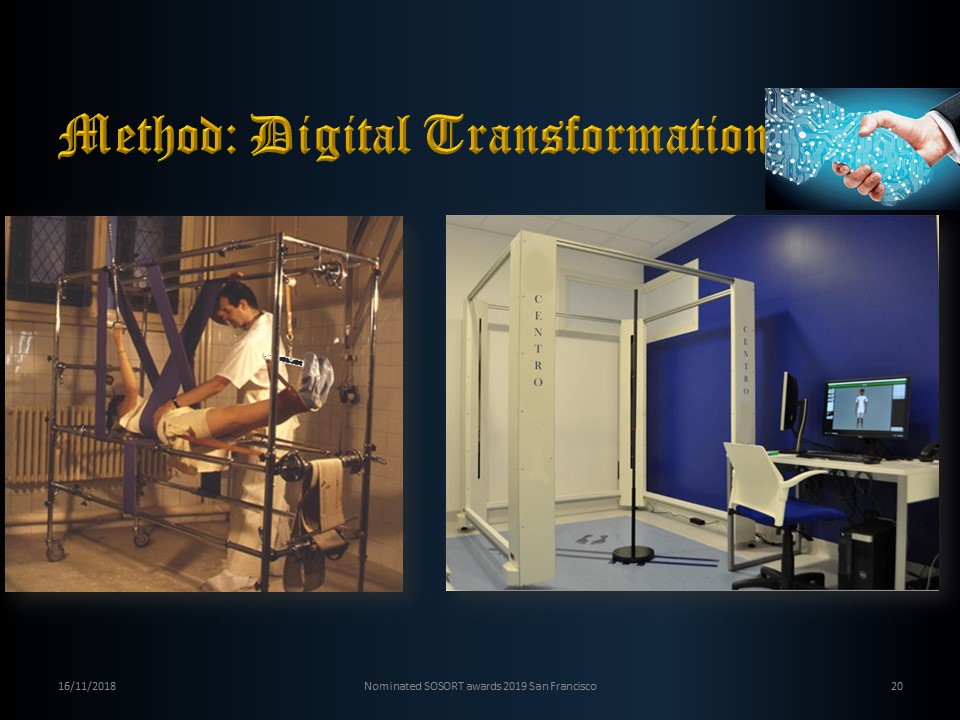 |
The evolution of technology has made it possible to switch from plaster cast correction to digital correction thanks to the use of an almost instantaneous 4-column sensor.
|
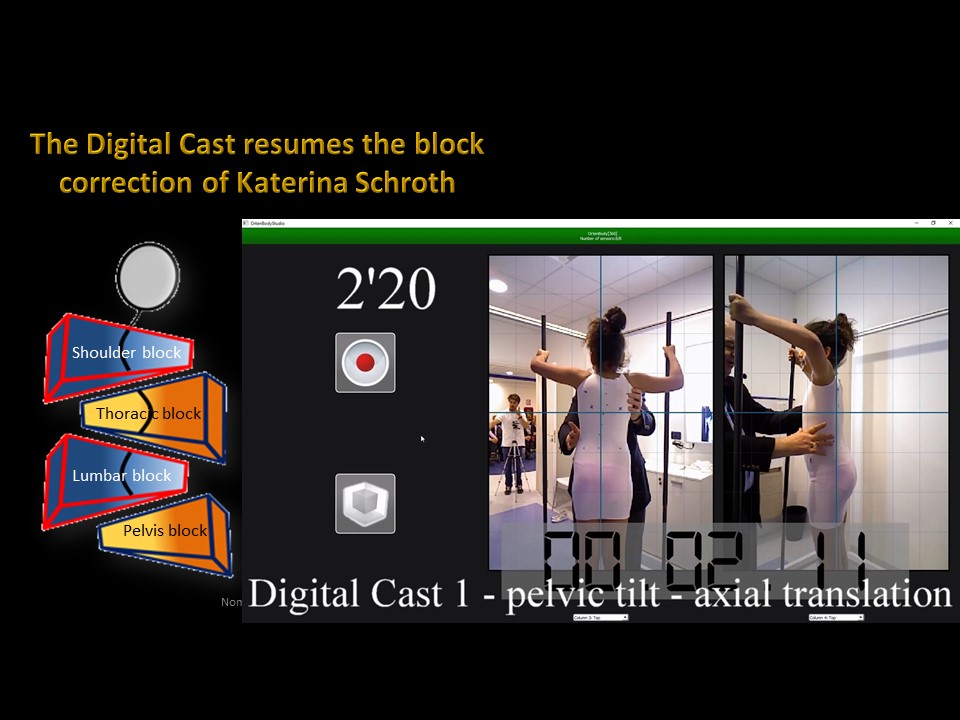 |
This is the same block correction strategy used by physiotherapists in the Schroth method. 3 successive scans record the corrections. 1. Elongation between shoulder girdle and pelvic girdle. 2. Lumbar block in lordosis and shift (translation) in a frontal plane. 3. thoracic block in kyphosis and bending (rotation on the sagittal axis) in the frontal plane. The principle of 3D correction of the Lyon method is based on coupled movements. In the sagittal plane the spine must be in isostatic equilibrium between the posterior arch backward and the intervertebral disc forward. This isostatic balance is determined for each patient according to their lumbopelvic incidence. The coupling of the frontal correction on a spine in sagittal isostatic balance automatically promotes derotation. In fact the rotation is different if the spine is not in an isostatic balance (Harrisson Fryette laws). In the frontal plane, the principle of correction is different at the lumbar level and at the thoracic level for biomechanical reasons of orientation of the posterior joints: sagittal at the lumbar level and frontal at the thoracic level.
|
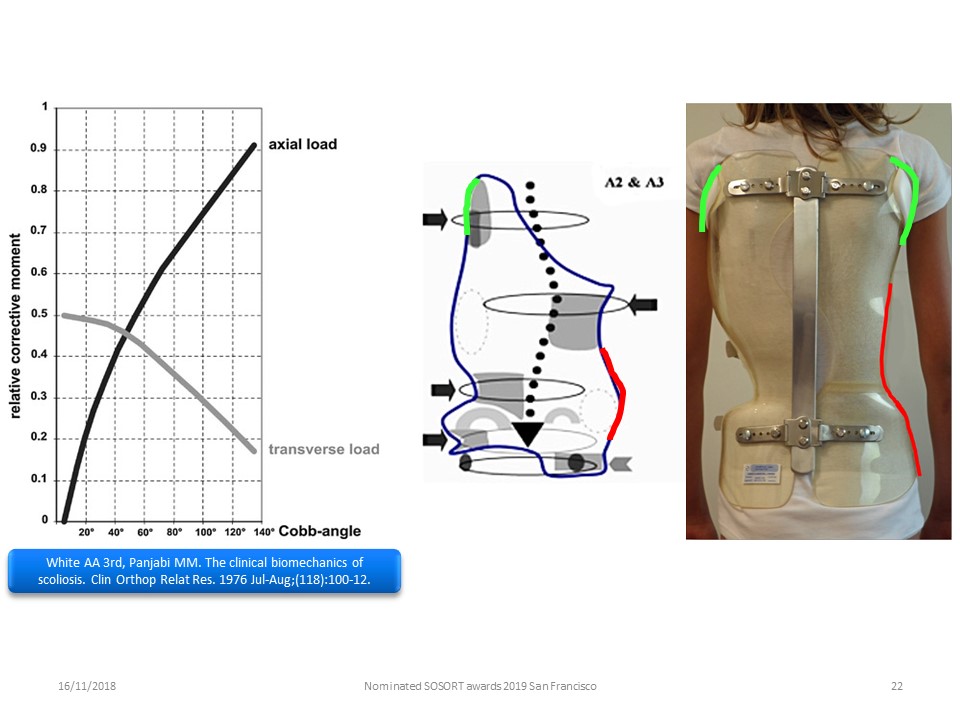 |
The translation along the vertical axis is the principle of Milwaukee brace correction. The action in a horizontal transverse plane is the principle of the majority of braces using a 3-point correction system. The ARTbrace allows to balance the mechanical actions according to the angulation of the scoliosis.
|
 |
As we saw in the Lyon physiotherapy method, radiology confirms that the only way to stretch the ilio-lumbar ligament is to translate this lumbar spine to the concavity. T his is usually enough to straighten the entire lumbar spine. Furthermore, at the lumbar level, the sagittal orientation of the posterior articular joints makes corrective bending impossible.
|
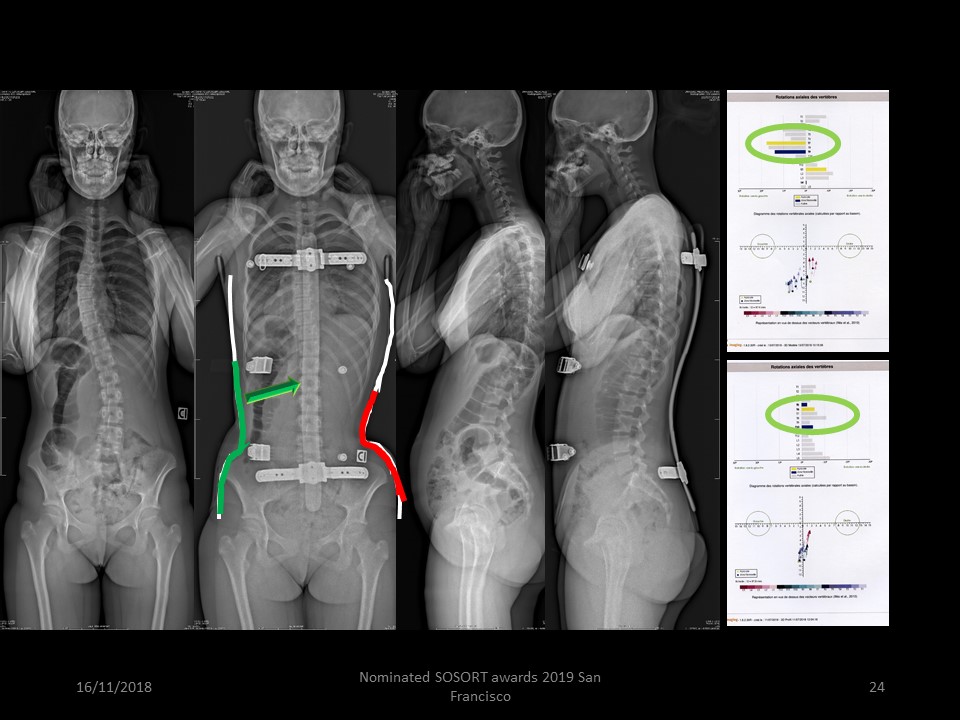 |
Laura is a young patient living in Rio de Janeiro, and is a perfect illustration of automatic detorsion during frontal bending. The thoracic bending is performed from a stable and vertical lumbar spine. In-brace, all the vertebrae align on the line of gravity.
