")
")
")
")
")
 |
. |
 |
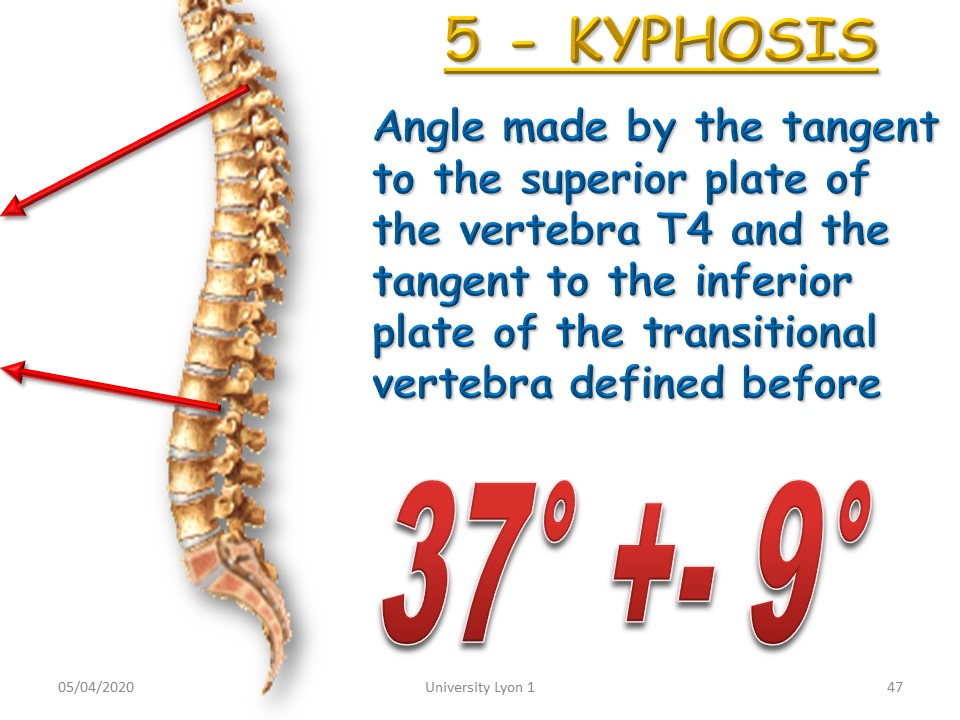
Kyphosis or hyperkyphosis is a deviation with exaggeration of the thoracic curvature in the sagittal plane. Unlike scoliosis, the surgical indications are much more limited, and it is therefore important to know how to recognize and treat them during adolescence. |
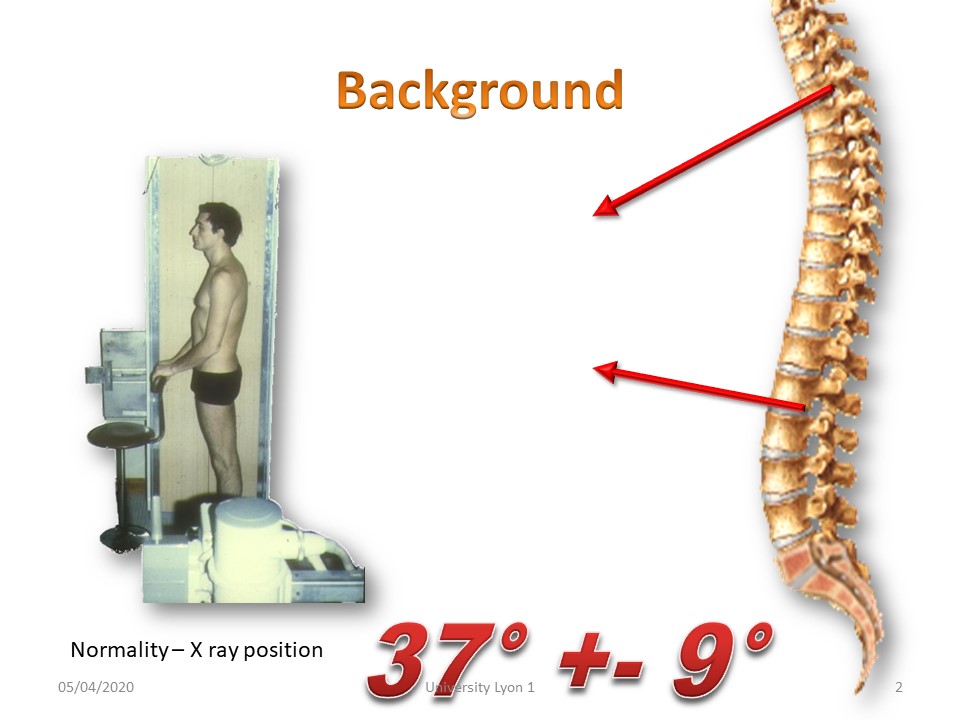 |
Another difficulty comes from the fact that, unlike scoliosis, kyphosis is physiological. One of the first researches was therefore to define the limits of physiological and pathological by a morphostatic study published in 1982. Taking T4 as the upper limit vertebra, the average angulation is 37°. |
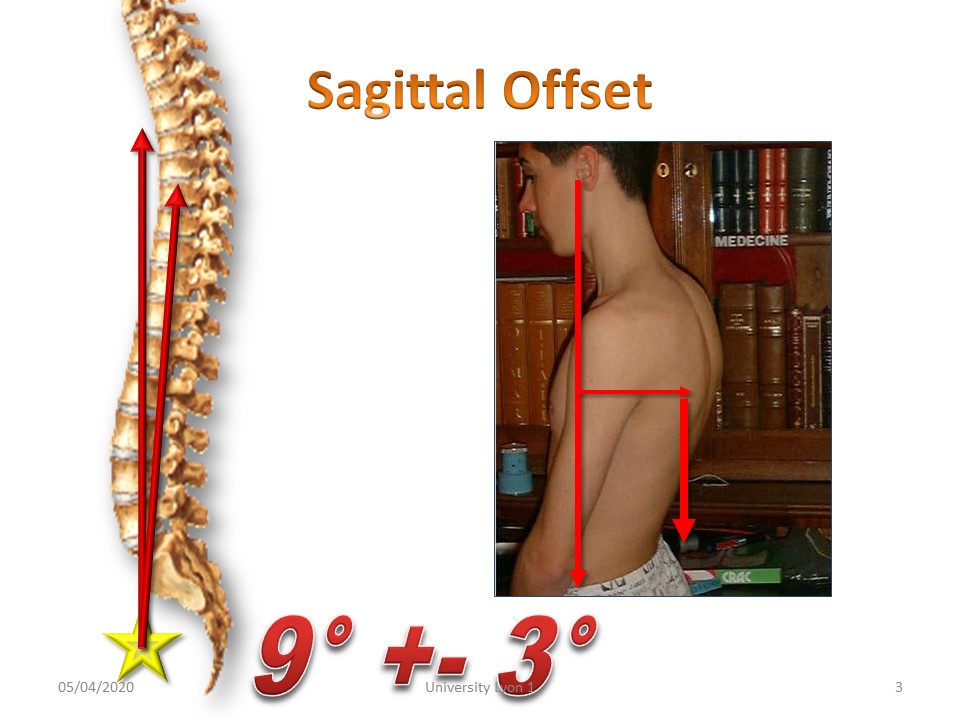 |
For the same angulation, there are significant variations depending on the patient's tone. In a hypotonic attitude, the apical vertebra moves away from the line of gravity. The sagittal offset increases. |
 |
Unlike scoliosis, most vertebrates have a dorsal kyphosis with sometimes a true hyperkyphosis as in this Belgian canary. |
 |
Unlike adolescent scoliosis, kyphosis is often painful. It should be sought clinically by the percussion of the spines, because the adolescent lives in the present time and does not memorize the pain. |
 |
|
 |
Unlike scoliosis, kyphosis is visible, which can have psychological repercussions that are well expressed in mythology. |
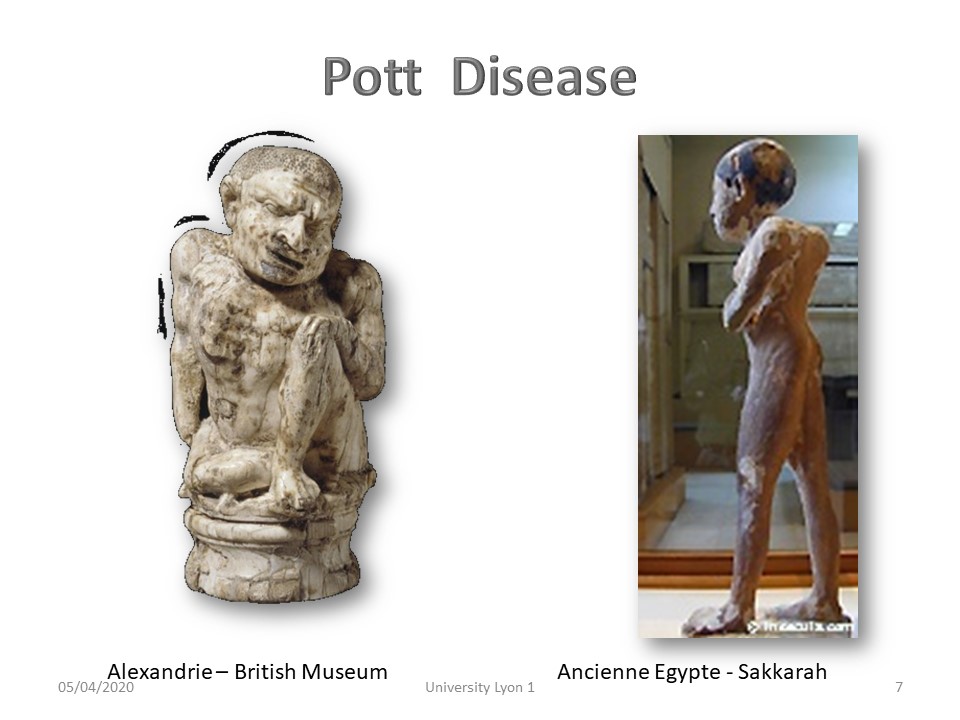 |
In Egyptian antiquity many kyphosis representations probably of Pott’s origin reflect their good integration into society. |
 |
Aesop the fabulist also had a kyphosis. “Nature put in an ugly body an excellent spirit” |
 |
The Gospel of Saint Luke describes the miracle of the humpbacked woman that Jesus will straighten. |
 |
Righteousness is one of the characteristics of Christianity and only one statue represents a kyphotic man supporting the stoup of Saint Anastasia in Verona. |
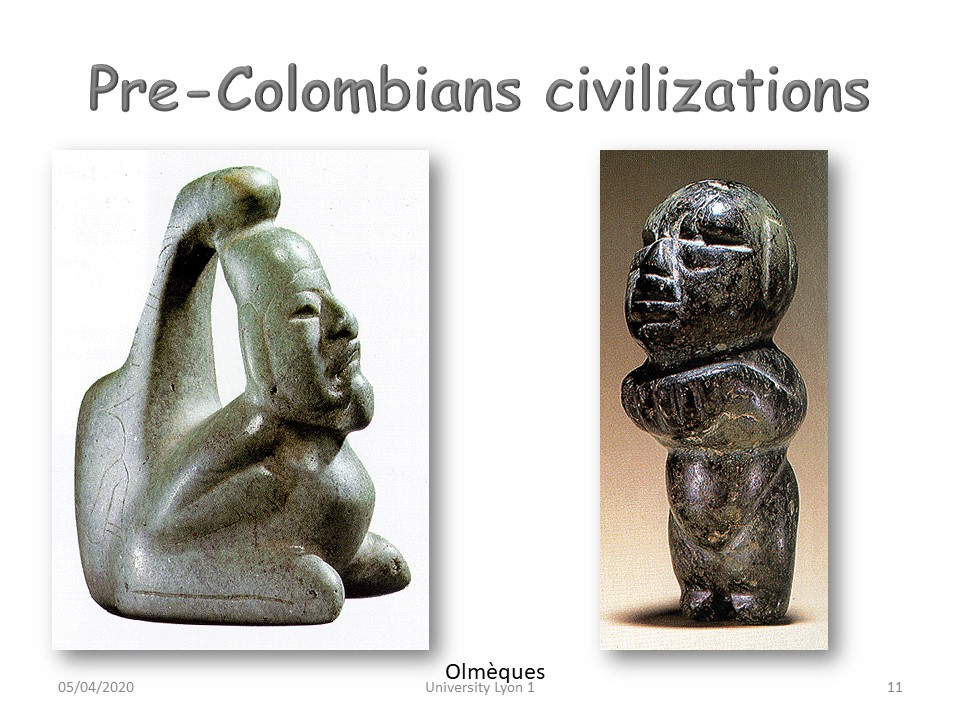 |
Pre-Columbian civilizations also used to represent kyphosis as in these Olmec sculptures. |