|
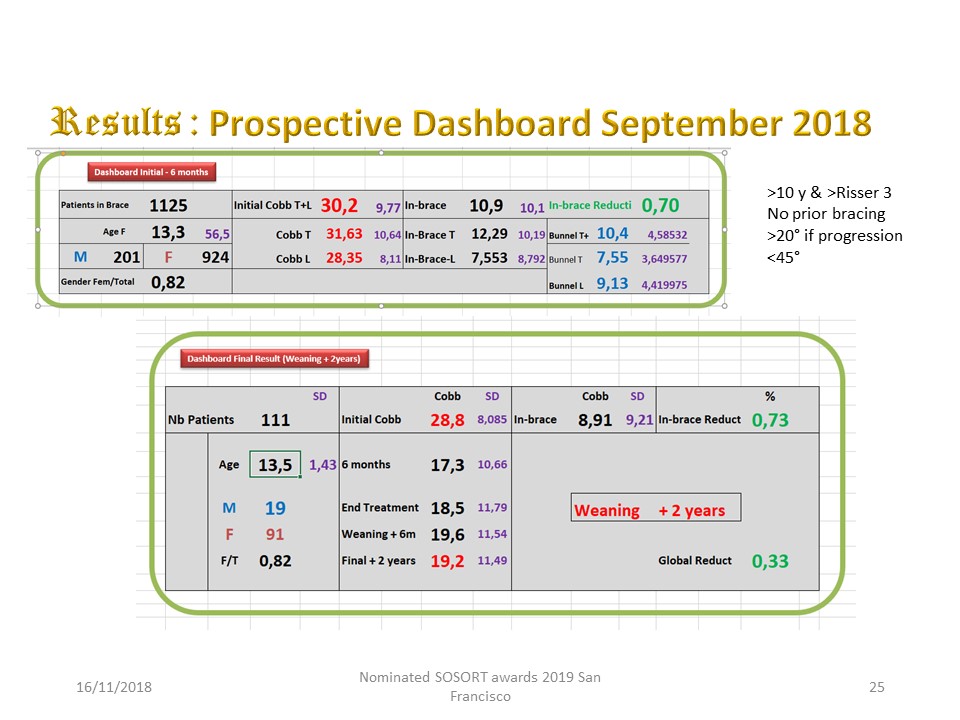 |
Objective: The aim is to present the final result 2 years after weaning and check if there is a correlation between the in-brace correction and the final result. Methods: Since May 2013, 110 Adolescent Idiopathic Scoliosis (91 females/19 males) were reviewed 2 years after brace weaning (from September 2016 to September 2018). The selection criteria are those of Richards: over 10 years and Risser
|
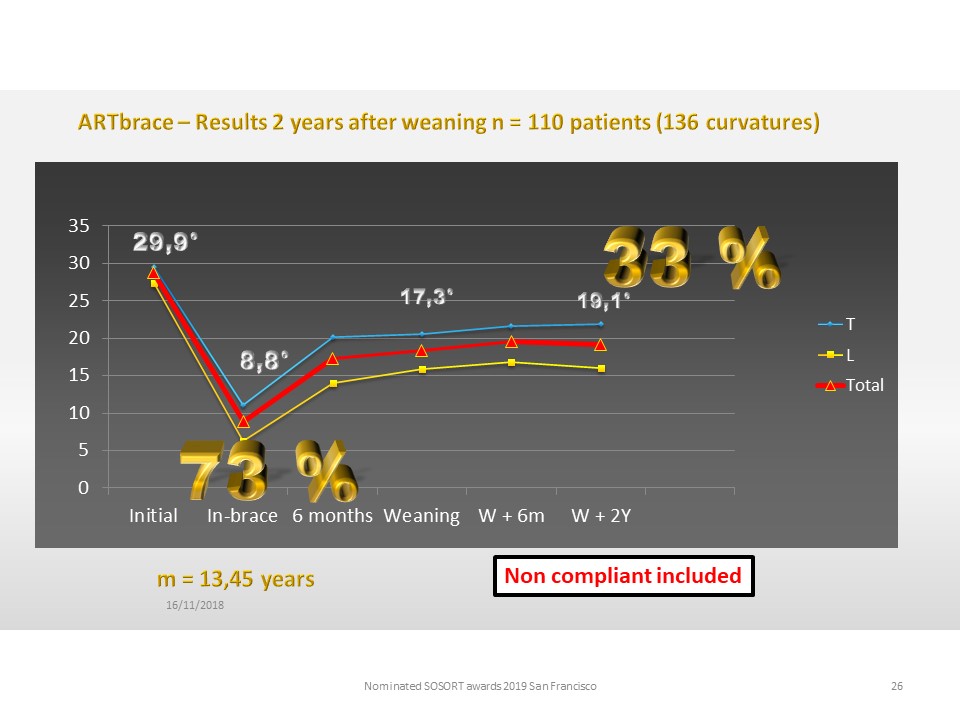 |
Results The 110 patients had an initial mean age of 13.45, The initial mean angulation is: 29.9°, The average in-brace angulation is: 8.83, The average angulation at 6 months without brace is: 17.3, The average angulation two years after weaning is: 19.1°; The average In-brace correction percentage is 73%, the definitive average correction 2 years after brace weaning is 36%.
|
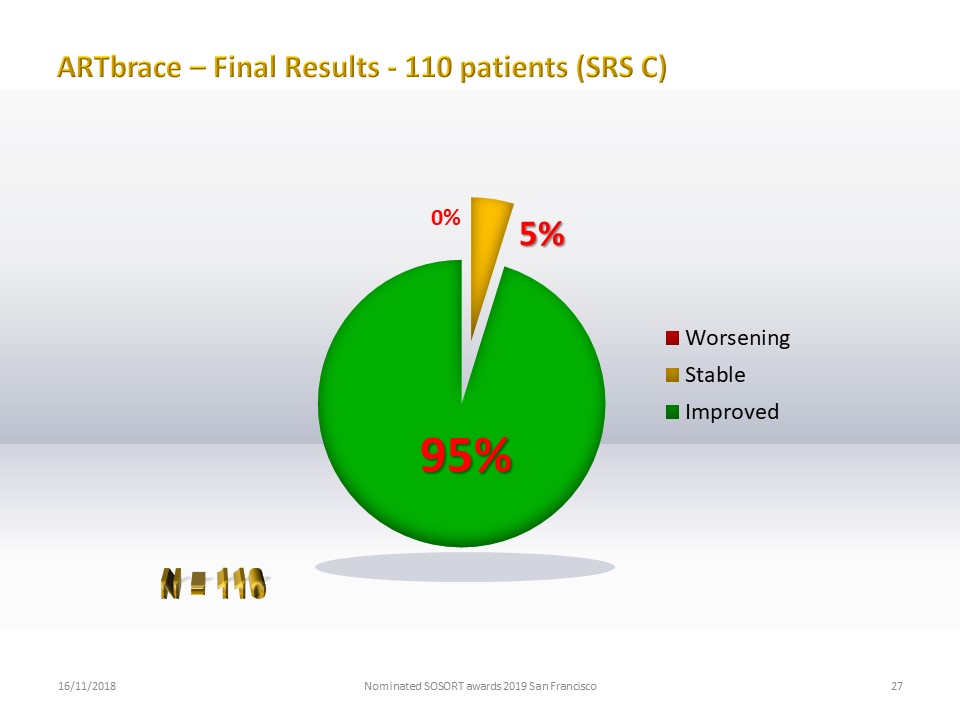 |
95% of the curvatures are improved by more than 5 °, 5% are stable, no curvature is aggravated.
|
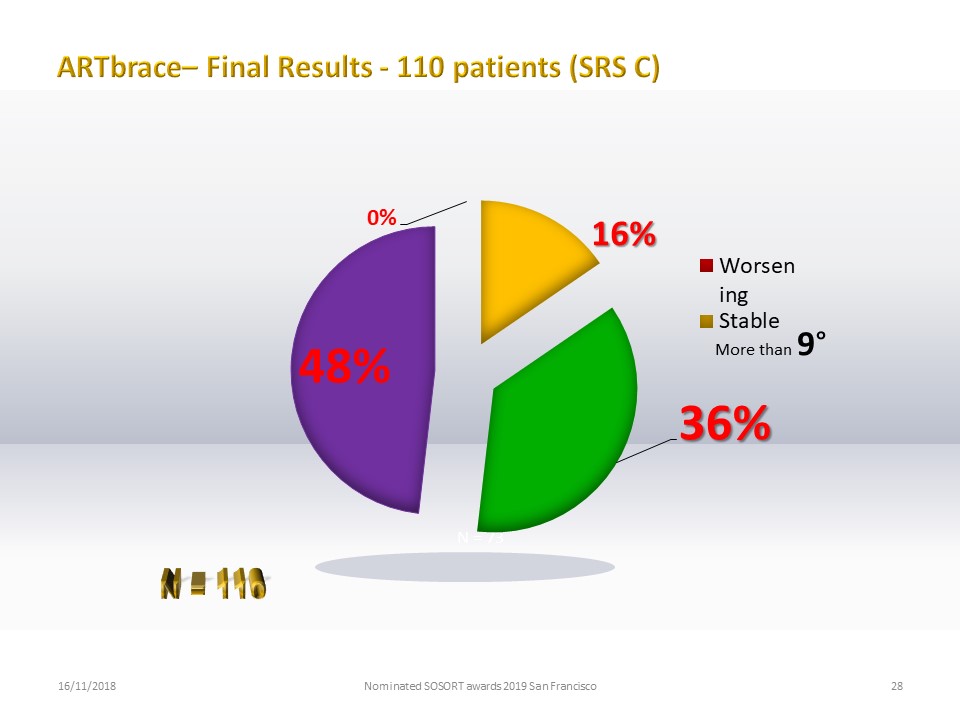 |
Almost 50% of patients have a final result greater than 9 °.
|
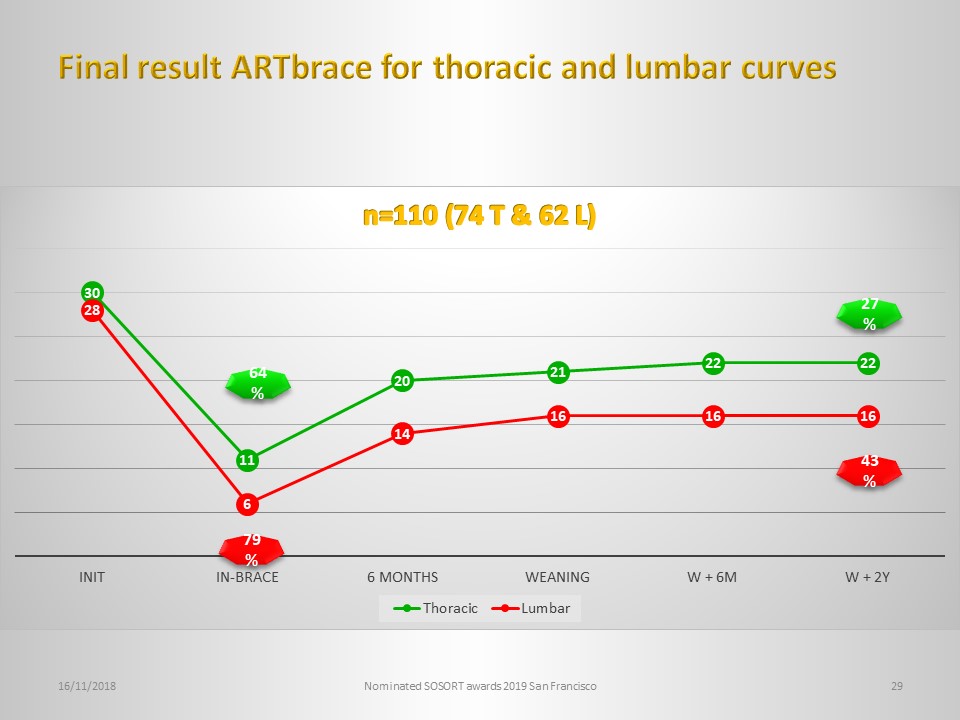 |
The in-brace correction is higher for the lumbar and thoraco-lumbar curvatures, no doubt due to the thickness of the intervertebral discs. On the other hand, the two curves are parallel thereafter.
|
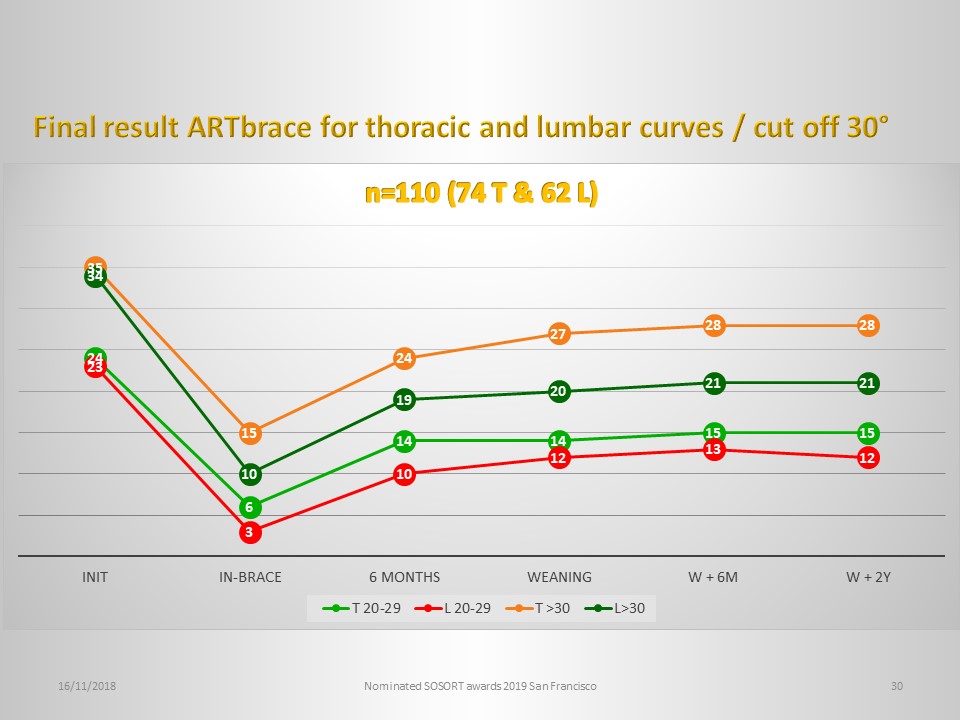 |
The initial angulation within the limits of 20 ° to 45 ° does not seem to modify the results, here with a cut off of 30 °.
|
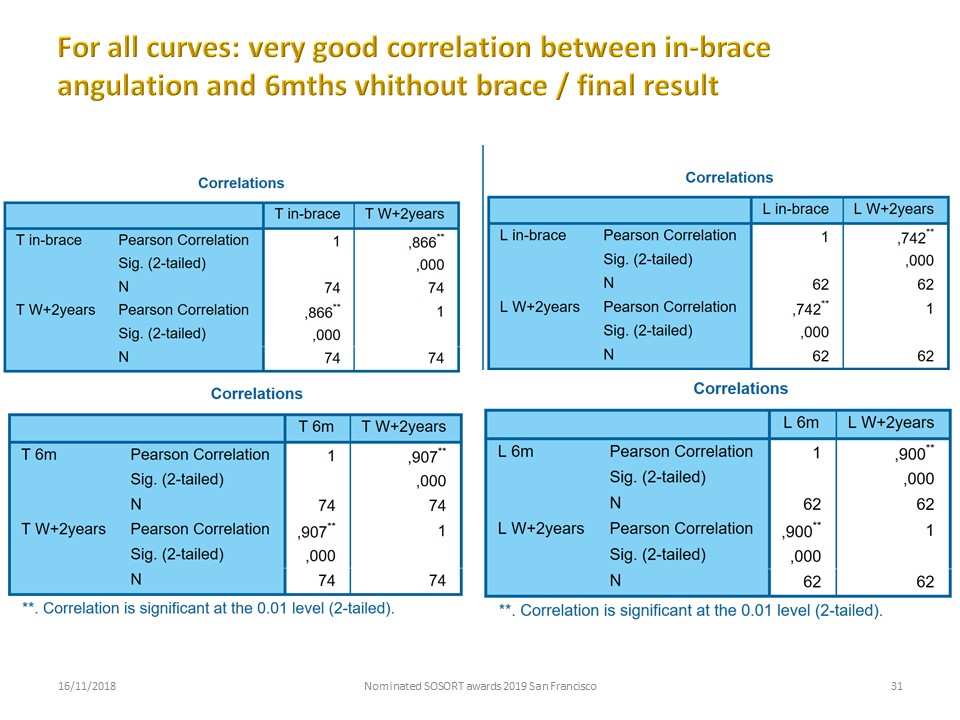 |
A Pearson product-moment correlation coefficient was computed to assess the relationship between Cobb angulation at 6 months and Cobb angulation 2 years after brace weaning There was a good positive correlation between the two variables, r = 90% for thoracic and lumbar curves, There was also a good positive correlation between in-brace correction and Cobb angulation 2 years after brace weaning, r=86% for thoracic curves and r=74% for lumbar curves. These two results allow to establish a prognosis of the final result of the treatment since the in-brace radiography. This prognosis will be refined with the radiograph at 6 months.
|
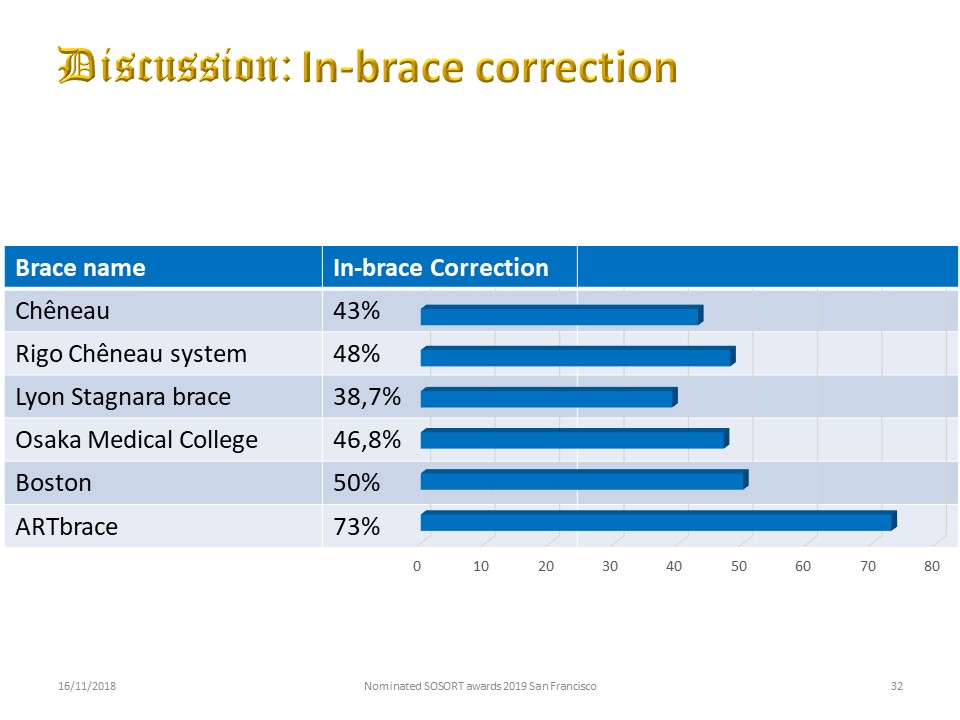 |
Discussion: If we compare the data from the literature under similar study conditions, the in-brace correction is exceptional and superior to all that has been published to date. New technologies therefore make it possible to improve the results of non-surgical conservative orthopedic treatment. Precise protocols also improve the reliability of the results.