 |
The Olmecs had a very advanced civilization that was at the origin of the Aztecs and Mayans who inherited the famous calendar. Like the Egyptians, their civilization seems to rise abruptly to an advanced level. |
 |
Indeed, we recognize the same style among the Incas and the Mayans. |
 |
One of Charlemagne's sons had kyphosis. He was the only one to foment a revolution in the palace and ends his days in a monastery. |
 |
In the Middle Ages, the hunchback had a special role in times of absolute monarchy. He is the only one who can speak frankly to the king. This myth will be widely taken up by Rabelais, Victor Hugo and Verdi. |
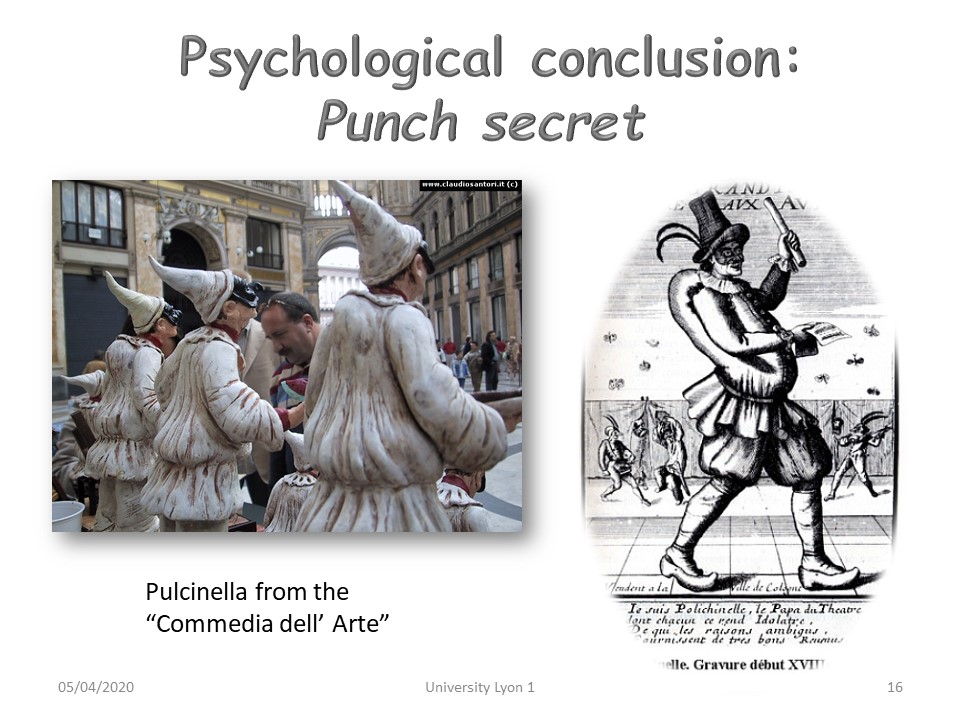 |
In the "Commedia del Arte", the backward kyphosis is compensated by the protrusion of the belly forward. |
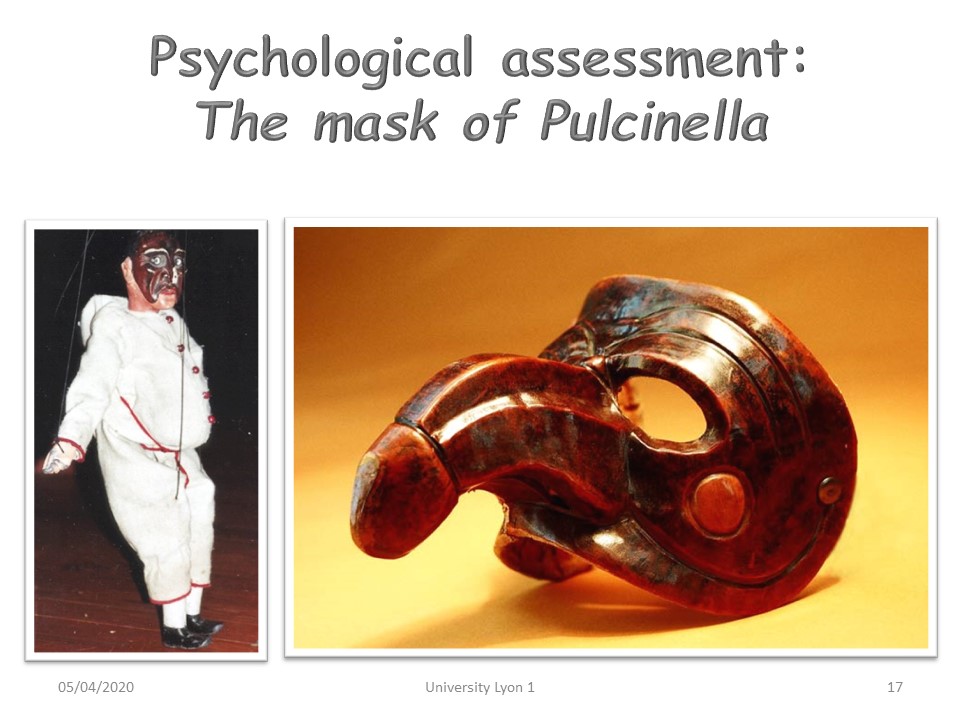 |
In addition to the fact that touching the bump brings luck, a phallic image is often associated with kyphosis. |
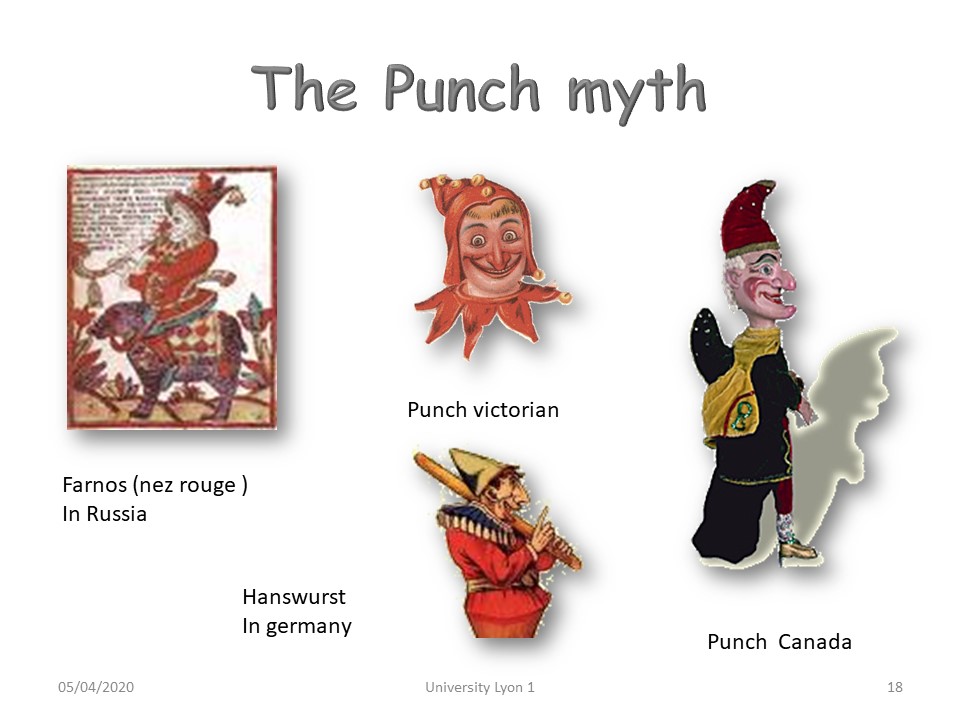 |
All European civilizations have taken up the myth of the hunchback. |
 |
At the beginning of the 20th century with the birth of cinema, the hunchback is the one who is trusted and consequently he is often the executor of dirty works. |
 |
|
 |
Early detection is important when it is done by the same examiner, which is not always the case in hospital. |
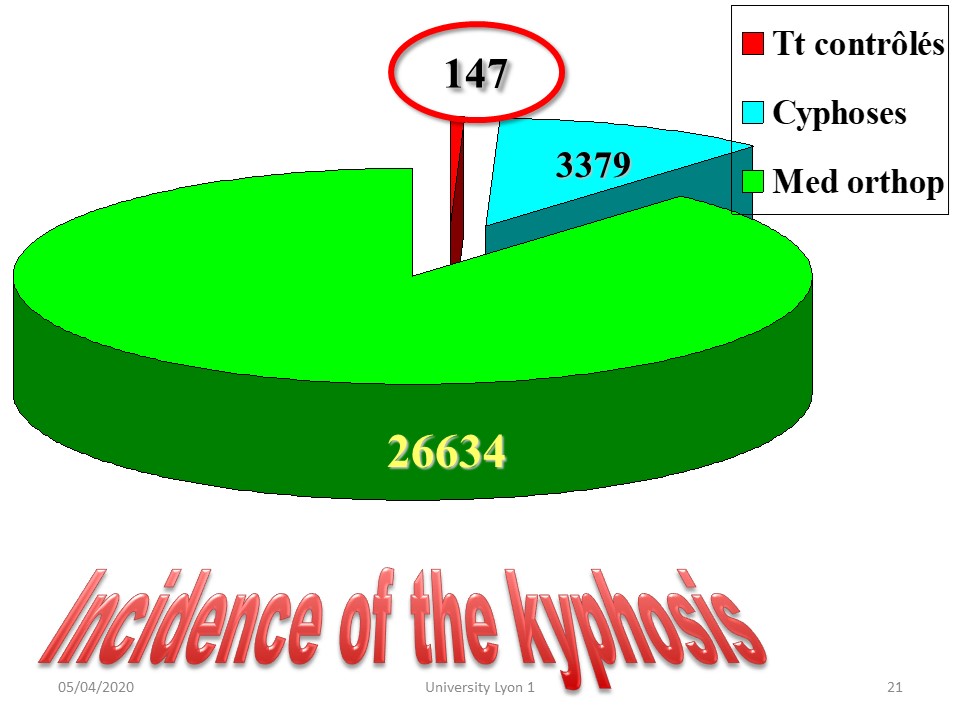 |
Kyphosis concerns 13% of orthopaedic medicine consultations. Brace treatment of kyphosis remains exceptional: about 5% of the consultants. |
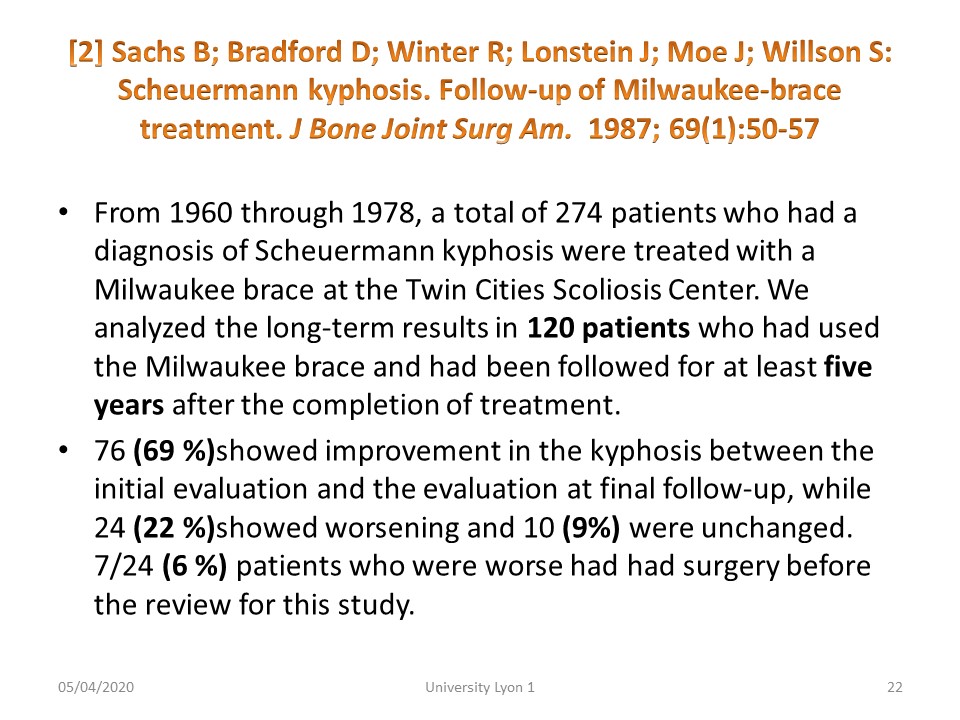 |
Few results are published in the literature. Sixty years ago, kyphosis was treated with the Milwaukee brace. Nearly 70% of patients improved. |
 |
|
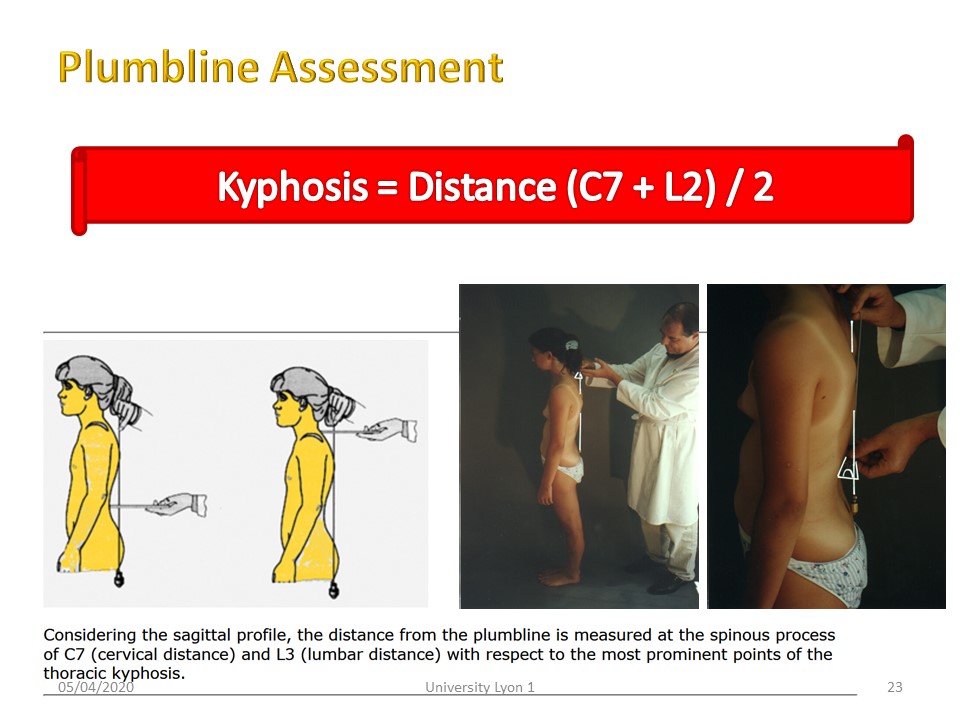 |
The measurement of the kyphosis arrows is indirect, it corresponds to the half sum of the cervical arrow at C7 and the lumbar arrow at the lordosis maximum concavity (usually L2). |
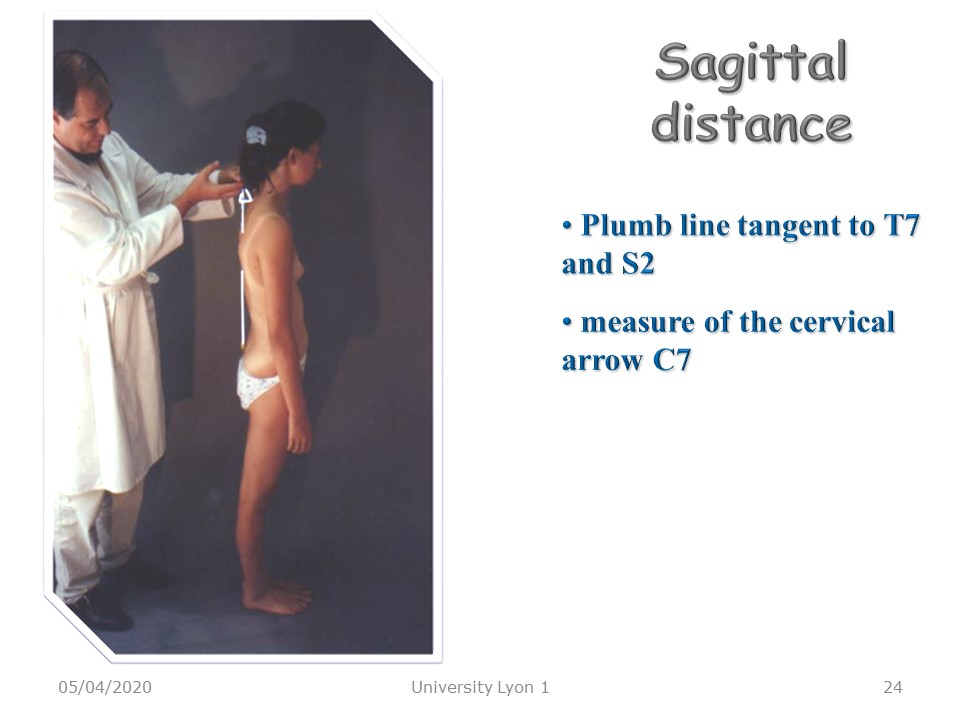 |