|
 |
All the results were analyzed in 3D using EOS, which allowed us to better understand the action of the brace. The protocol has not been changed since 2013.
|
 |
Conclusion and significance: These results confirm previous publications. The average in-brace reduction is the largest published to date. This correction is correlated to the final result. For the first time, it is proven that bracing can not only stabilize, but also correct the initial curvature. The final angulation less than 20 ° is symbolic but allows to hope for an excellent stabilization in the long term.
|
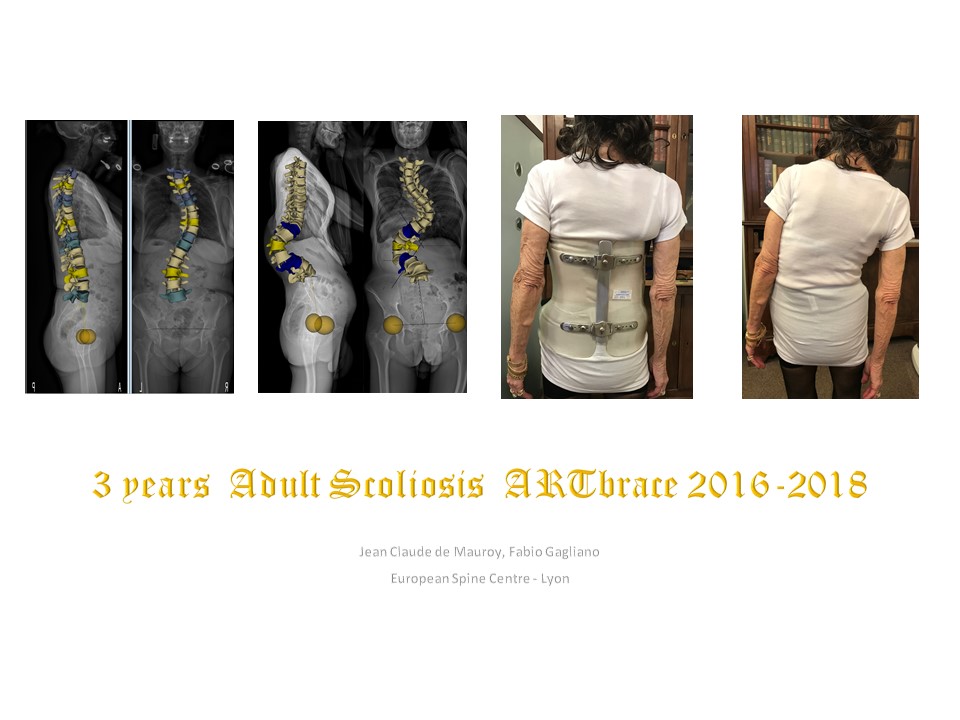 |
Non-surgical conservative orthopaedic treatment in adult scoliosis is often limited to a few specialized centres. However, new technologies make it easier to make corrective braces. At the request of many patients, an adult version of the ARTbrace in 3 mm Europlex was adapted since 2016. The experience of the first 3 years is presented.
|
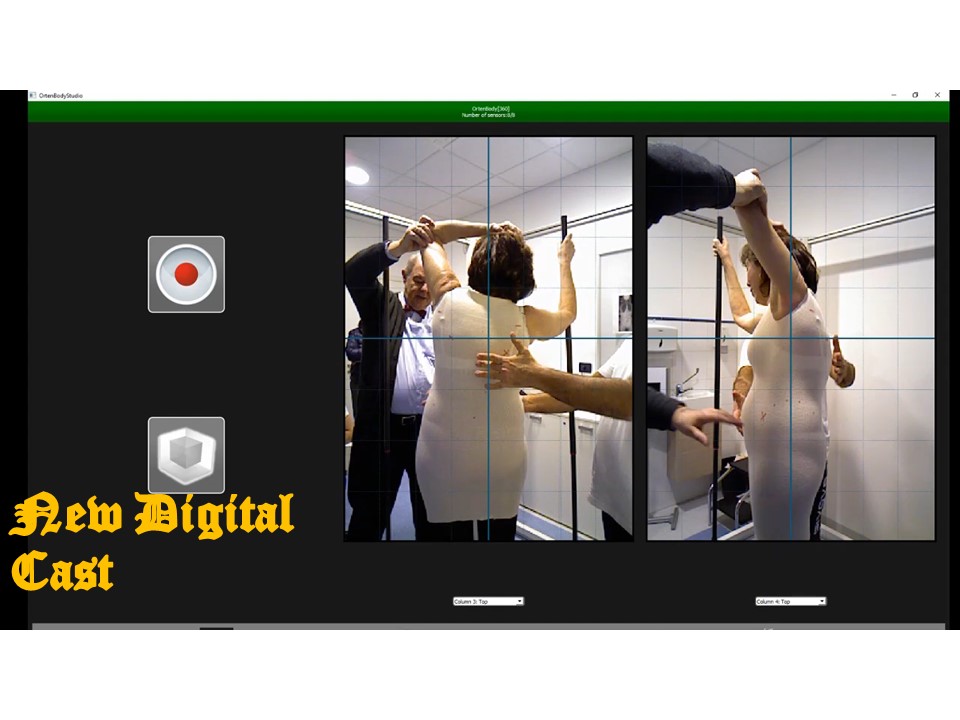 |
New technologies considerably facilitate the production of corrective braces in adults. A preliminary preparation by physiotherapy is however desirable, because the brace will be carried out in the position of maximum correction. The patient is positioned in the centre of the 4 columns. The convex upper limb holds the pole, while the concave hand is placed on the head. The corrective position is derived from the Schroth. The sagittal plane and the frontal plane are corrected simultaneously while ensuring the overall balance of the spine. The spine is placed in maximum extension to promote lumbar lordosis and reduce hyperkyphosis of the chest. Digital cast has replaced the traditional plaster cast. The advantages are multiple: 1. The patient can maintain the maximum corrected position in a standing position for a few seconds. 2. Breathing is controlled, and the patient can be asked for maximum inspiration. 3. The accuracy of the 8 sensor structures is less than 1mm. Very high rigidity 3mm polyamide can be used in place of polyethylene. The processing that is done here in real time is very fast. The green trace corresponds to the infrared which calculates the depth. Image cleaning is performed automatically. It is possible to work with bare skin, but the optical jersey makes it possible to use reference points for the superposition of blocks. Most of the time a single scan is sufficient. The processing allows the realization of the positive which will be milled by a milling machine. The CPO has all the tools to rework the captured shapes if necessary. As soon as the brace is put in place, the wearing protocol is permanent 24:24 for 3 weeks, like the old plaster cast. In addition to the plastic deformation of the paravertebral ligament structures, permanent wearing creates skin anesthesia facilitating adaptation. This is the principle of the watch.
|
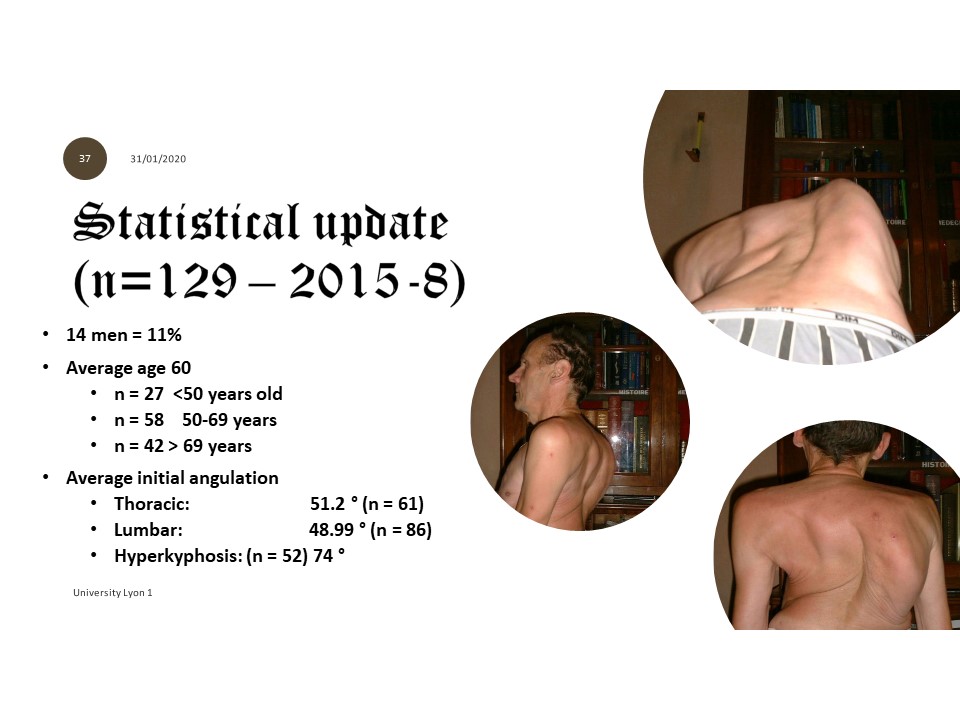 |
129 consecutive patients were seen again 6 months after the placement of the brace, 11% of whom were men. The average age is 60 years. The initial angulations are approximately 50 °. All patients had a painful instability most often associated with a new progressive of scoliosis. Contrary to adolescence, in half of the cases we find a hyperkyphosis of the chest and in some cases a flexum of the hip.
|
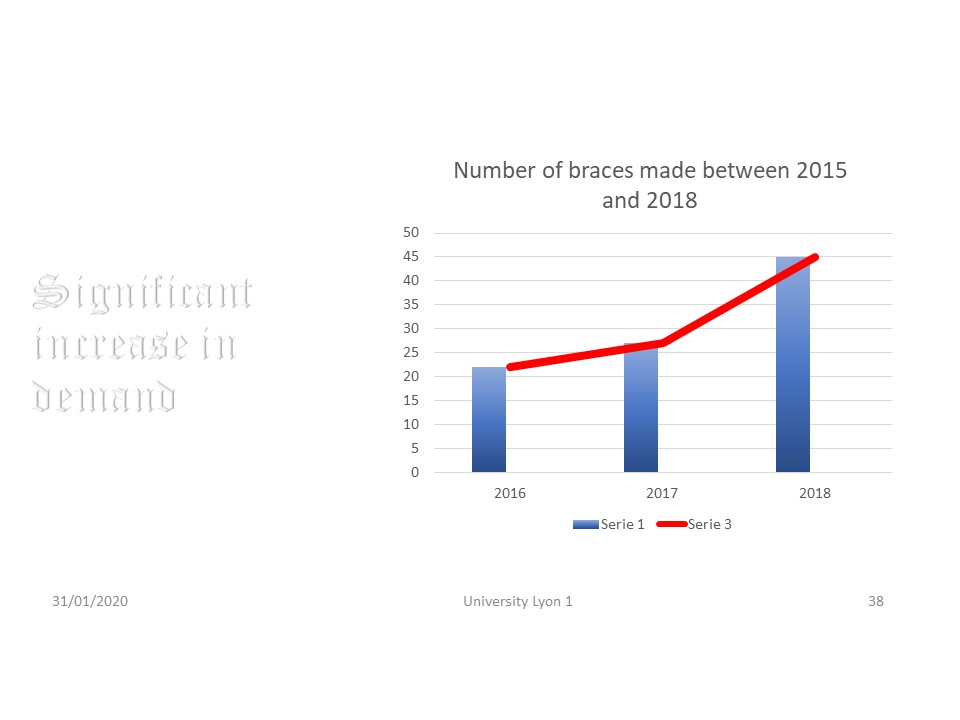 |
Very quickly an increase in demand for this type of treatment is noted, although the inclusion criteria have become more stringent with reducibility in decubitus.
|
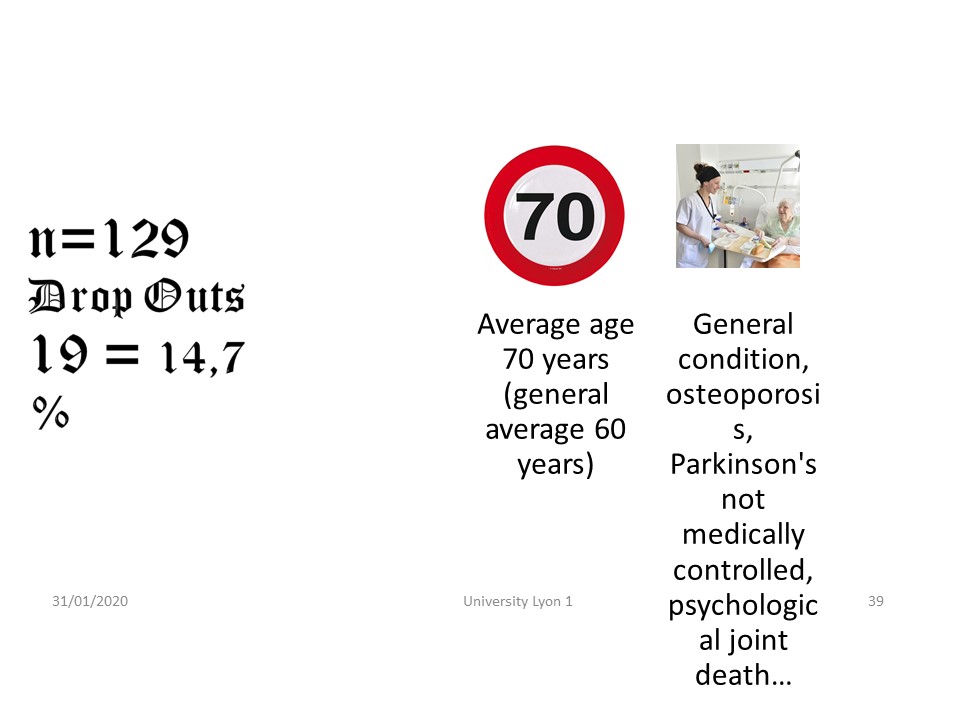 |
The dropout rate is 14.7%, unchanged since the start of this treatment and very low given the negative image of the brace in adults. Patients who have given up are a little older and weakened by pathologies associated with scoliosis.
|
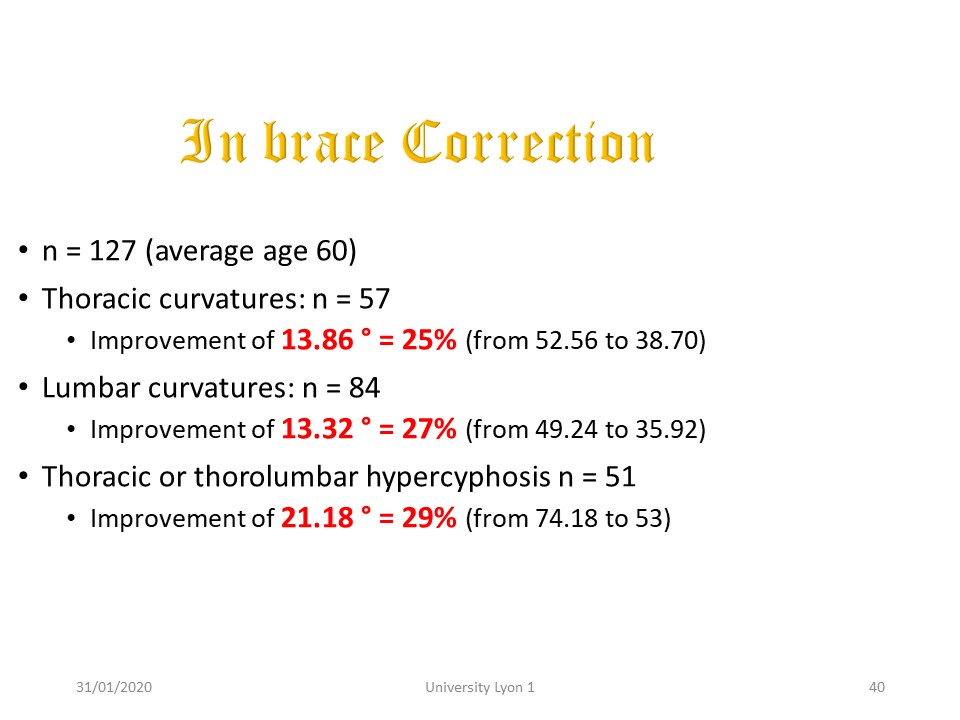 |
The orthopaedic results of in-brace correction are significant with approximately 25% of correction on thoracic and lumbar curvatures, but especially 30% of correction on kyphosis from 74 ° to 53 °, while the average is 45 ° in the normal population. This result is all the more interesting as the defect of the old polyethylene brace was the insufficient correction in the sagittal plane.
|
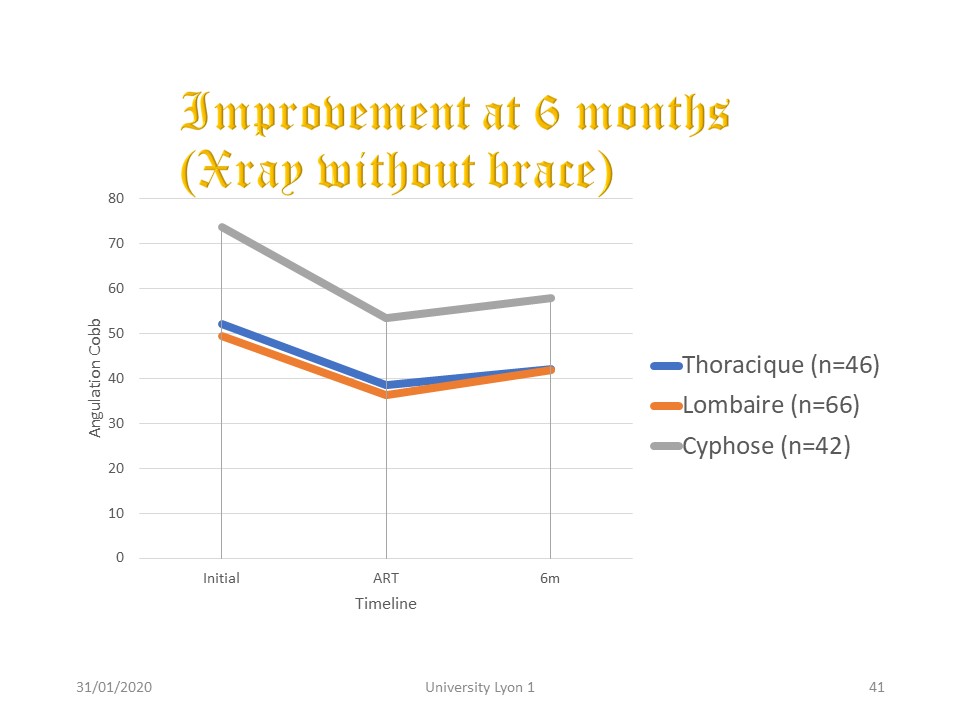 |
This correction is partially maintained at 6 months depending on the elasticity of the paravertebral ligament structures.