The sagittal arrows are noted: Cervical lordosis arrow in T1. Usually the plumb line is tangent to T7. In scoliosis, the existence of a flat back is appreciated at this level. Lumbar lordosis arrow in L2, sagittal unbalance, when the plumb line is at a distance from S2. |
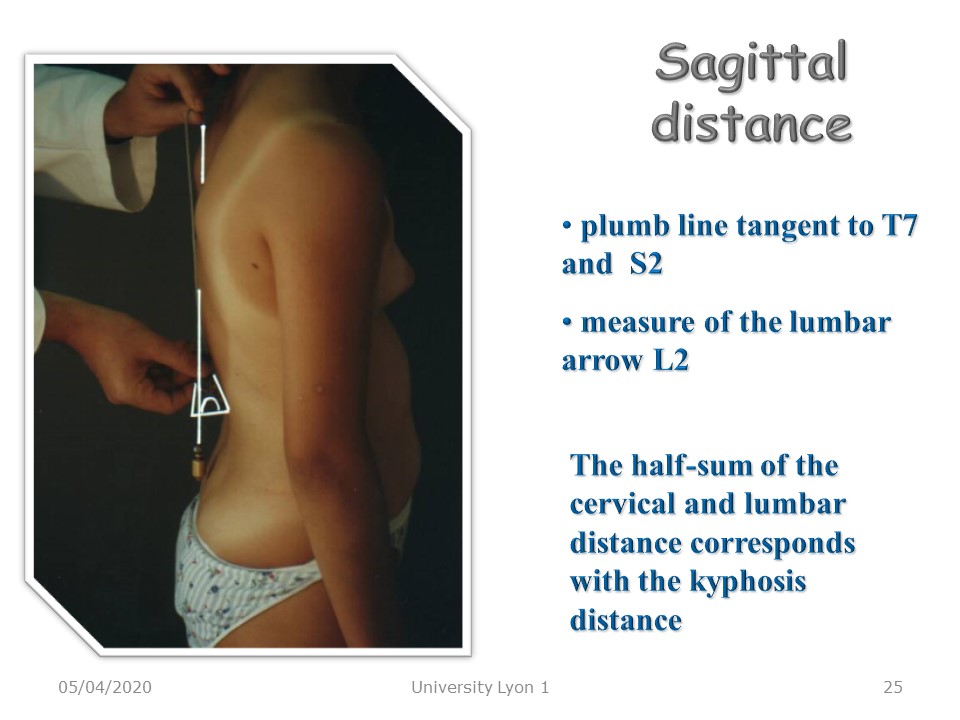 |
Here, measuring the lumbar arrow. |
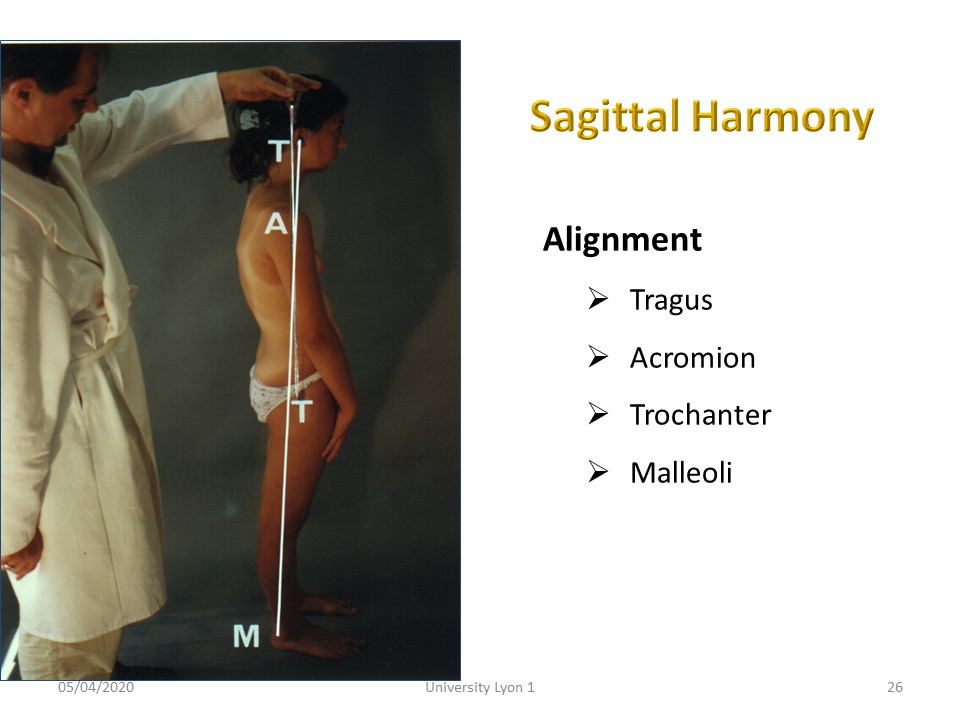 |
The overall balance of the spine can be assessed by looking at the alignment of the Tragus, Acromion, Trochanter and Malleolus. |
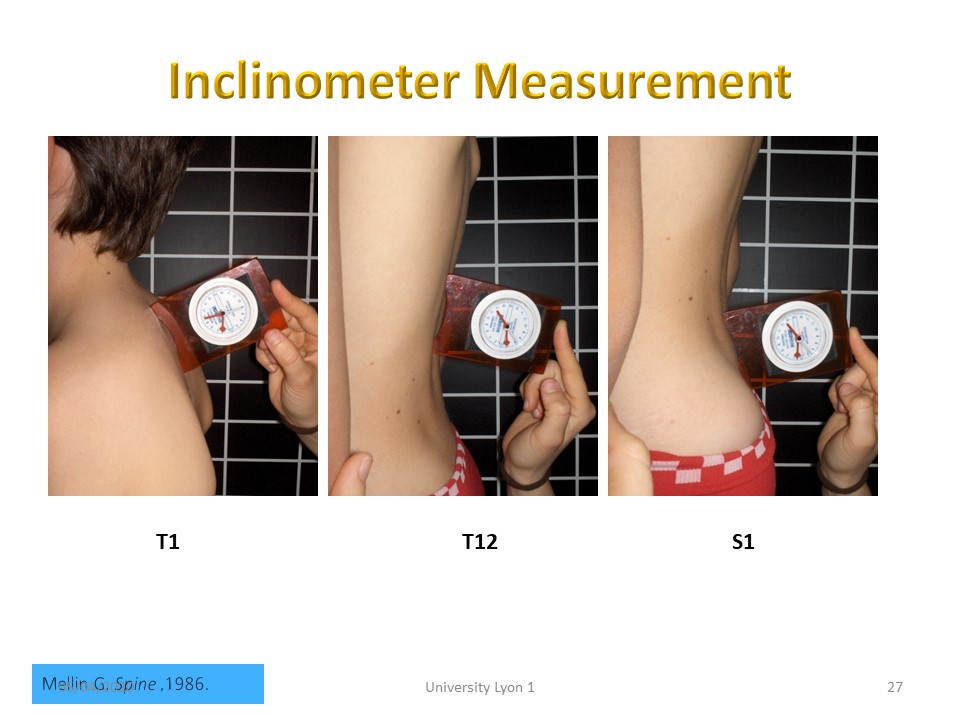 |
The inclinometer also makes it possible to appreciate the kyphosis which corresponds to the sum of the angles in T1 and T12. |
 |
The reference position is fundamental. The lower limbs are in a position of standing at attention to you. The feet are joined, in rotation 0, i.e. the malleolus-big toe lines are parallel. The upper limbs and shoulders are relaxed. The palms of the hands are aligned with the outside of the thighs. |
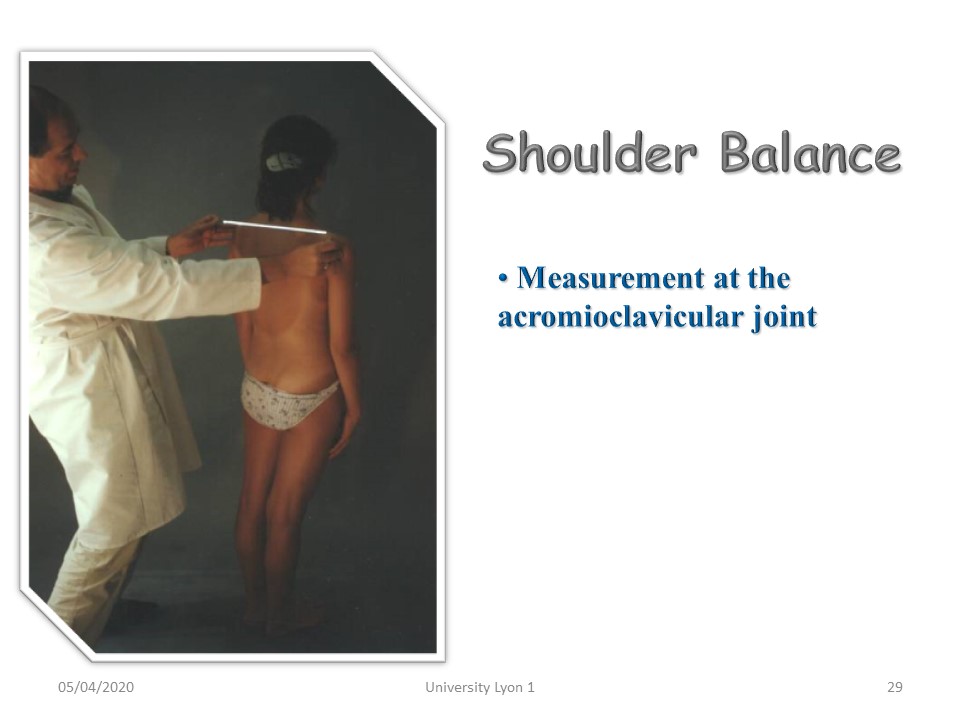 |
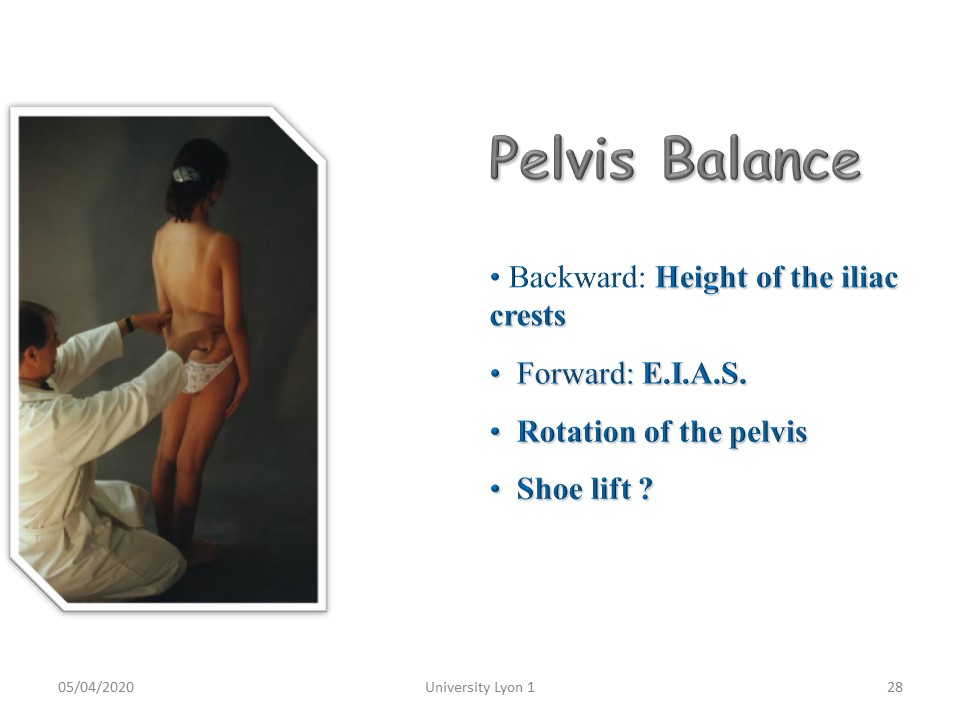
A possible unevenness of the shoulders will be noted. |
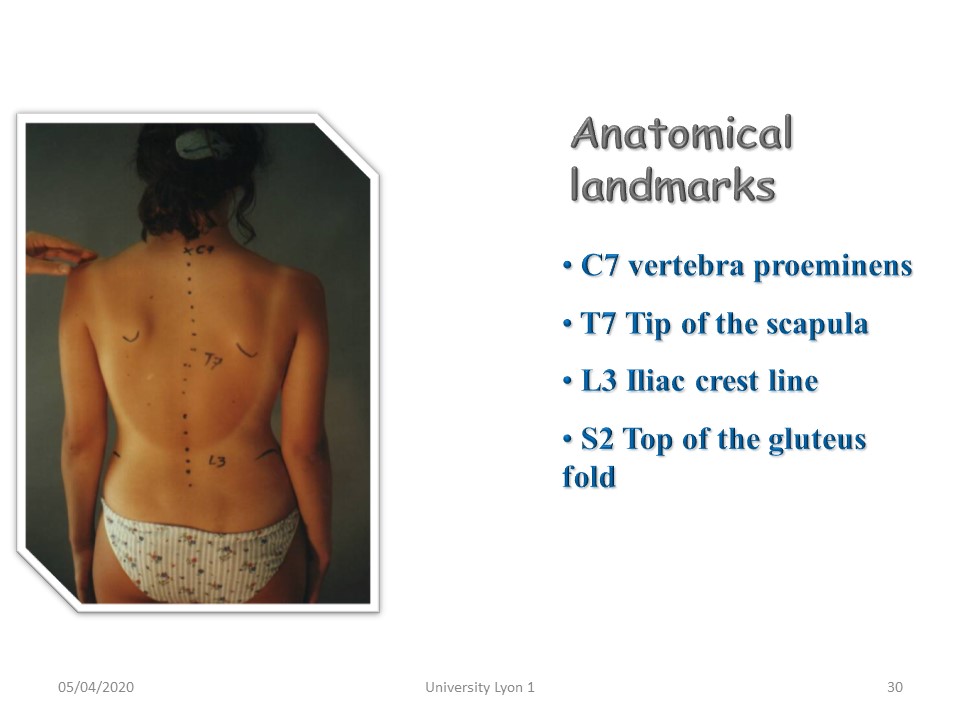 |
The skin landmarks are possibly underlined with a dermographic pencil: - T1 is located opposite the most prominent C7 spine or vertebra proeminens at the base of the nape of the neck. - T7 lies opposite the point of the shoulder blades, - L4 lies opposite the iliac bi-crest line, - S2 lies at the top of the gluteal fold will be noted. |
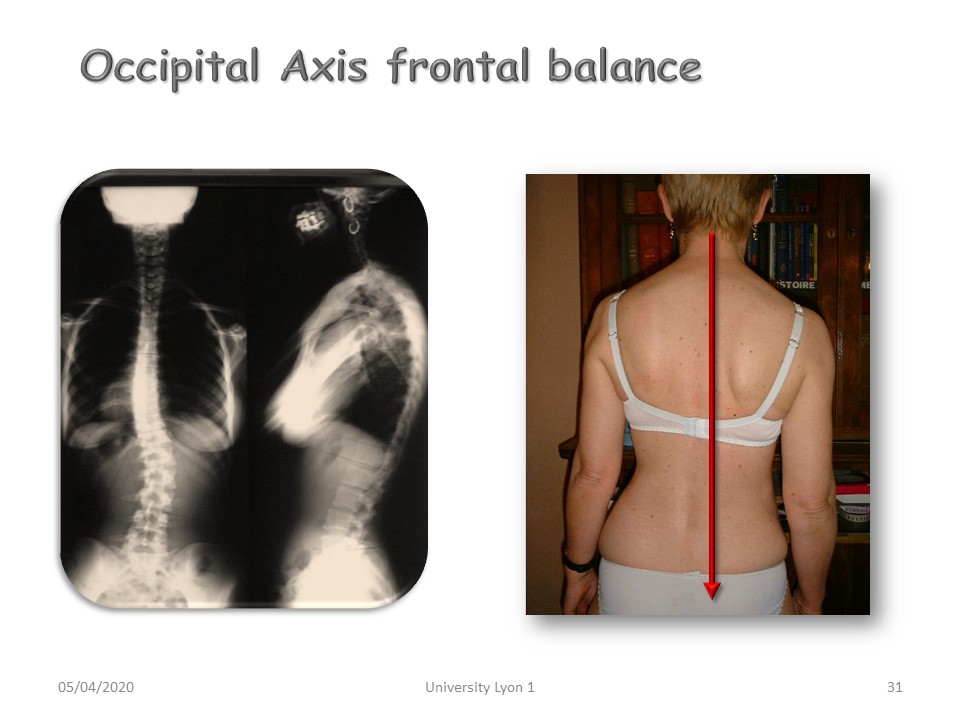 |
The offset of the occipital axis is appreciated by pointing the plumb line at the C7 spine. Note the offset of the top of the gluteal fold (S2) in relation to the plumb line. |
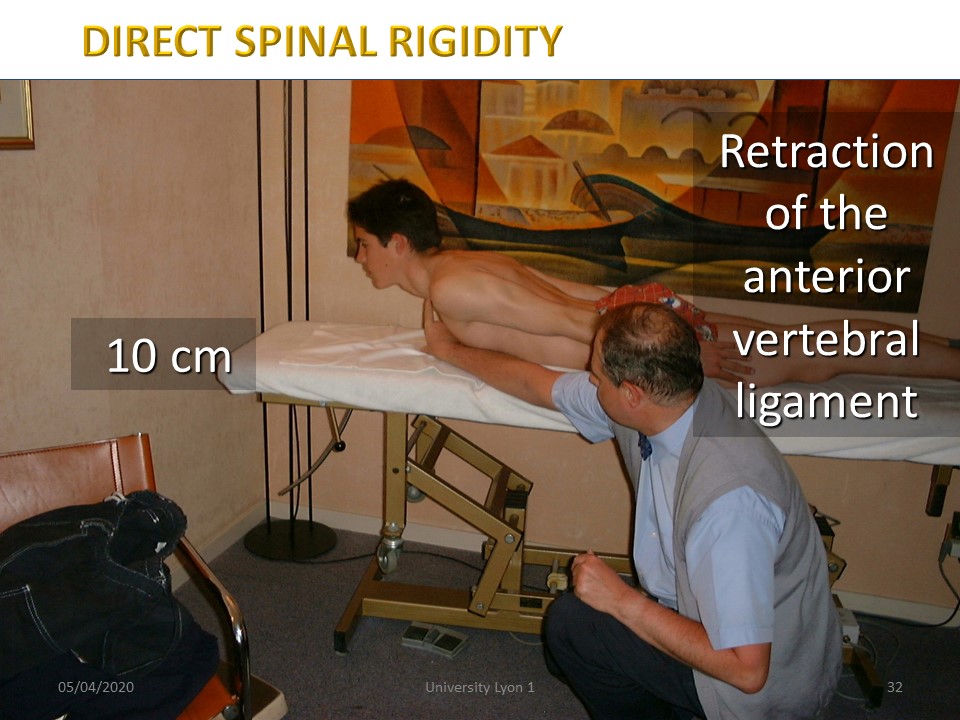 |
Direct rigidity. We're measuring the manubrium-table distance. The reducibility is an essential element for the indication of a brace. Rigidity corresponds to a retraction of the posterior longitudinal common ligament which will no longer be accessible to physiotherapy alone. |
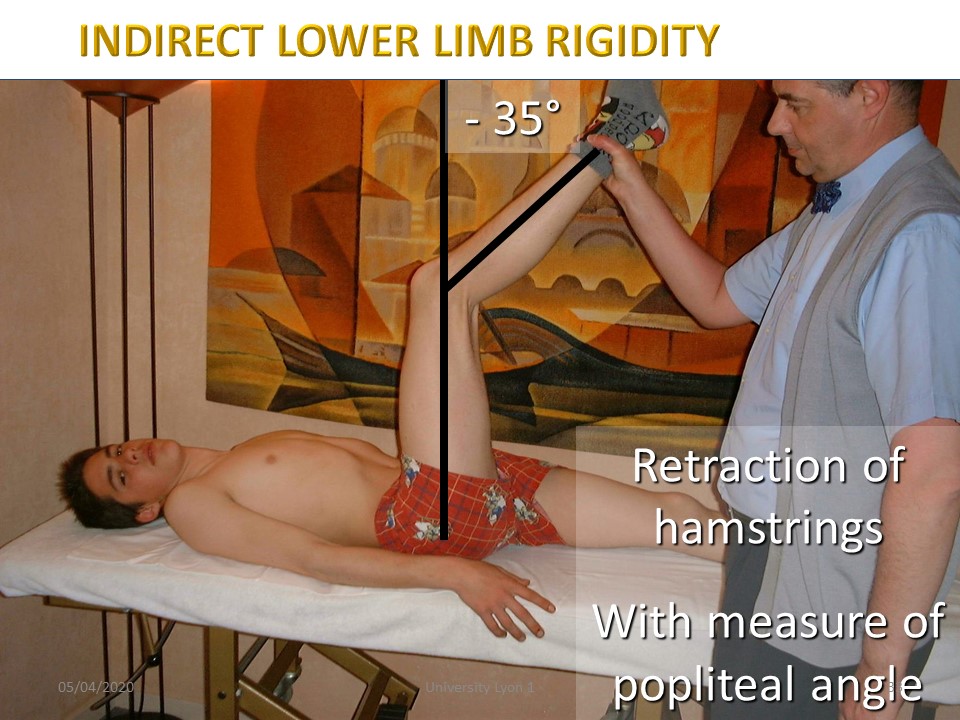 |
Indirect rigidity: hamstrings. We measure the angle missing to reach the vertical. The popliteal angle is used to assess the elasticity of the ligaments. It is little modified by physiotherapy. |
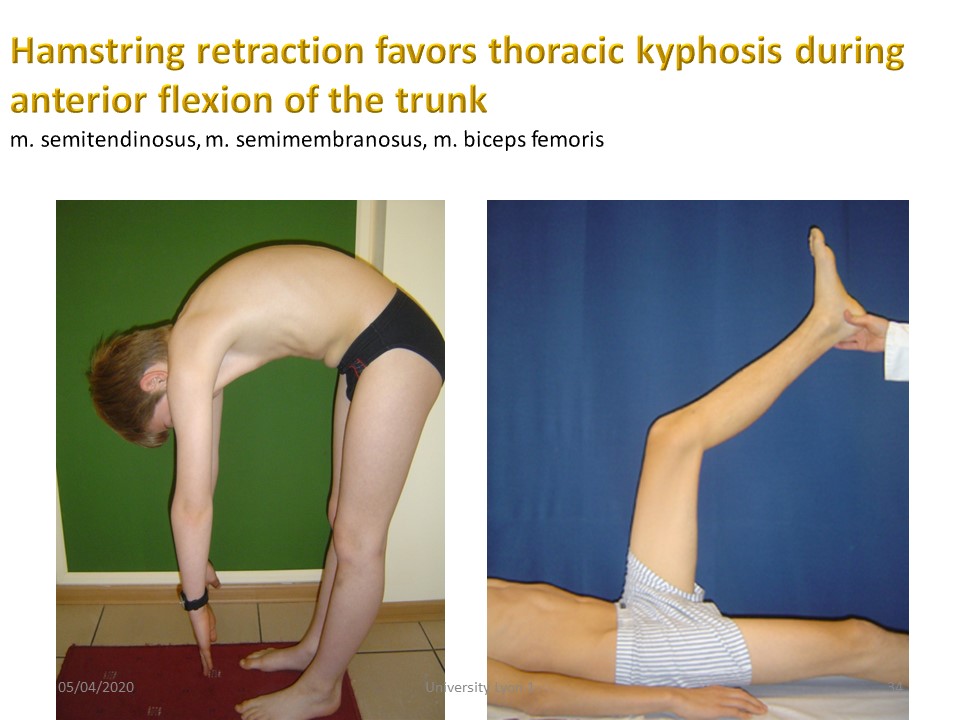 |
Retraction of the hamstrings promotes thoracic kyphosis during anterior trunk flexion. |
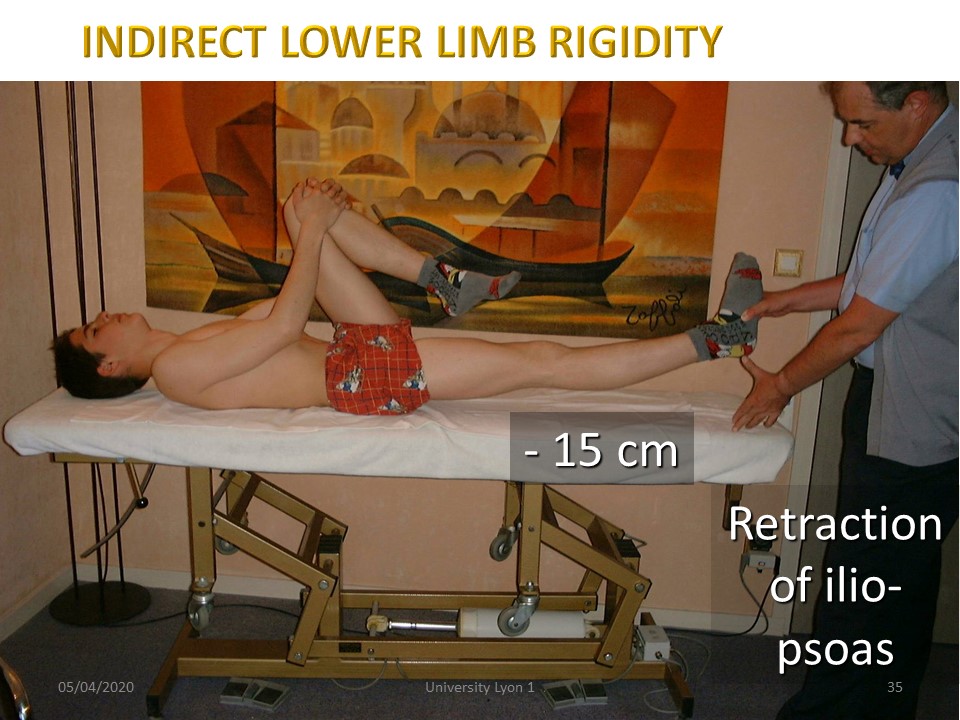 |
The ilio-psoas is in direct continuity with the posterior longitudinal ligament, which it will extend to the lower limbs. Its retraction causes a pelvic anteversion that can only be corrected by a hip flexum. |
 |
Pectoral retraction is measured by the elbow-to-table distance. It often accentuates the rolling of the shoulders forward. |
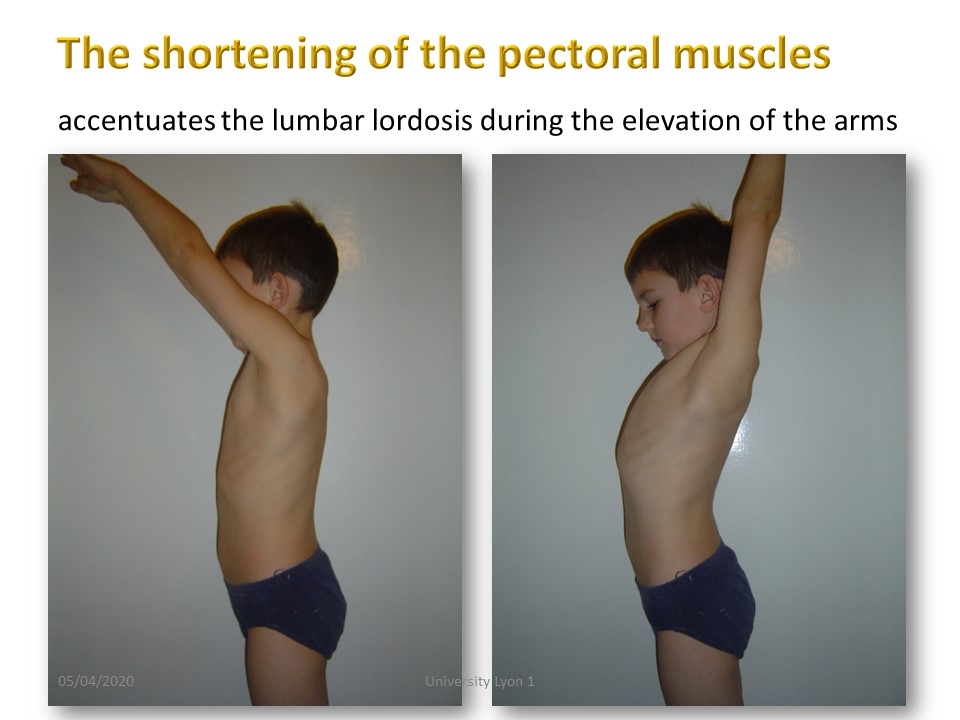 |
The retraction of the pectoral muscles during the elevation of the upper limbs will accentuate the lumbar lordosis. |
 |
|
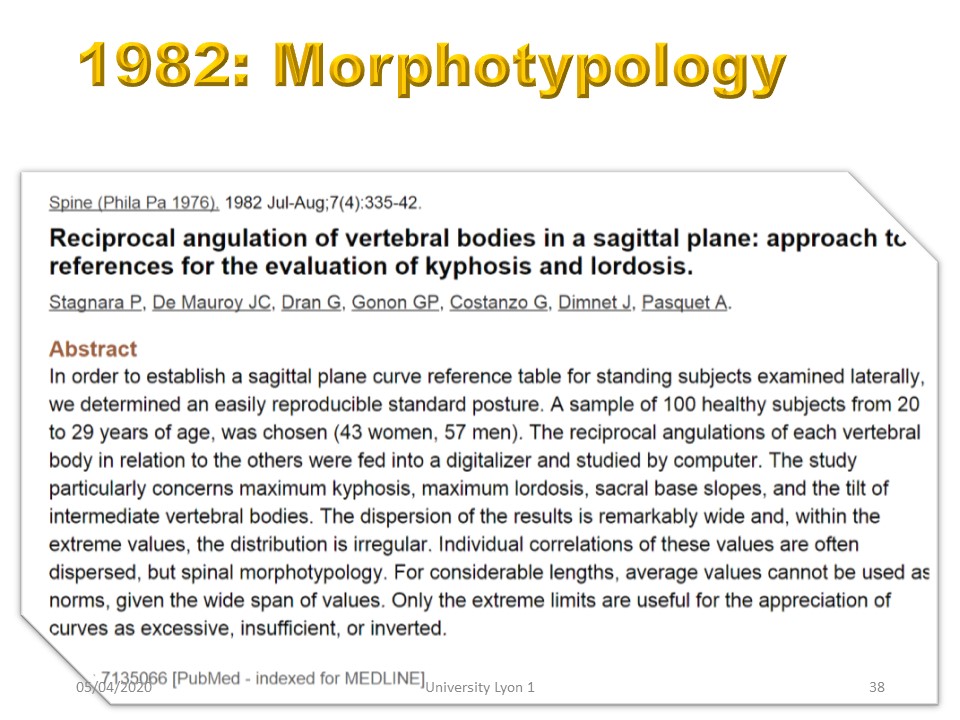 |
In 1982, we studied the radiological morphotypology of 100 normal subjects aged between 20 and 30 years. Angular distributions are normal without defining types. The standard deviation makes it possible to specify the limits of the physiological and pathological. |
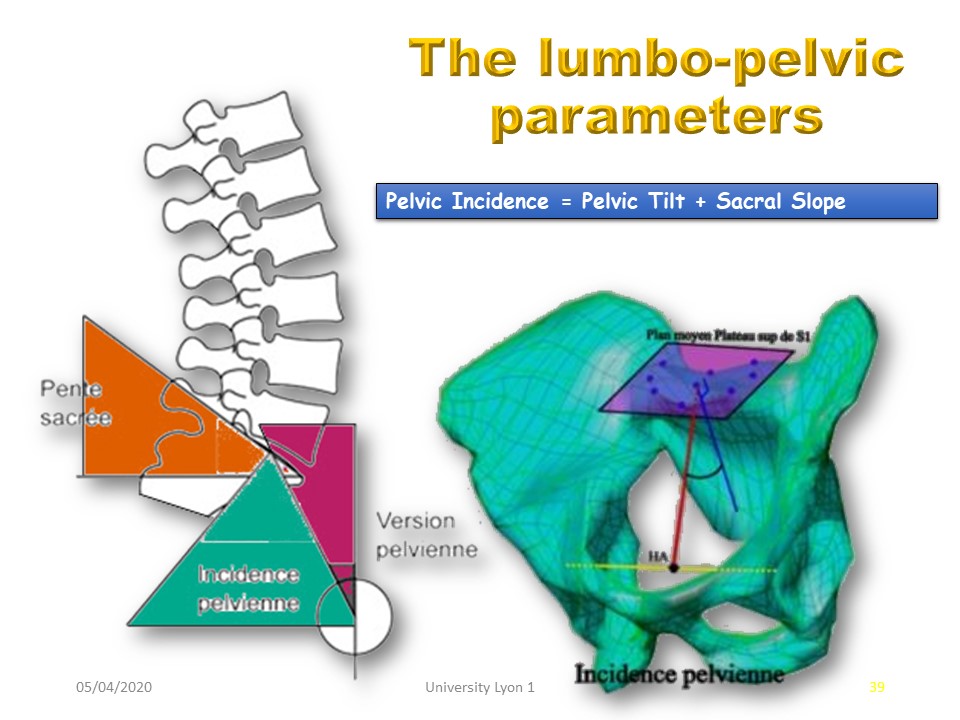 |
The lumbo-pelvic parameters were defined in a second step by Mrs. Duval-Beaupère. Pelvic incidence is a constitutional parameter. The sacral slope is correlated with lordosis. The adjustment is made by the pelvic version. The pelvic belt must take these parameters into account. |
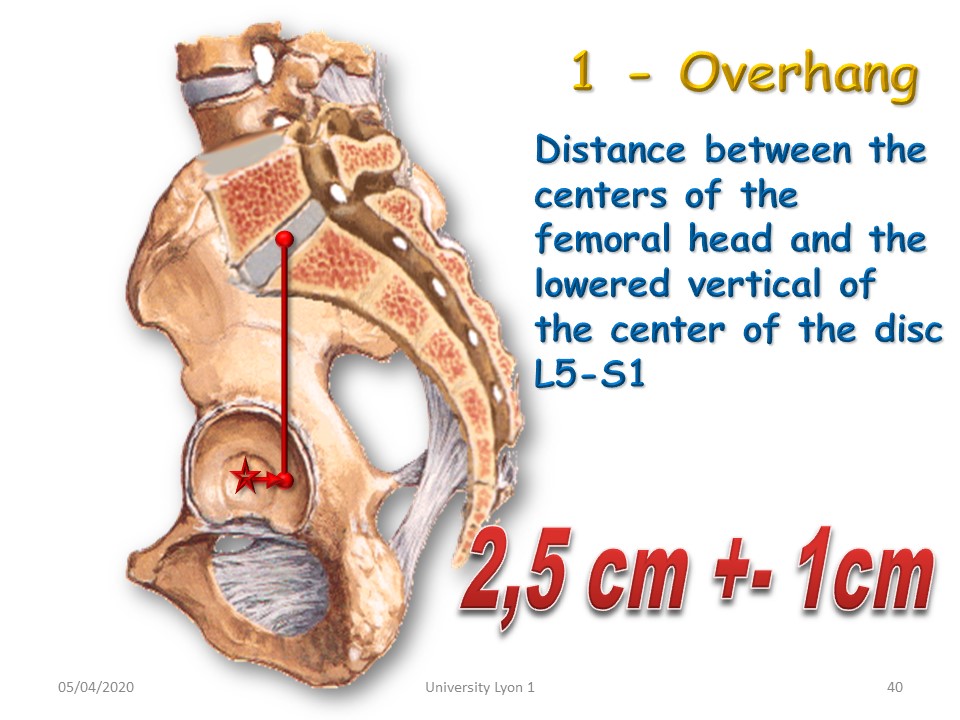 |
The overhang is determined by the position of the nucleus of the L5-S1 disc in relation to the centre of the femoral head. Normally, the nucleus projects 2.5 cm behind the femoral head. When it projects forward, it is called anteversion, and when it projects backward, it is called retroversion. The pelvic version of the ARTbrace is checked during casting no. 1 according to the following radiological parameters. |