|
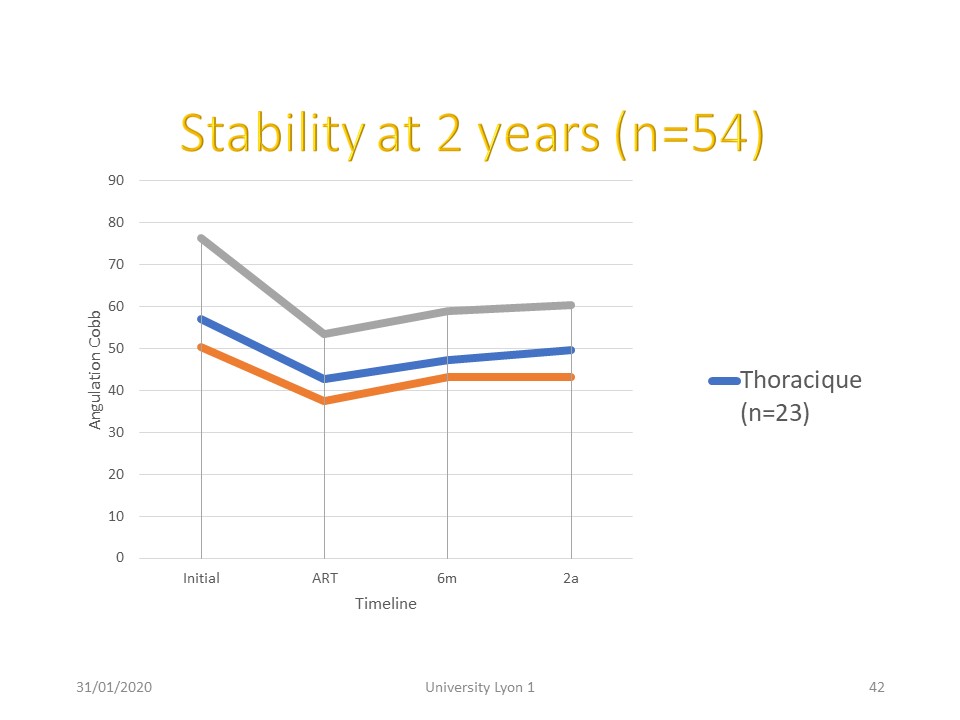 |
The stability is almost perfect between 6 months and 2 years after the fitting of the ART brace.
|
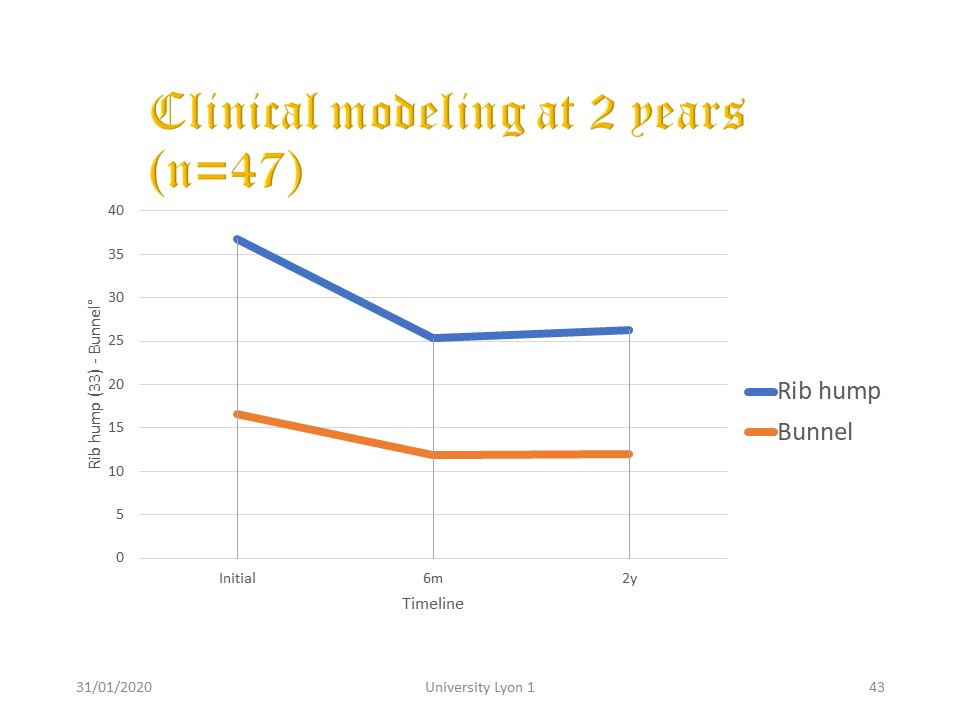 |
It is the same for the rib hump and the ATR. This modeling effect is highly sought after by patients.
|
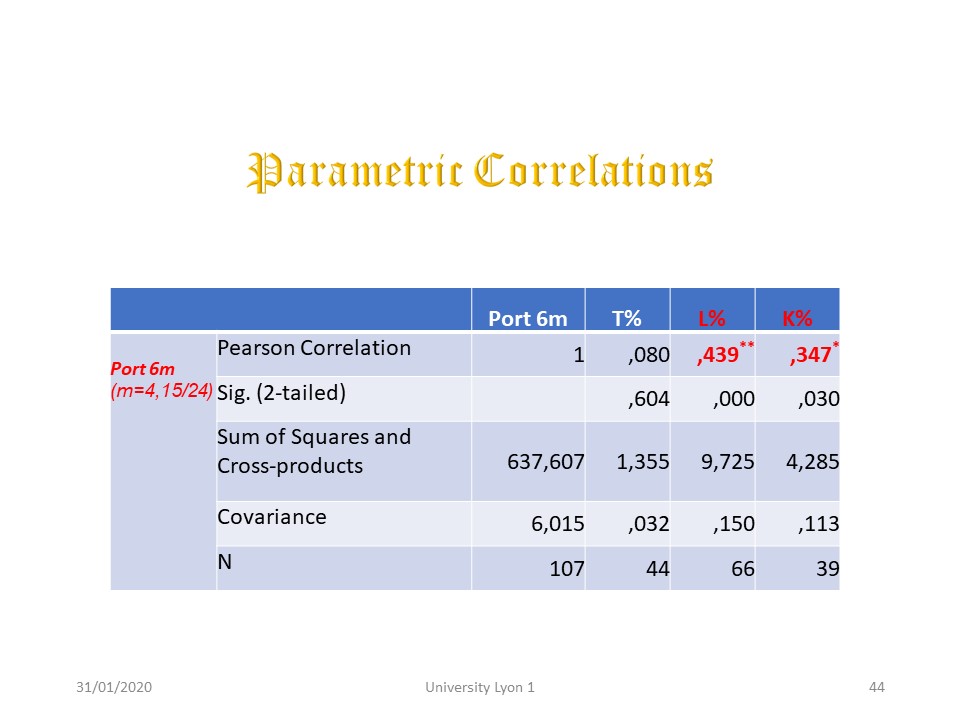 |
The usual indication of wearing the brace is 4 hours during the day after 3 weeks of total time. At 6 months we noted the actual wearing time of the corset and looked for correlations with the percentage of correction at 6 months. There is a significant correlation for lumbar correction and kyphosis. At the thoracic level, the percentage of correction seems more to be linked to plastic deformation during the initial full time of 3 weeks.
|
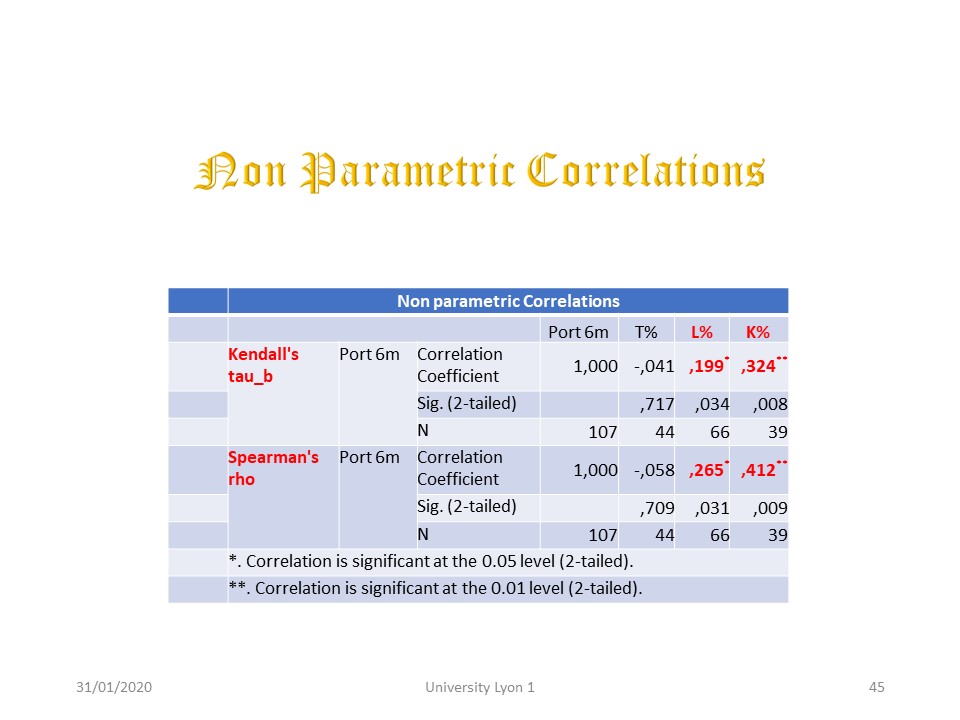 |
The non-parametric correlations confirm the prolongation of the mechanical action at the lumbar level and in the sagittal plane.