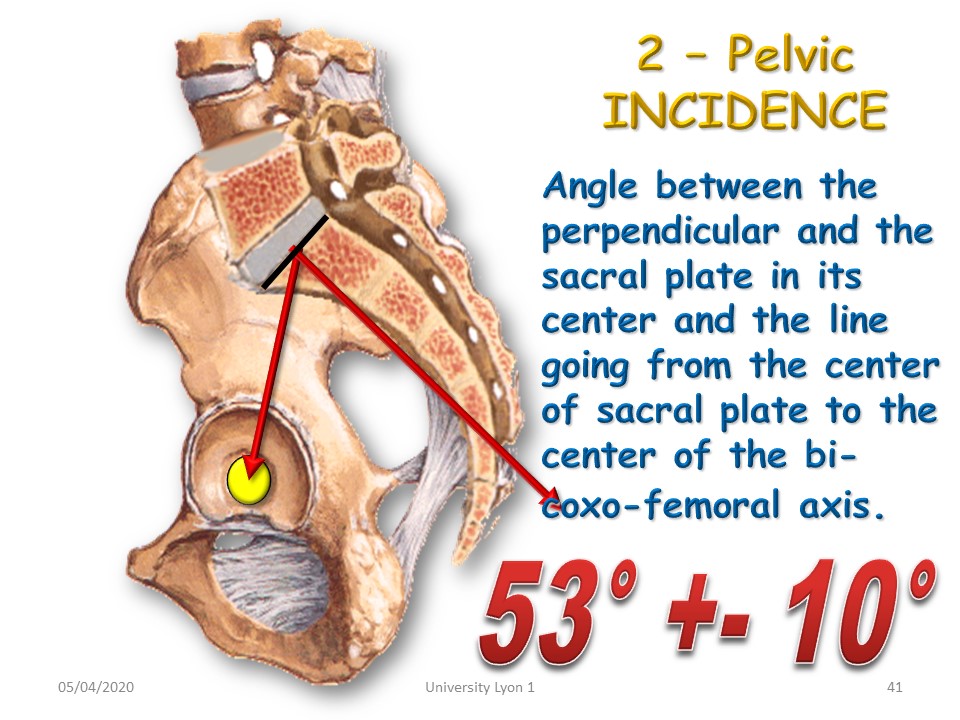 |
Pelvic incidence is defined by the angle formed by the perpendicular to the centre of the plateau of S1 and the line joining the centre of the acetabulum. This angle is constitutional and is not modified by the pelvic version. It is equal to the sum of the inclination of the sacral slope to the horizontal (37°) + the pelvic version (16°). In case of normal incidence all defects can be corrected. If it is pathological, it will have to be compensated by adapting the sitting position. During the growth period, treatment with a brace can slightly modify this angle. |
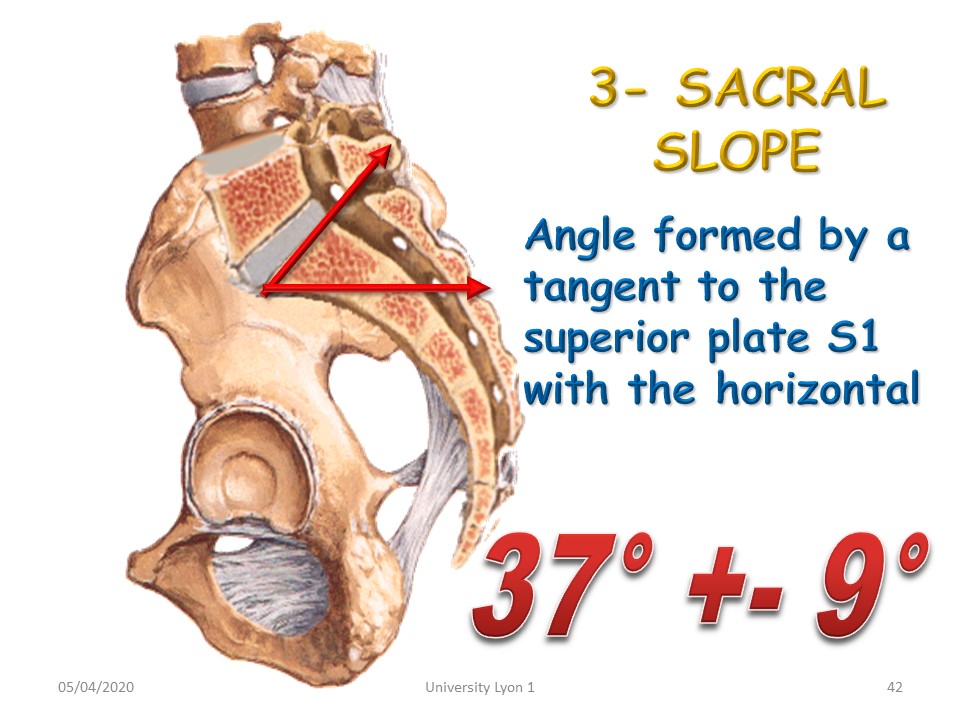 |
The inclination of the sacral slope is on average 37°. It varies according to the pelvic version. 1st case: normal pelvic incidence (53°). Excessive inclination with anteversion and hyperlordosis is corrected by pelvic retroversion positioning. A slight tilt with retroversion and hypolordosis is corrected by positioning in anteversion. 2° case, there is an abnormal incidence. The patient is placed in a neutral pelvic position and the sitting position is modified: - Low incidence = sitting in a kneeling position, - High incidence = use of a triangular cushion on the seat. |
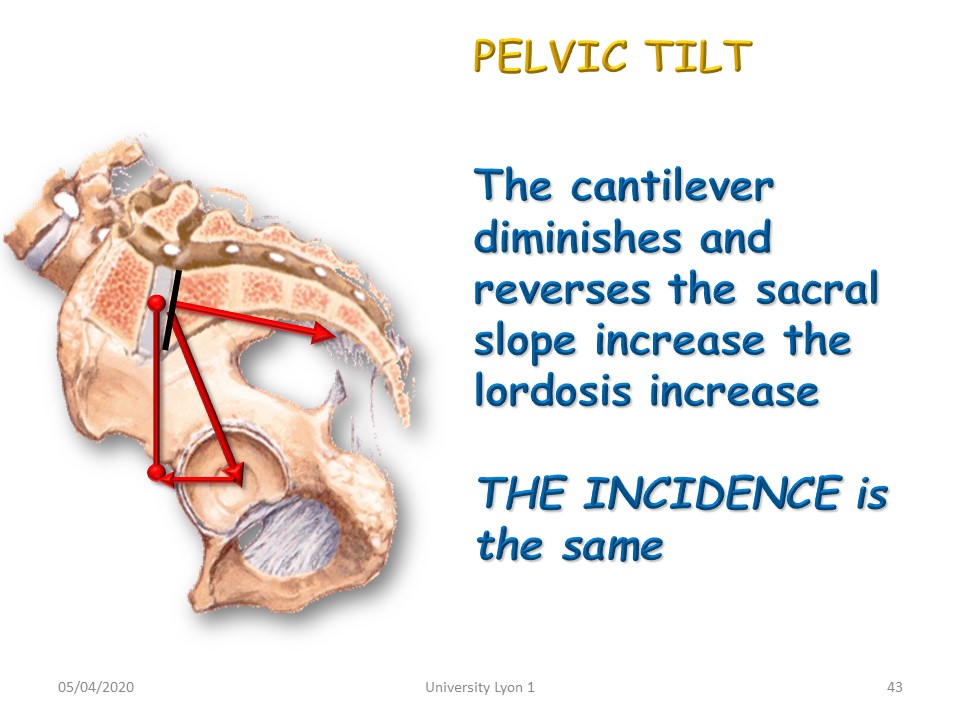 |
Pelvic anteversion projects the L5-S1 disc in front of the acetabulum and increases the inclination of the sacral slope and the lordosis. |
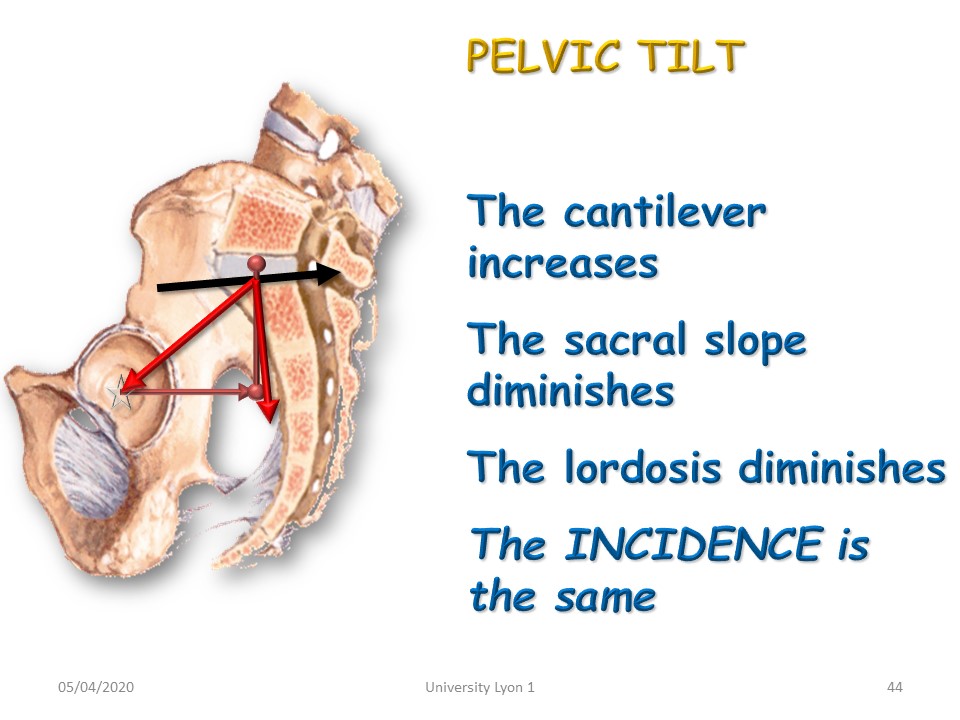 |
On the contrary, pelvic retroversion moves the L5-S1 disc away from the centre of the femoral head, decreasing the inclination of the sacral slope to the horizontal and lordosis. The pelvic incidence remains the same. |
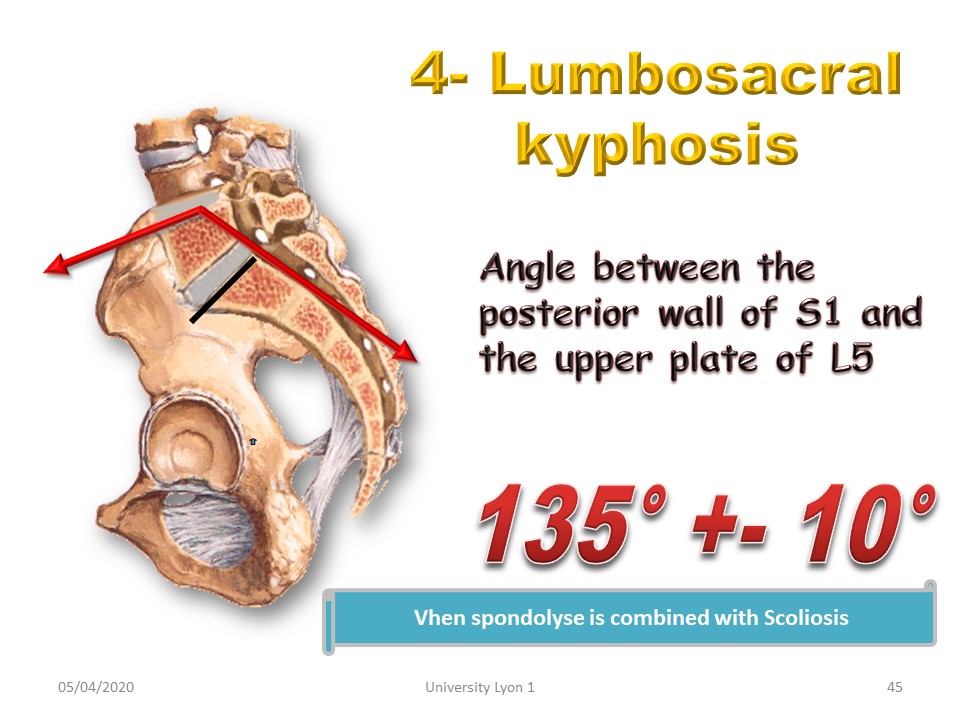 |
20% of lumbar scoliosis is associated with spondylolisthesis. The evolutionary prognosis is determined by lumbo-sacral kyphosis: 135° = Normal and 110° = brace, 90° = surgical discussion. |
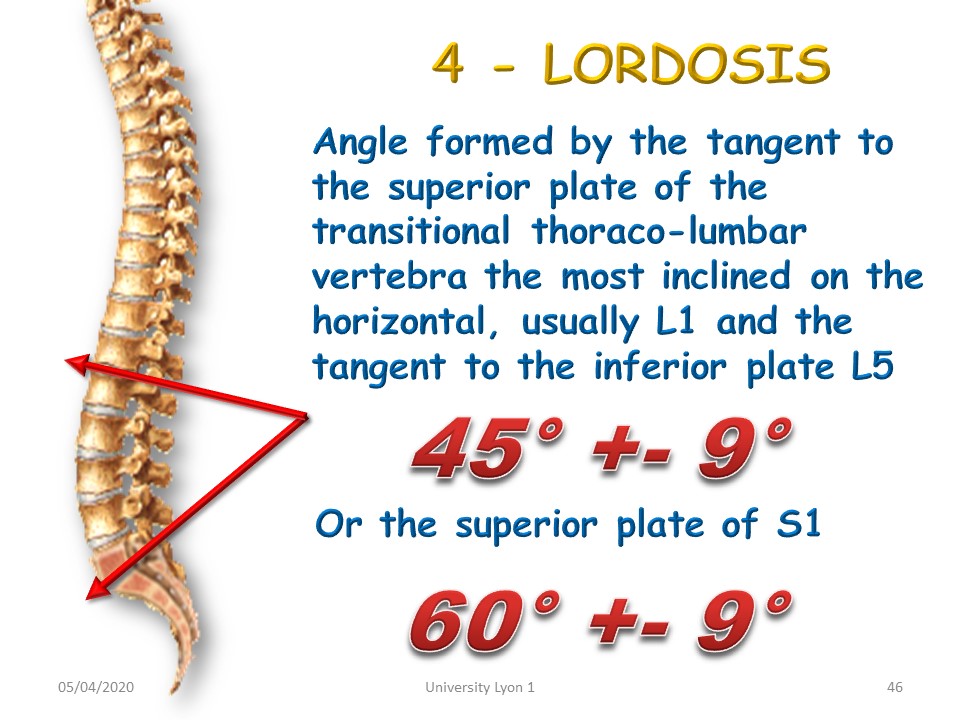 |
The lumbar lordosis is the angle formed by the lower plateau of L5 and the upper plateau of the transitional vertebra (the most inclined to the horizontal at the thoracolumbar hinge). It is correlated to the inclination of the sacral slope to the horizontal. The majority of braces strongly reduce lordosis (12° for the Boston). Thoracic kyphosis cannot be recreated in the case of a flat back without underlying lordosis. Casting n° 2 will therefore be made in physiological lordosis. |
 |
The angle of the kyphosis is formed by the lower plateau of the transitional thoracolumbar vertebra and the upper plateau of the most inclined vertebra at the cervico-thoracic level. The kyphosis angulation is currently measured up to T1 using EOS. Half of the scoliosis is associated with a flat back with angulation less than 30°. Casting n° 3 is performed in thoracic kyphosis. |
 |
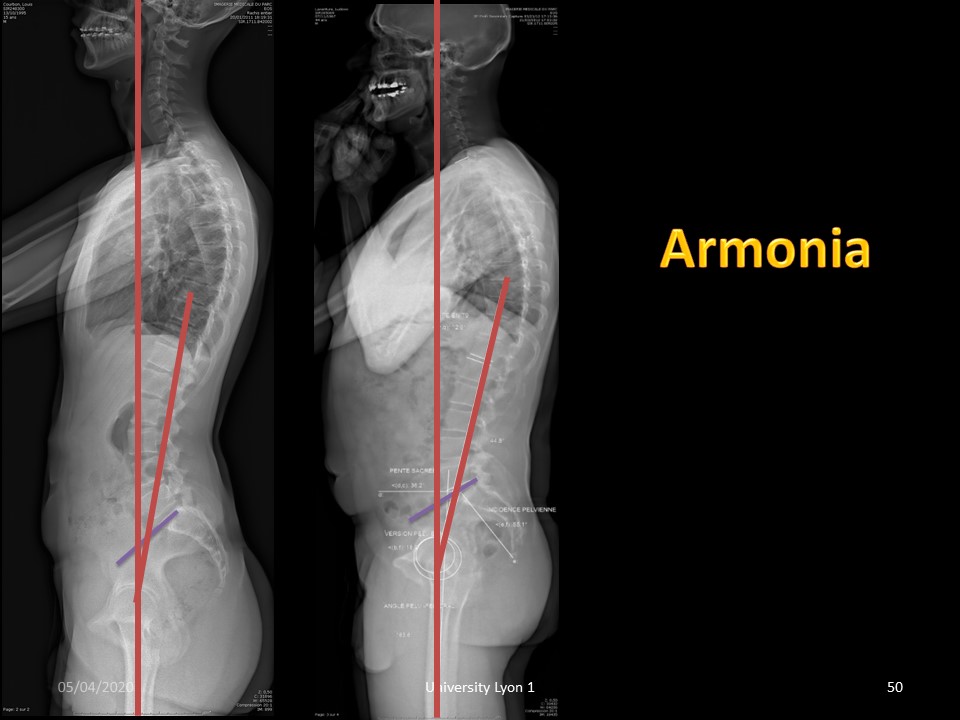
This regular medium thoracic kyphosis is disharmonious, unmatched by underlying lordosis. |
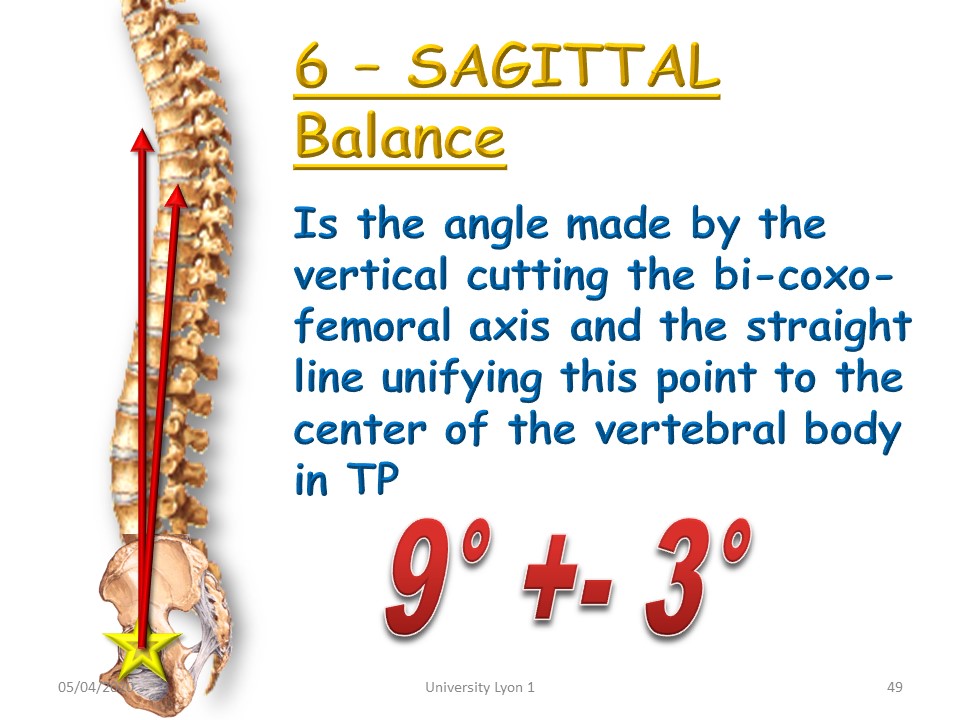 |
The sagittal offset allows the projection of the trunk forward or backward to be measured. It is the angle formed by the vertical at the centre of the femoral heads and the line joining the centre of the vertebral body of T9. |
 |
The increase of this angle corresponds to an accentuation of the kyphosis not compensated by an underlying lordosis. |
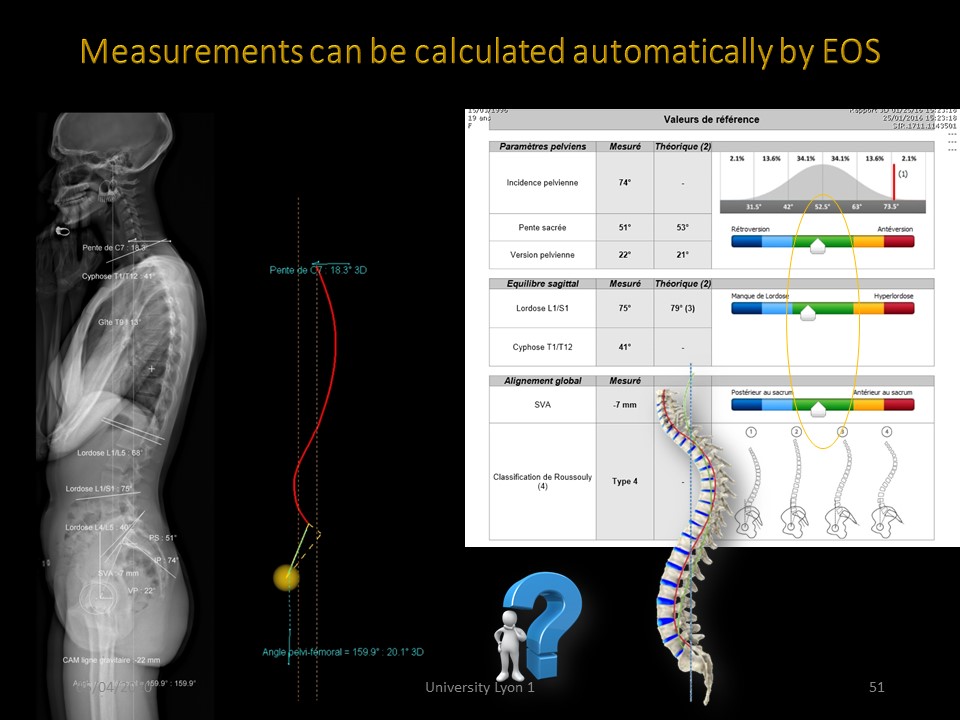 |
It is possible with EOS to automatically measure these parameters and specially to see if they are moving away from predictable data as a function of pelvic incidence. However, thoracic kyphosis is not correlated with other parameters. Here all the parameters are in the green zone, ie the equilibrium is ideal. |
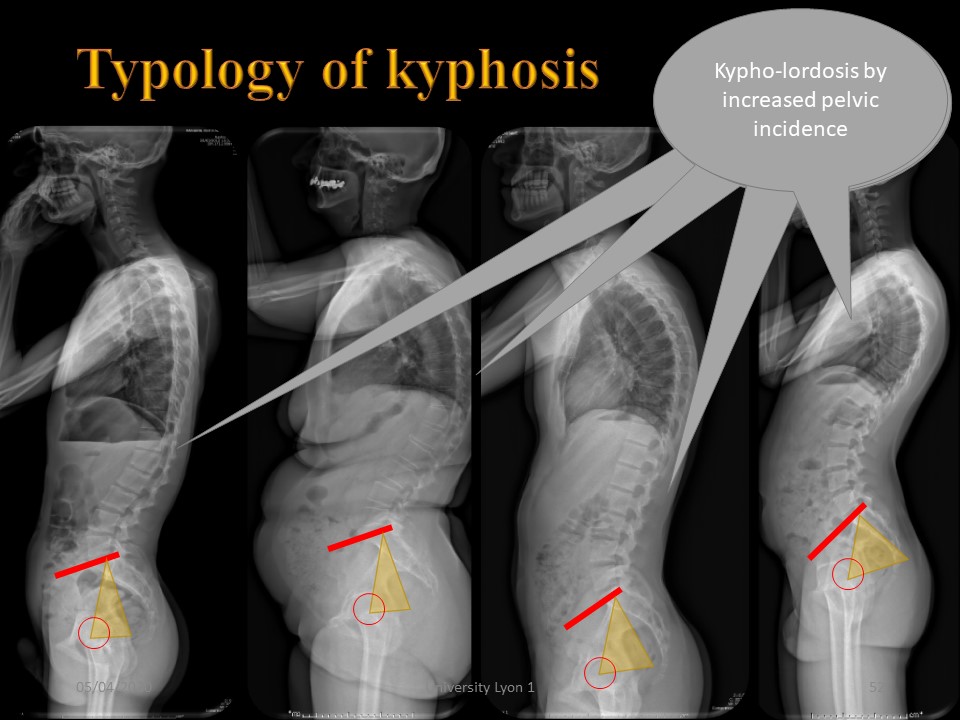 |
Typology of kyphosis may vary with pelvic incidence. 1. Low incidence promotes thoraco-lumbar kyphosis. 1. Low incidence promotes thoraco-lumbar kyphosis with flat back 2. or extension of thoracic kyphosis. 3. Normal incidence with thoracic kyphosis and hypolordosis. 4. Kypho-lordosis by increased pelvic incidence. |