|
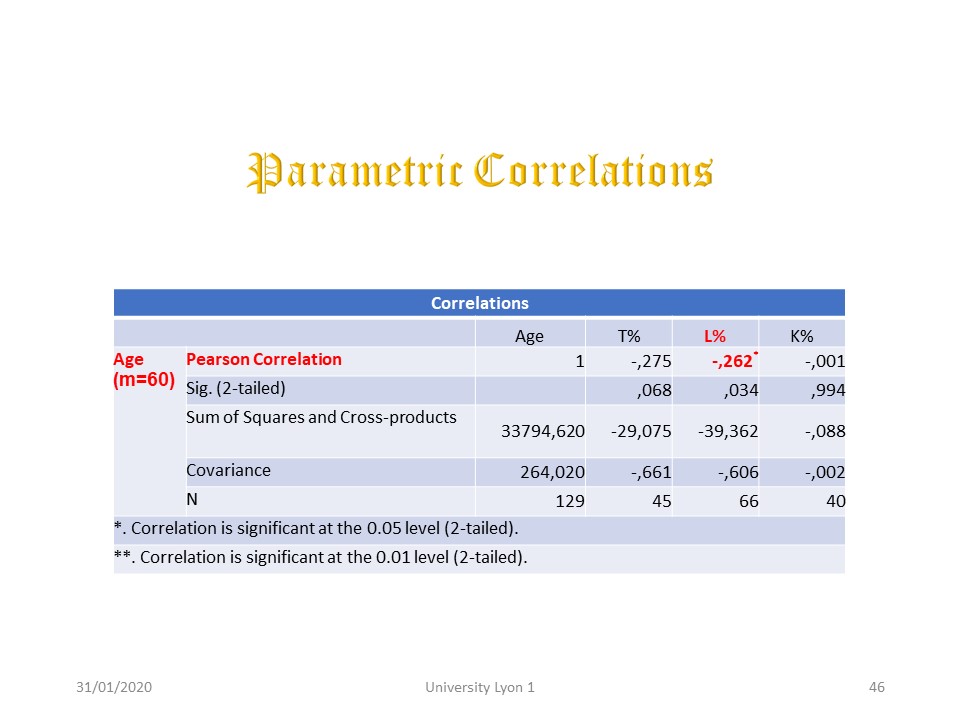 |
Age could also be a correction factor. It does very little with a little more lumbar stiffness in older patients.
|
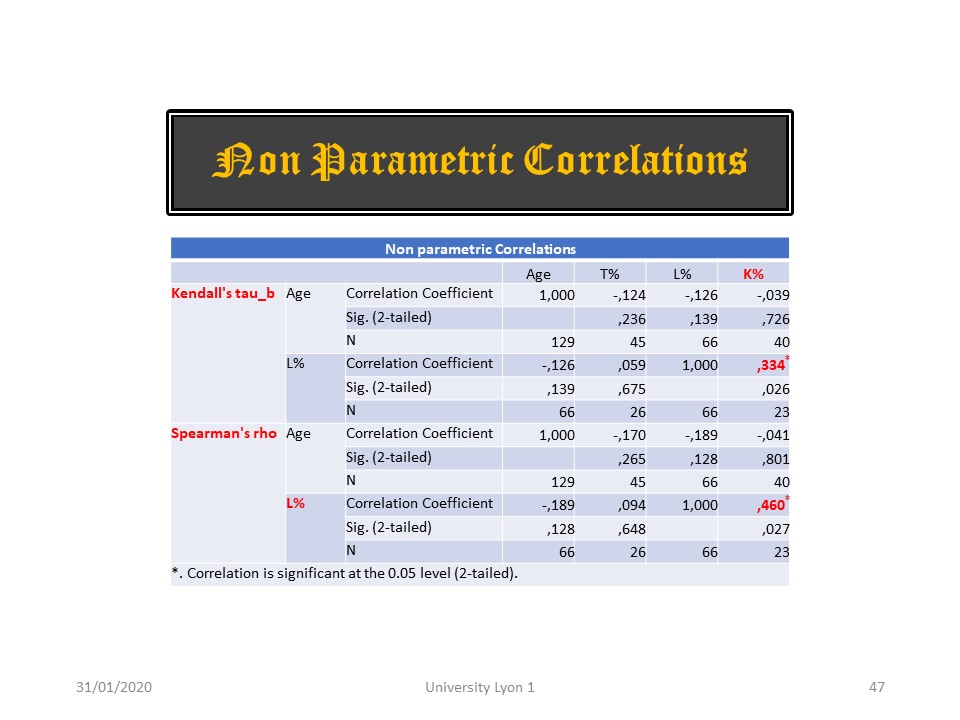 |
Nonparametric correlations confirm that lumbar stiffness increases with age.
|
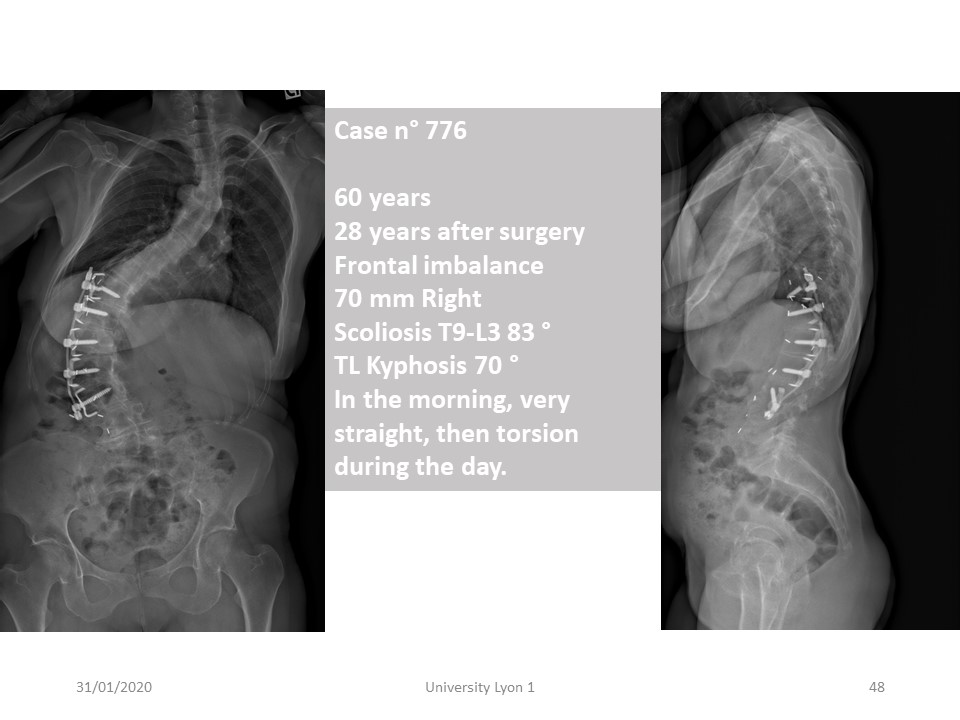 |
The Case n° 776 is an example of the new management This patient was seen at 60 years, 28 years after surgery with a good anterior Lumbar arthrodesis, but upper thoracic decompensation The Frontal imbalance is 70 mm Right, Cobb angulation T9-L3 83° and Thoraco-lumbar kyphosis 70° In the morning, she is very straight, then torsion appear during the day. x
|
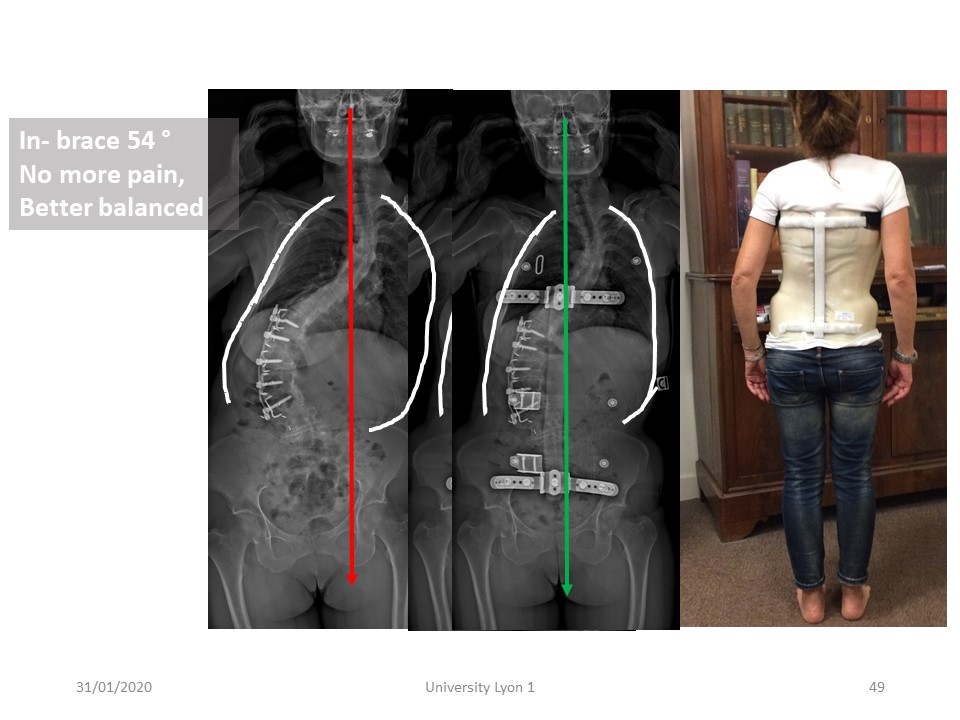 |
She did not want the recommended surgical revision and prefer to try bracing, In-brace Cobb angle was 54°, No more pain since the first night, and better balance.