 |
The morphostatic of children aged 5 to 20 years was studied by Voutsinas and Mac Ewen and completes our work done between 20 and 30 years. |
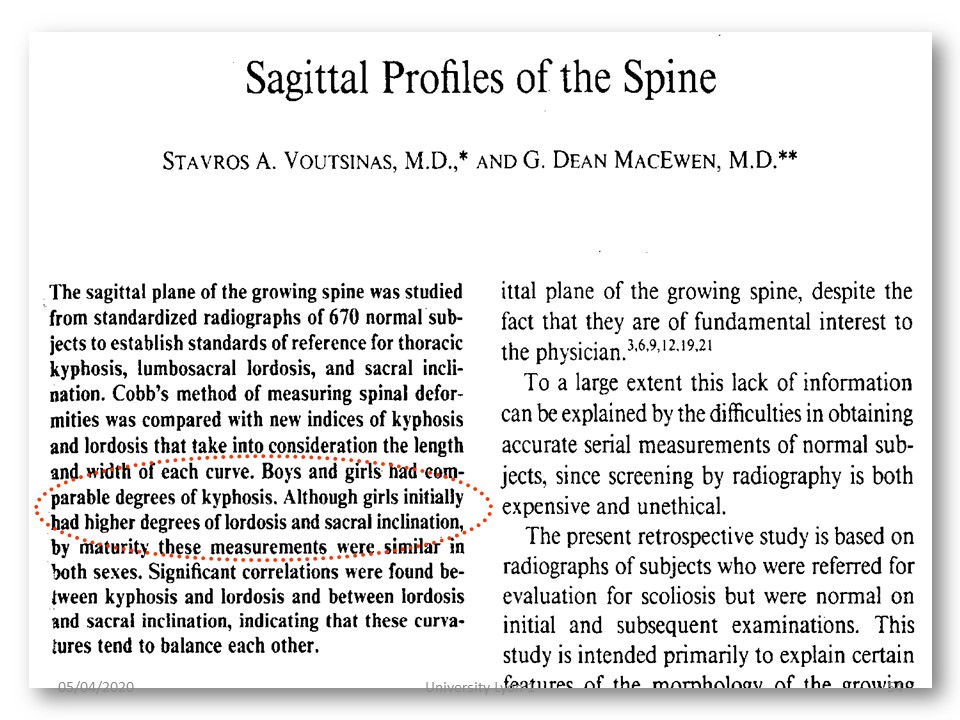 |
There are comparable numbers between boys and girls. |
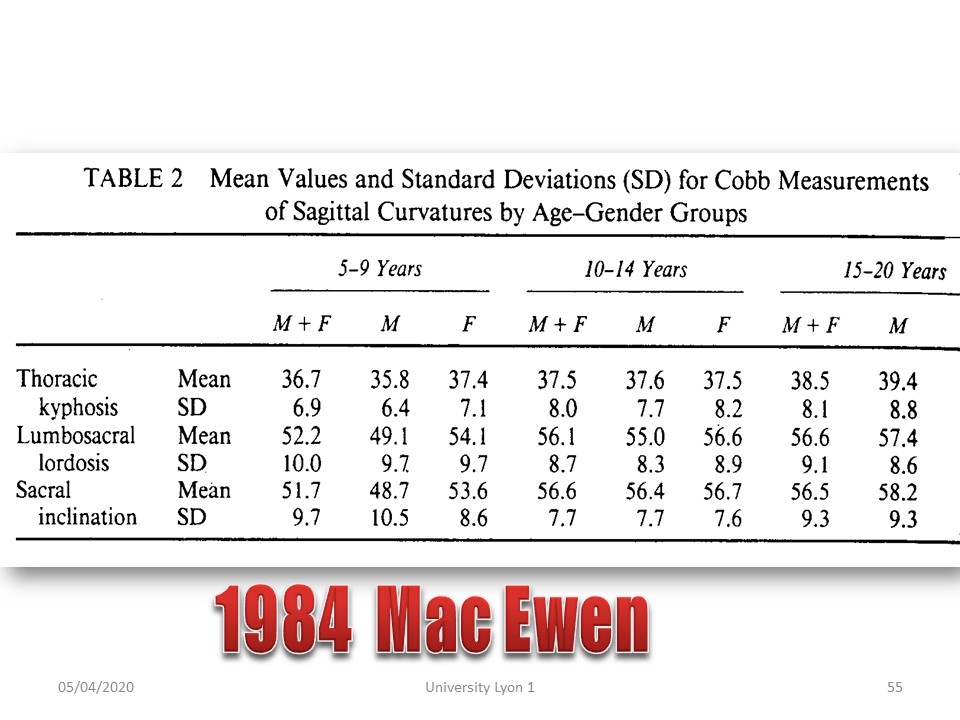 |
We find the same angulation of kyphosis measured in T4 and an average lordosis of 55 ° (number which is part of the Fibonacci sequence). It is therefore around the age of 5 that homo sapiens acquires its definitive morphostatic, which leaves possibilities of modeling to conservative orthopedic treatment. |
 |
Achieving sagittal isostatic balance is fundamental in the correction of scoliosis. It is only recently that profile radiographs have been performed systematically. The plastered sections of the past are no longer necessary with modern technologies allowing simultaneous correction of both planes. |
 |
Achieving sagittal isostatic balance is fundamental in the correction of scoliosis. It is only recently that profile radiographs have been performed systematically. The plastered sections of the past are no longer necessary with modern technologies allowing simultaneous correction of both planes. |
 |
We are now going to study the clinical patterns of the different kyphosis. |
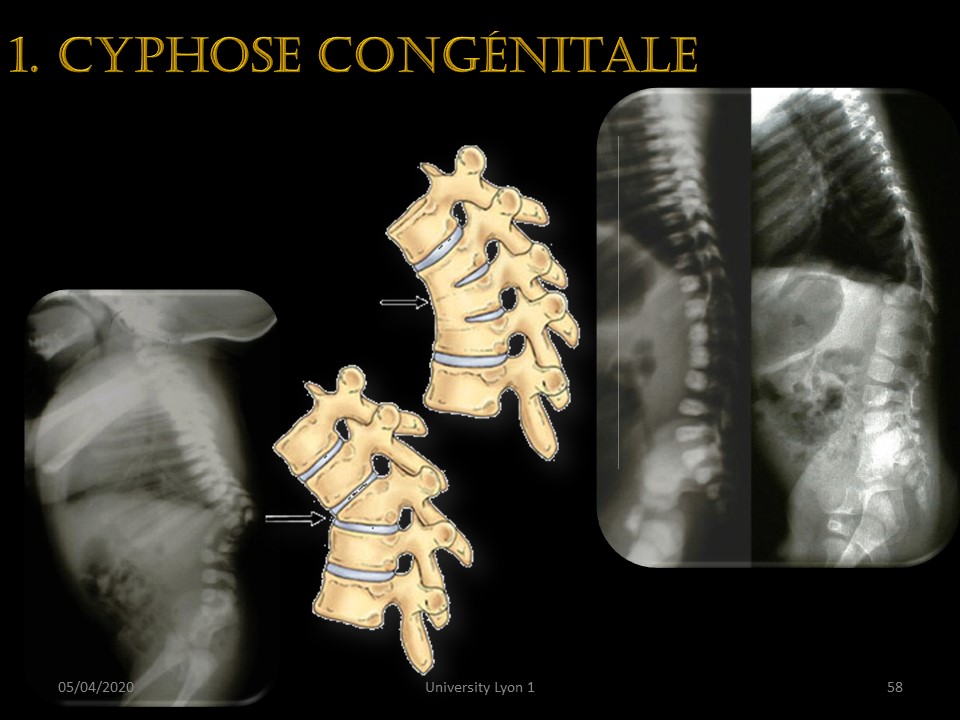 |
In infants, the existence of a kyphosis, most often angular, is a congenital vertebral malformation that can be either an anterior block or a corporeal agenesis. |
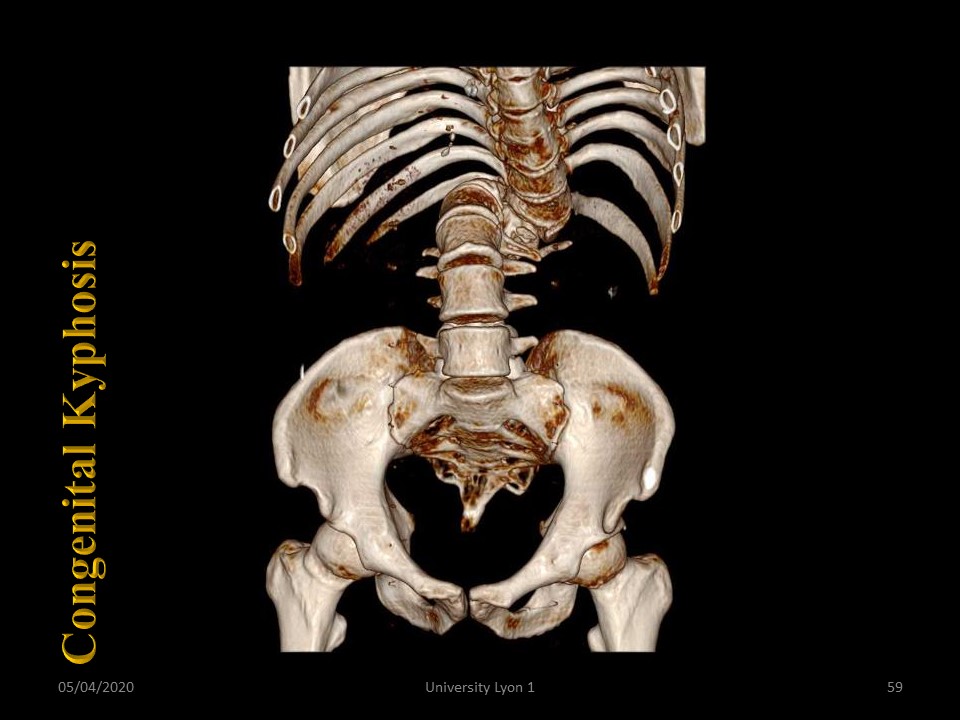 |
Here we see the so-called bayonet evolution of a congenital malformation at the thoraco-lumbar junction. The tri-dimensional representation is obtained by a bar scanner, because in this case, EOS does not work. |
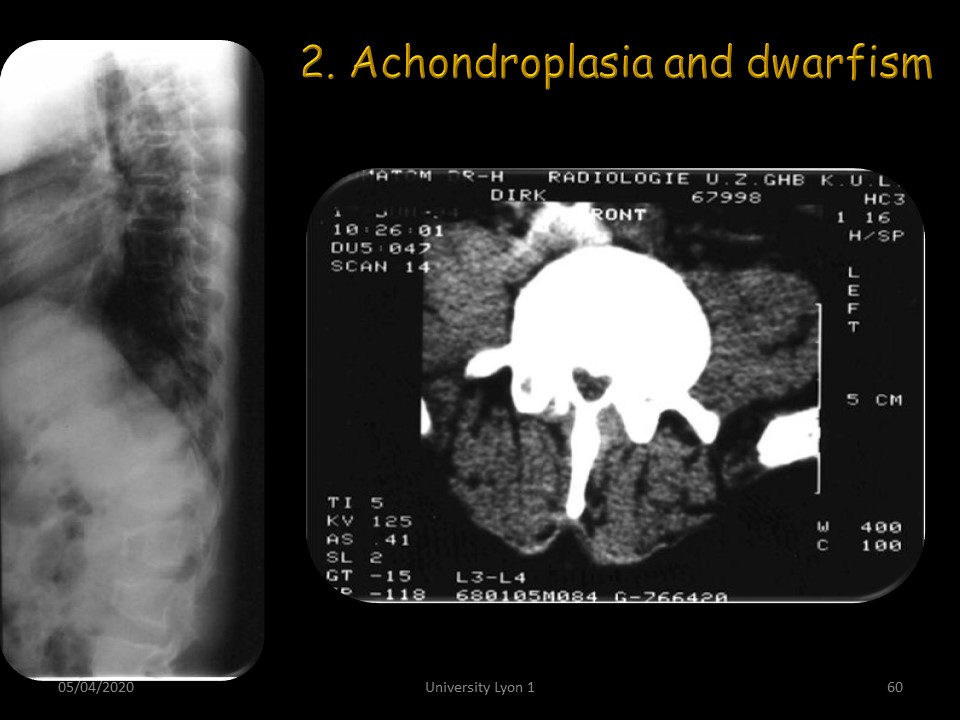 |
Dwarfism, including achondroplasia, often presents thoraco-lumbar kyphosis with a spinal stenosis. |
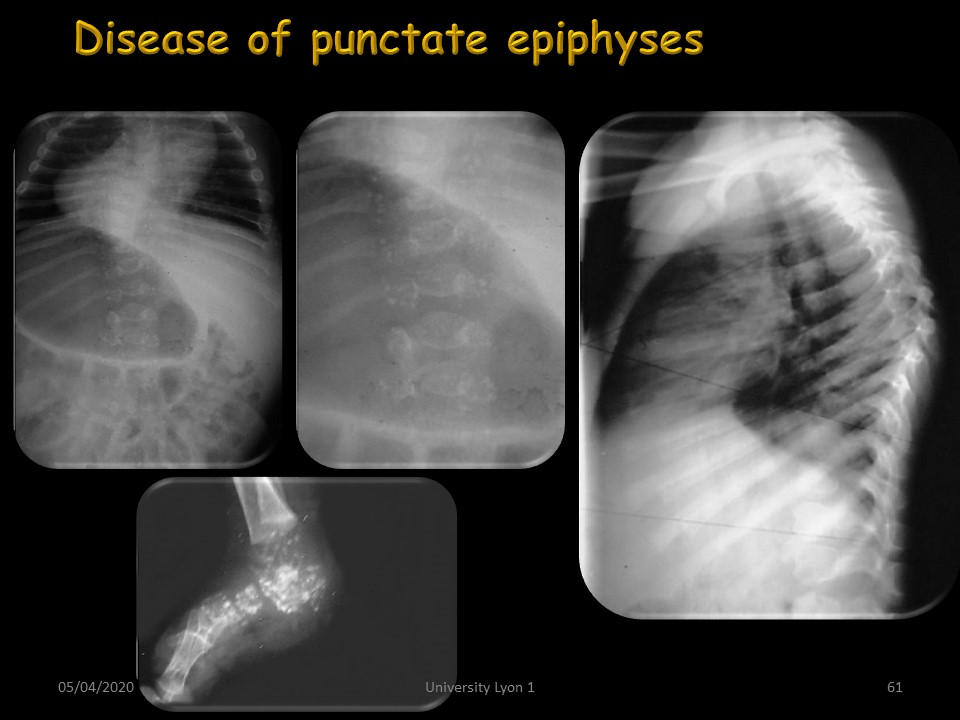 |