|
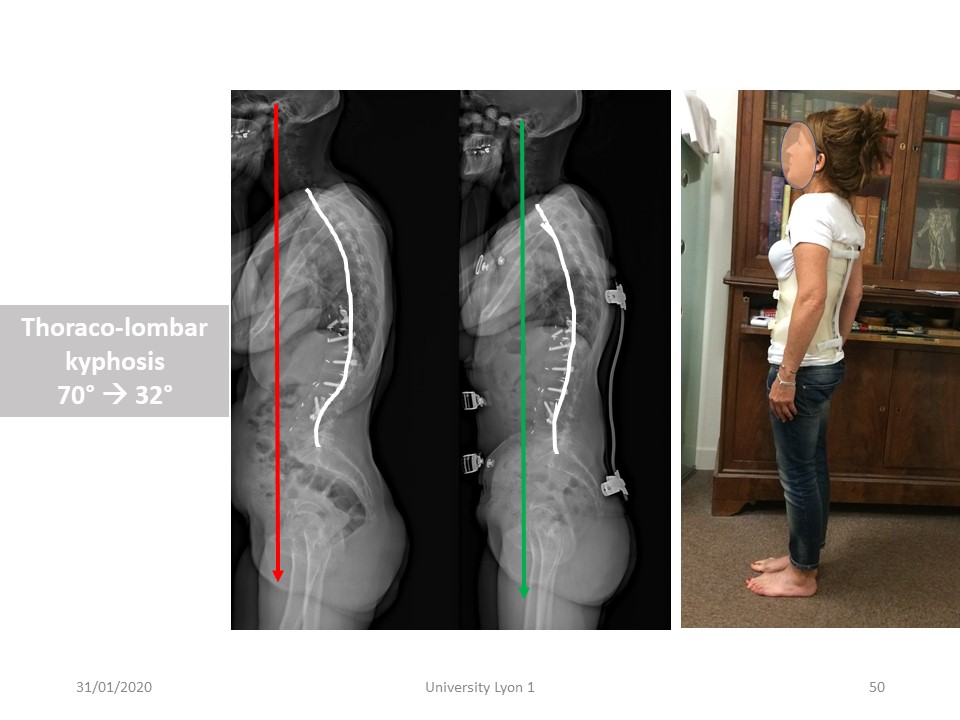 |
But the most spectacular result is in the sagittal plane with marked improvement in thoraco-lumbar kyphosis. Given the arthrodesis, this improvement is difficult to explain.
|
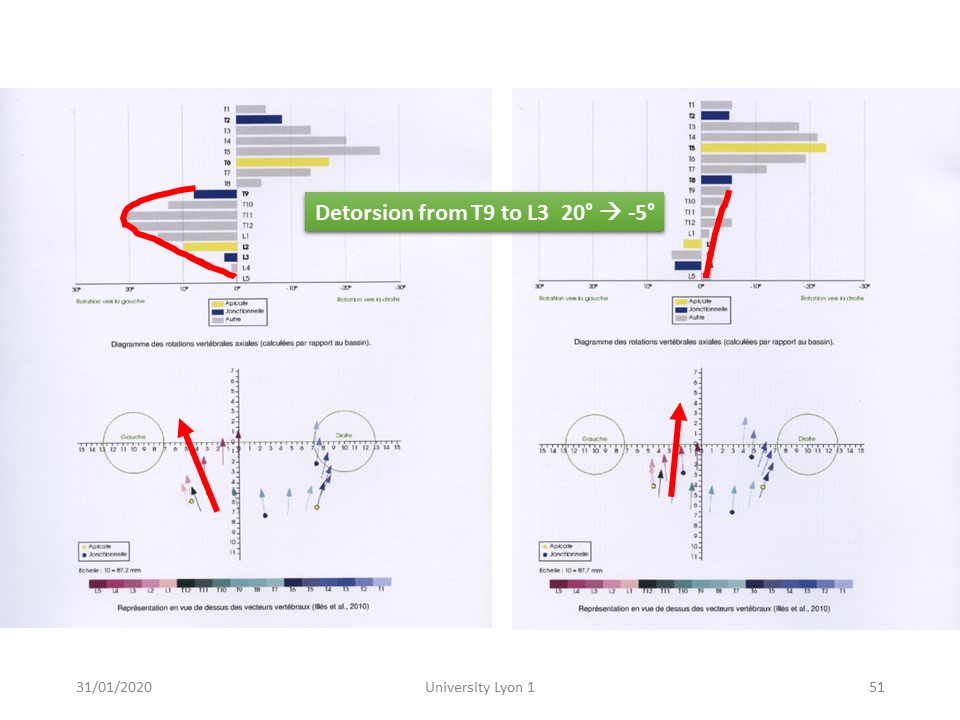 |
It is the EOS 3D study that shows the nearly 25° detorsion mechanism from T9 to L3, confirming that the ARTbrace is a detorsion brace, even in adults.
|
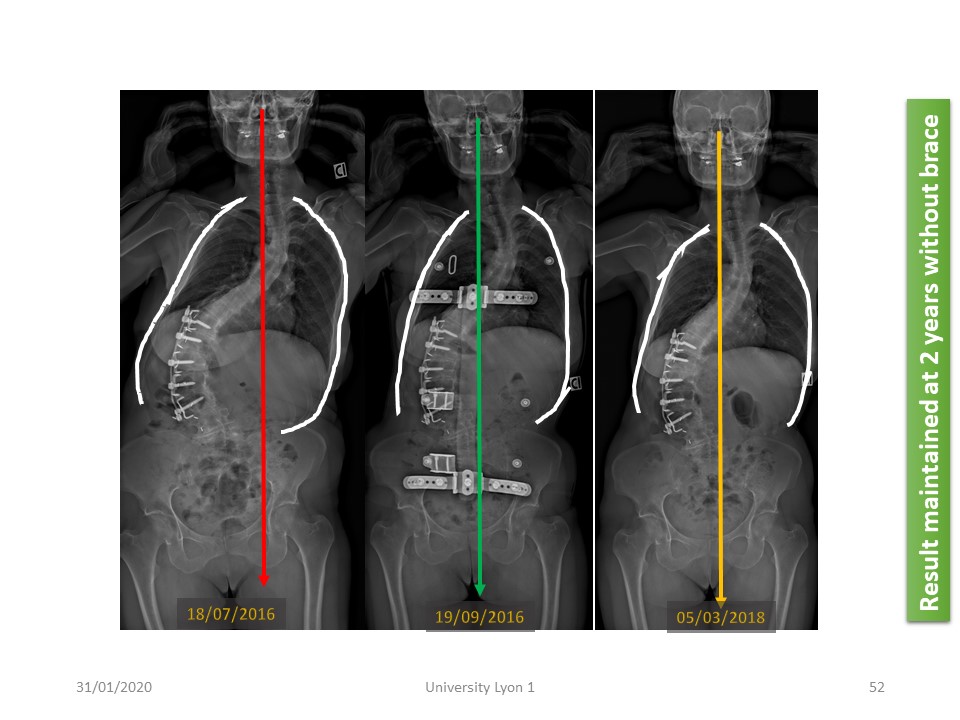 |
This improvement seems to be maintained over time here in the frontal plane...
|
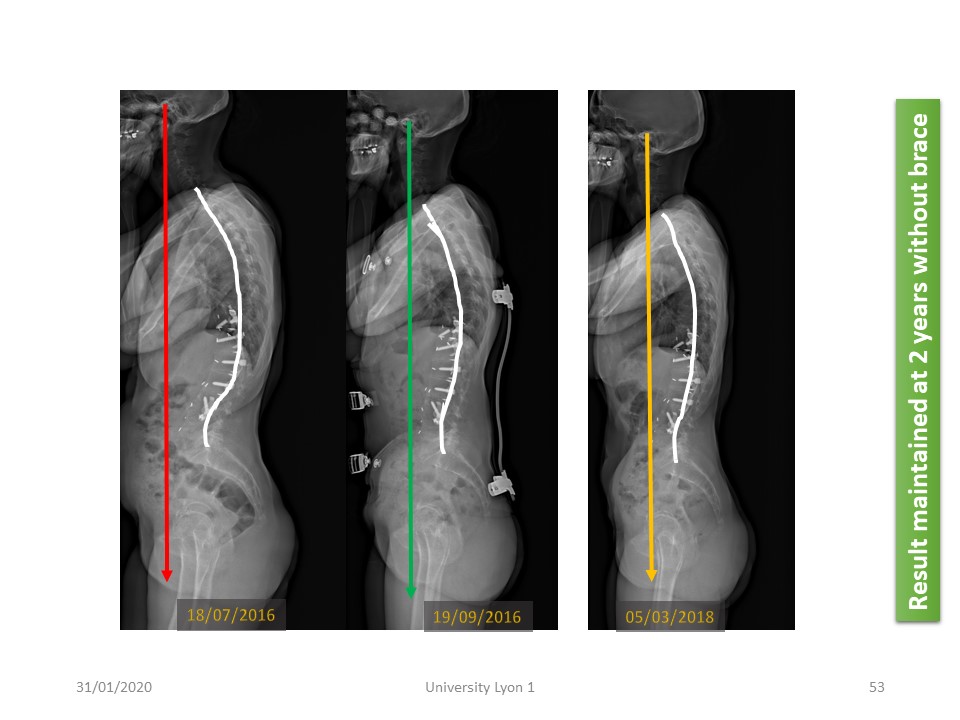 |
and the same in the sagittal plane. The improvement of thoraco-lumbar kyphosis is maintained 2 years after without brace. In conclusion, new technologies should make it possible to stabilize the spine by limiting the surgical procedures for which we know the high rate of complications at this age. The technique is simple, however the motivation of the patient remains a factor of success of these treatments.
|
 |

To register for Certification, please contact SSOL

|
")
")
")
")
")