In the same way as other chondrodystrophies such as punctate epiphysis disease, which are seen very transiently on X-rays. |
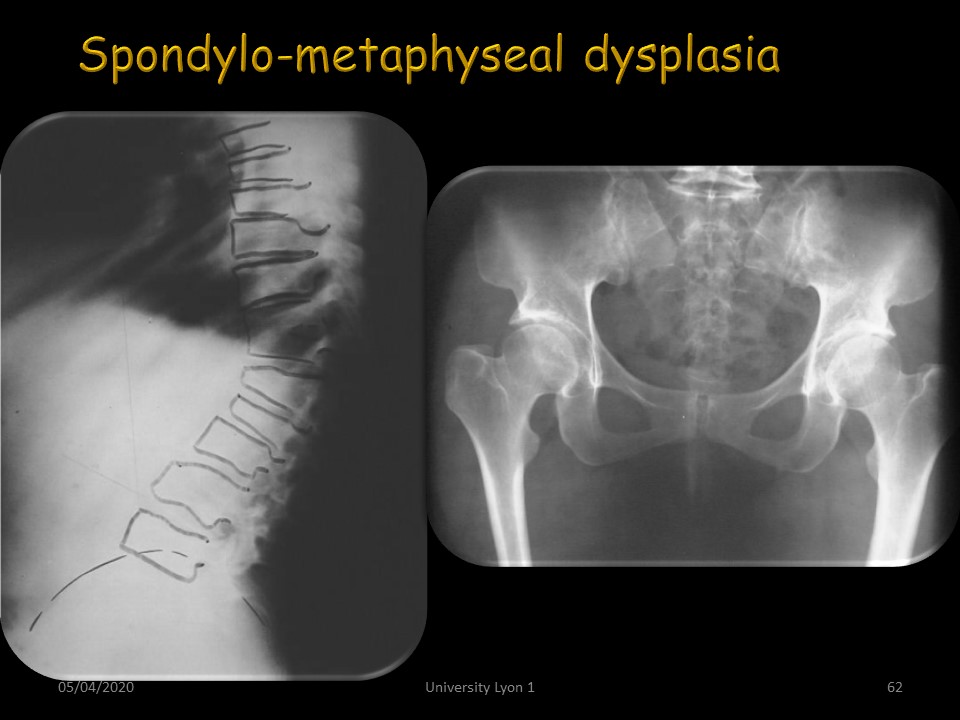 |
The dysplasias can be spondylo-epiphyseal or spondylo-metaphyseal, as in this patient with a strong thoraco-lumbar kyphosis. |
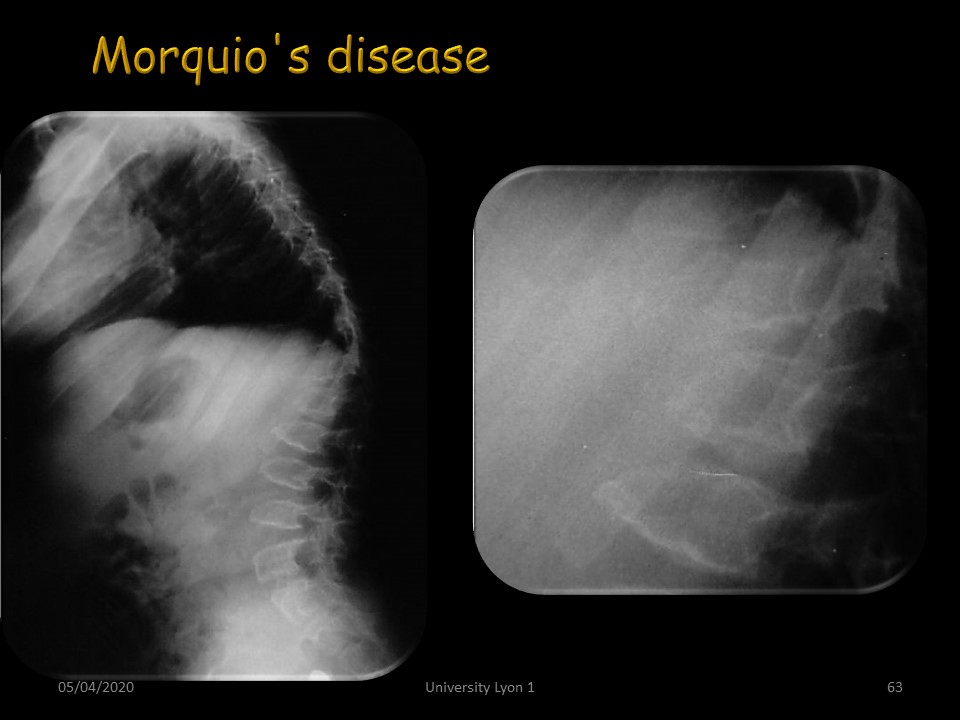 |
The same is true for metabolic dysplasias such as Morquio's disease.x |
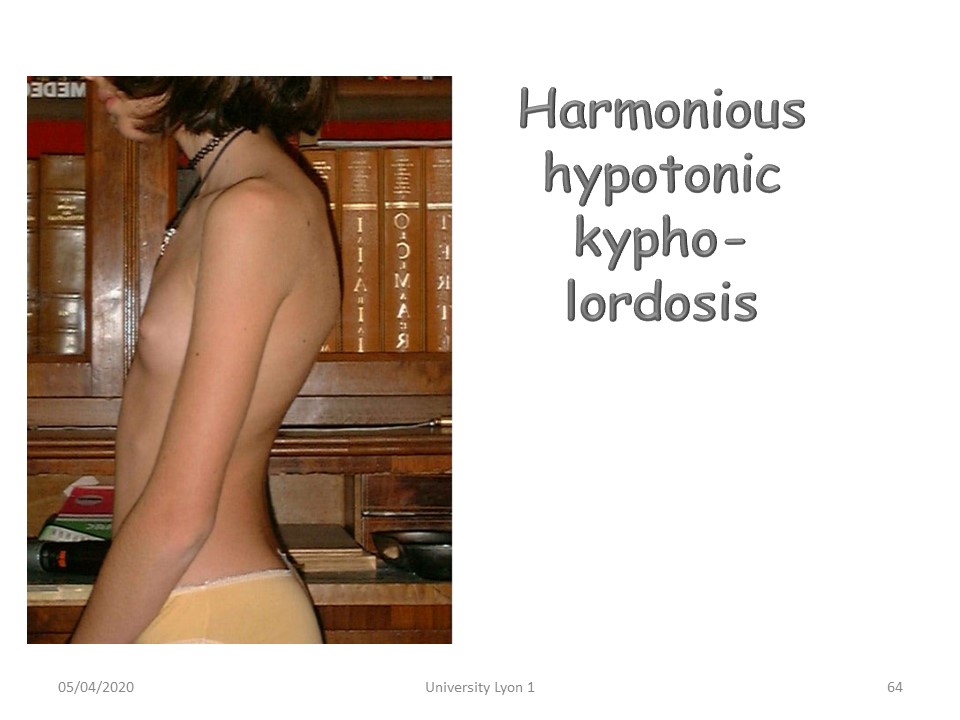 |
Harmonious hypotonic kypho-lordosis. |
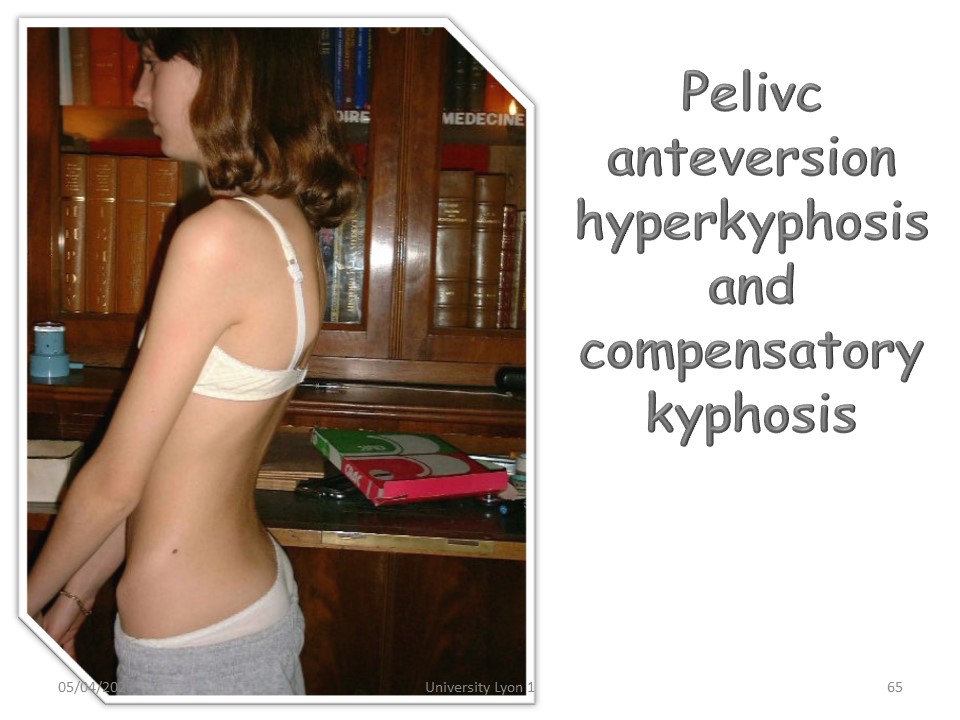 |
Hyperlordosis by pelvic anteversion and compensatory kyphosis. Kyphosis is sometimes the rebalancing consequence of underlying hyperlordosis. |
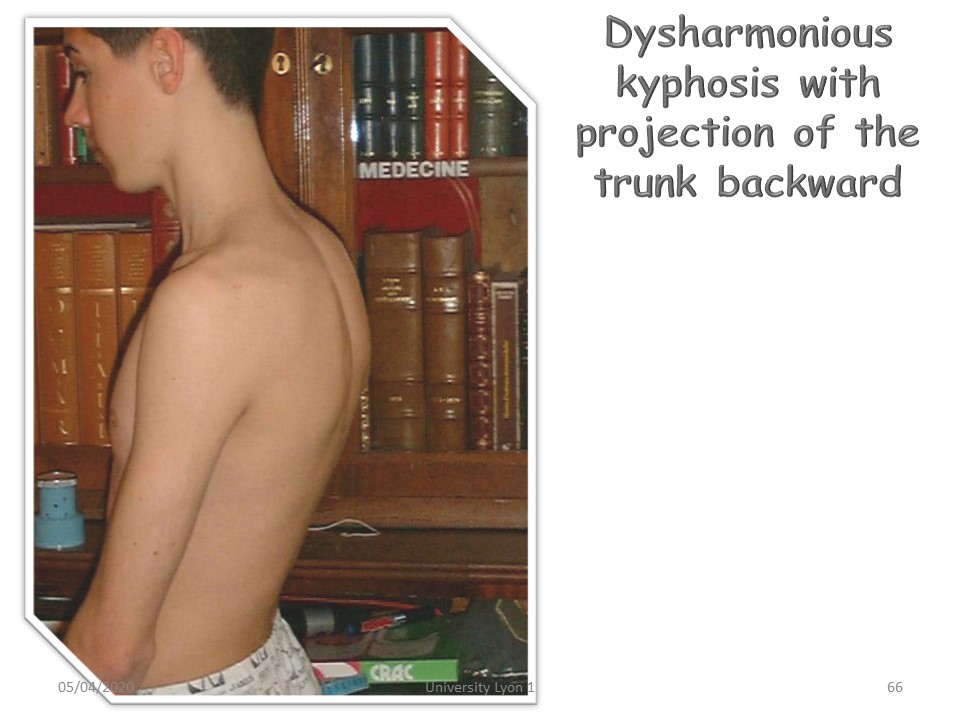 |
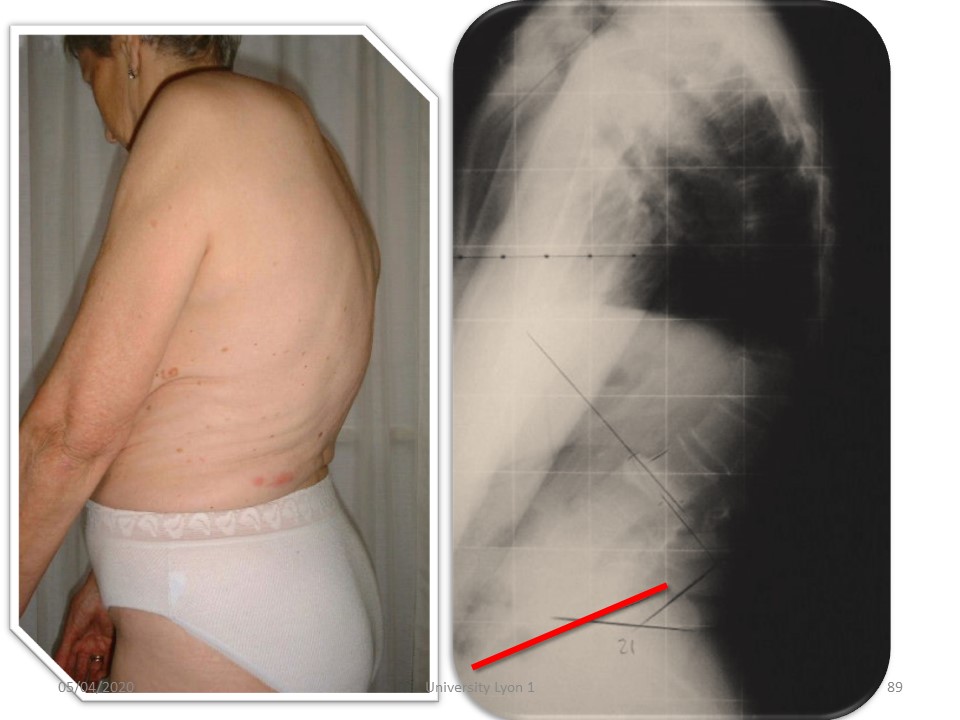
Kyphosis with backward projection of the trunk. The sagittal offset is increased. |
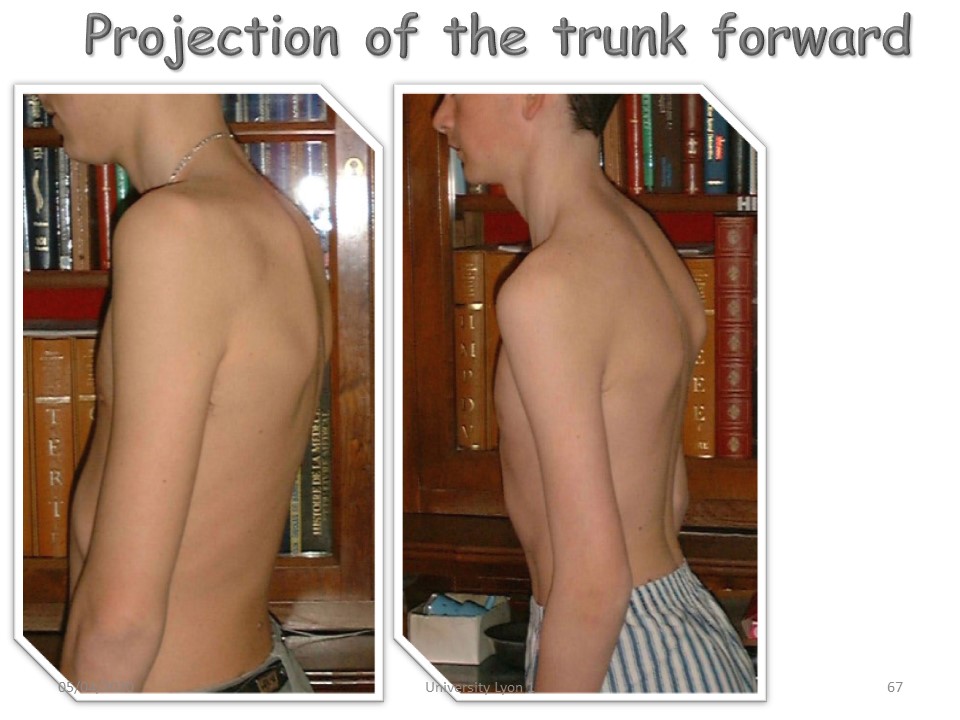 |
Kyphosis with forward projection of the trunk, the sagittal offset is diminished or inverted. |
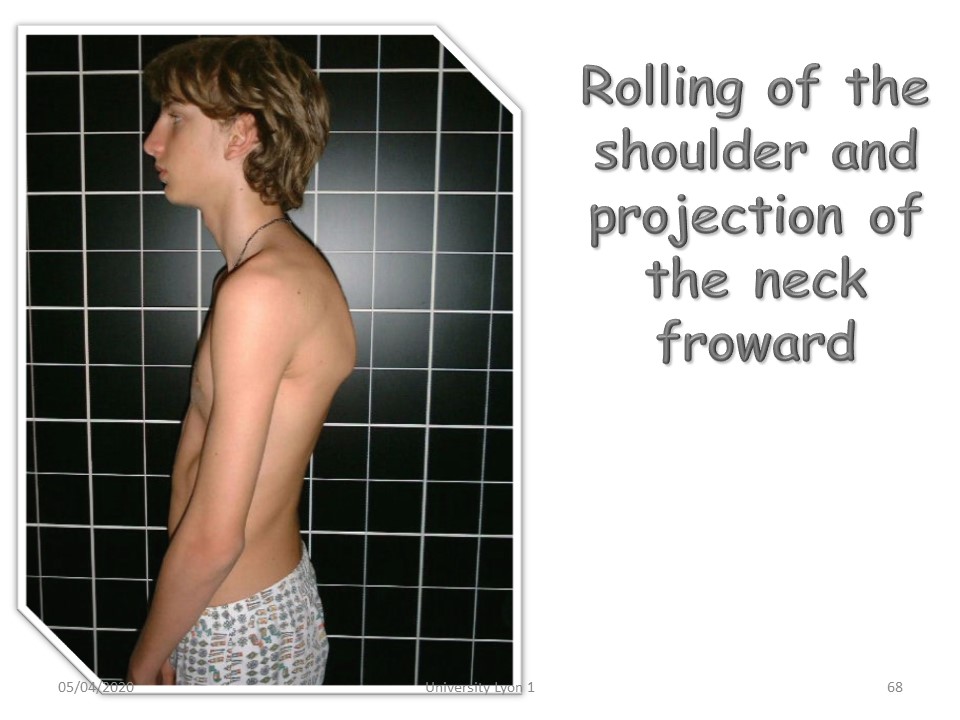 |
Kyphosis and forward shoulder wrap. |
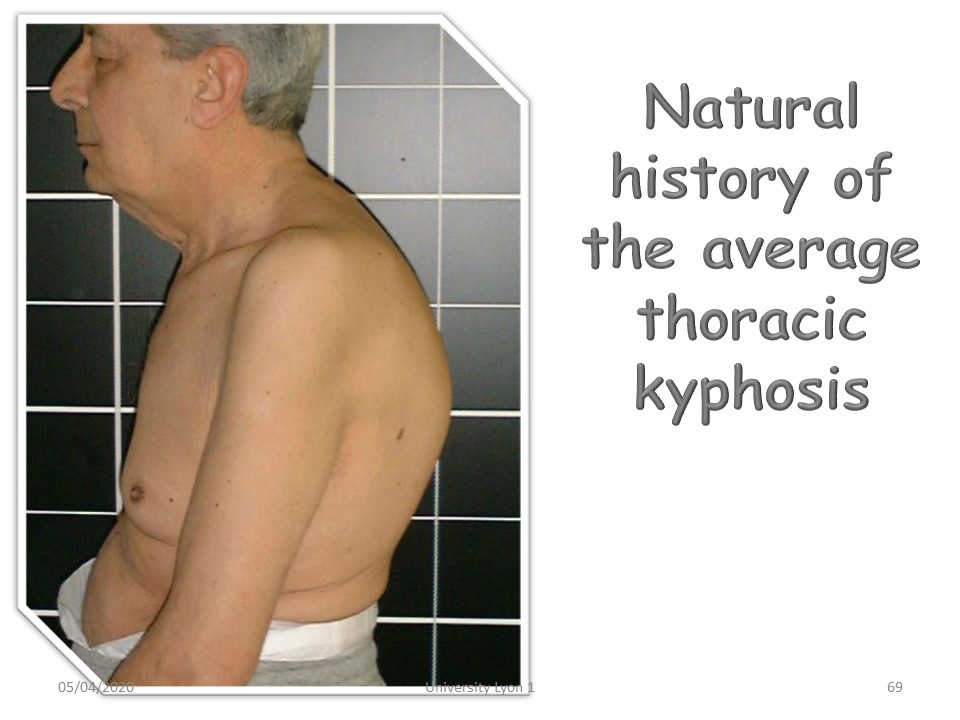 |
Natural history of middle thoracic kyphosis. |
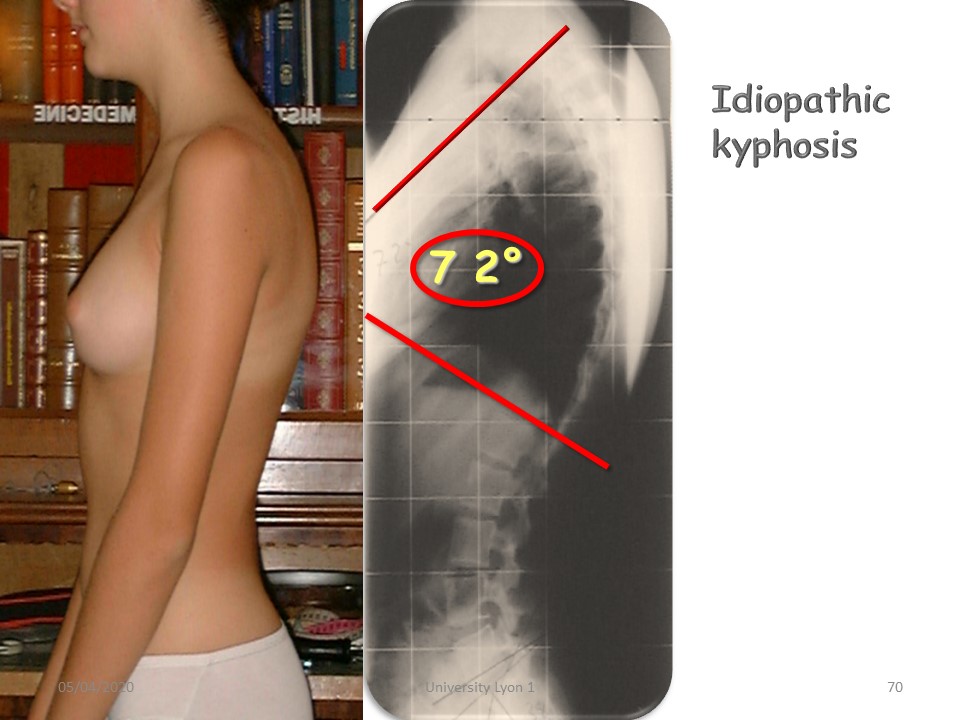 |
Idiopathic Hyperkyphosis. |
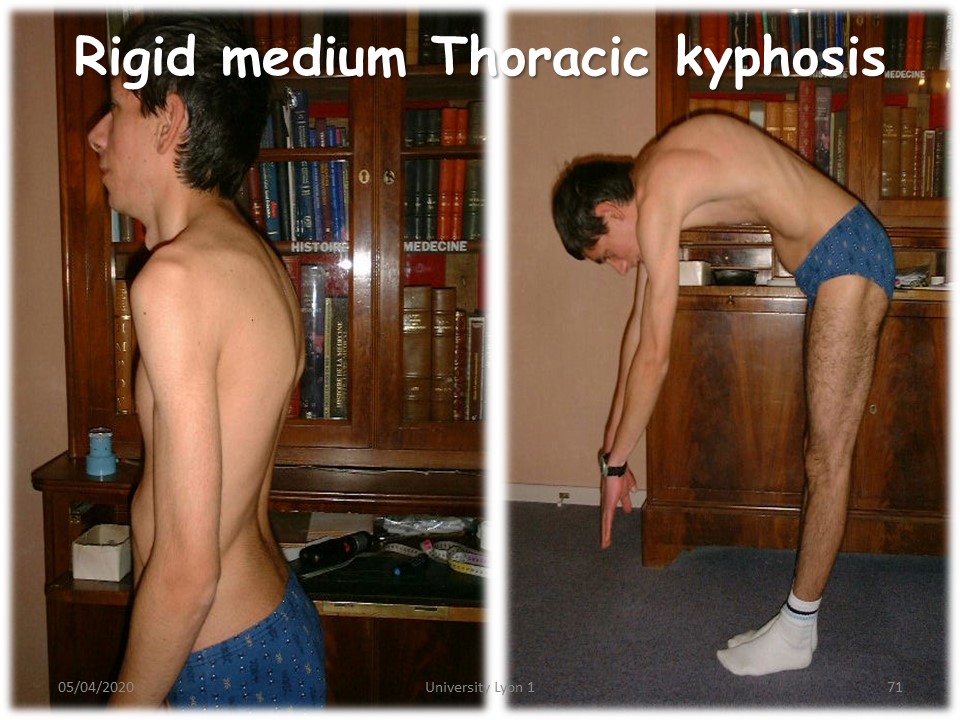 |
Rigid middle thoracic kyphosis. Combination of direct and indirect stiffness. |
 |
|
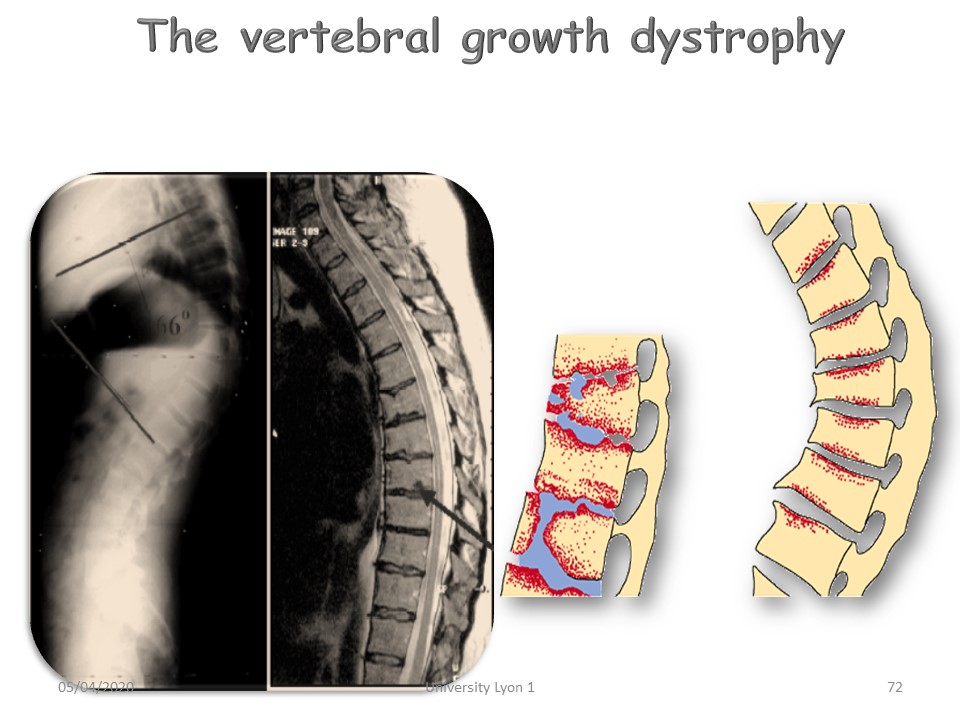 |
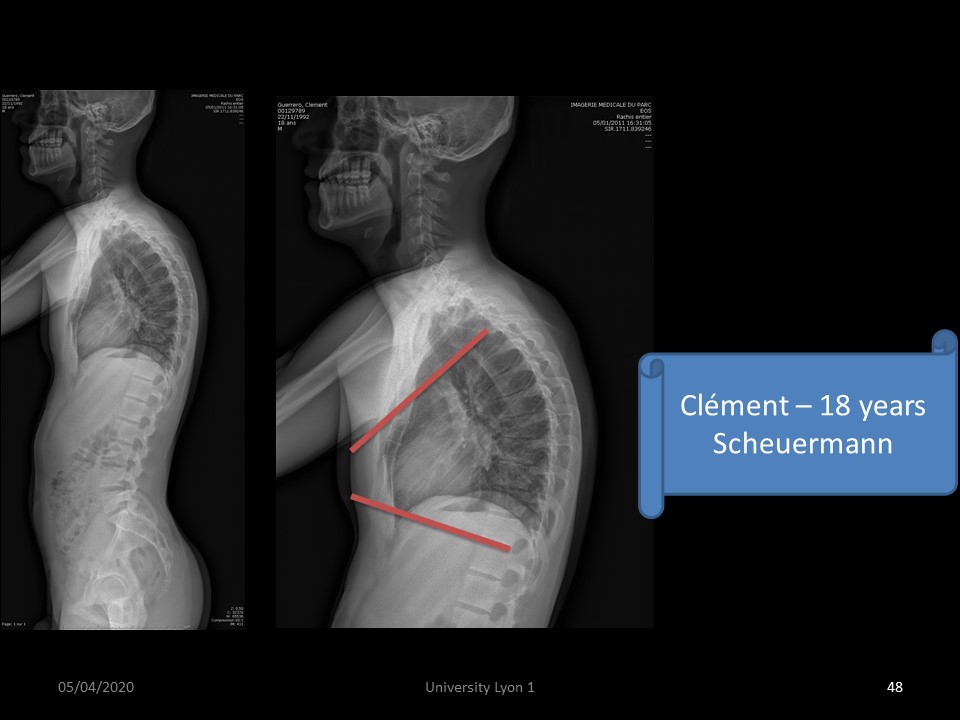
Spinal growth dystrophy or Scheuermann's disease is one of the most common causes of thoracic or thoracolumbar hyperkyphosis. The first stage is the irregularity of the cartilage plates. |
 |
It has been described by an orthopedic surgeon and Danish radiologist on apprentice watchmakers. |
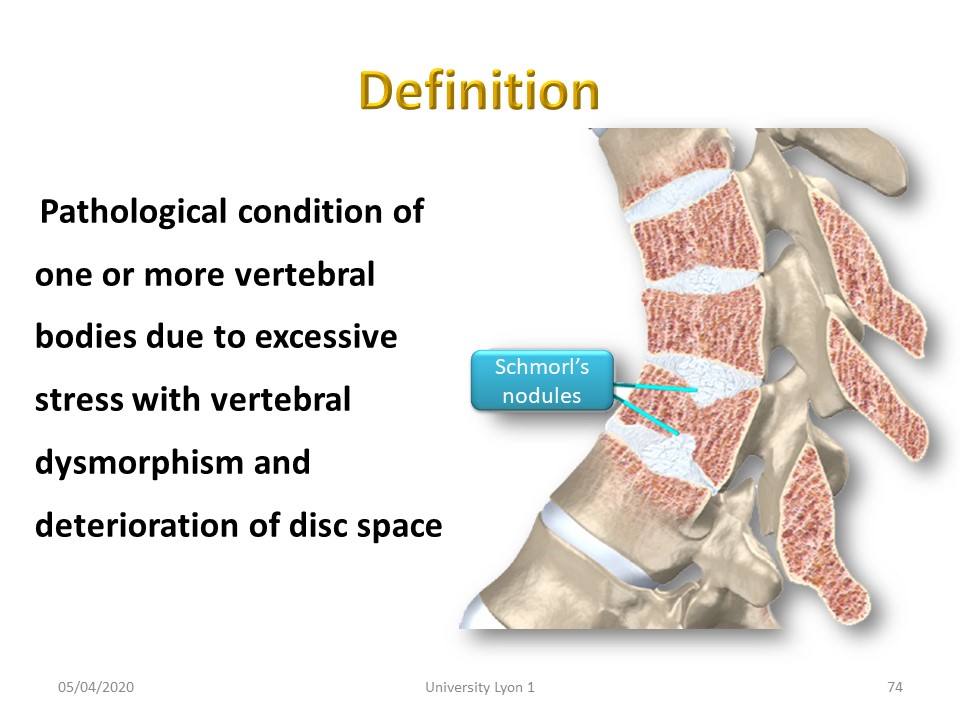 |
The disease concerns one or more vertebral bodies with mechanical deformity (cuneiformization) of the vertebral bodies. The height of the intervertebral disc is frequently decreased. The notion of repeated micro-traumas is frequently found. |
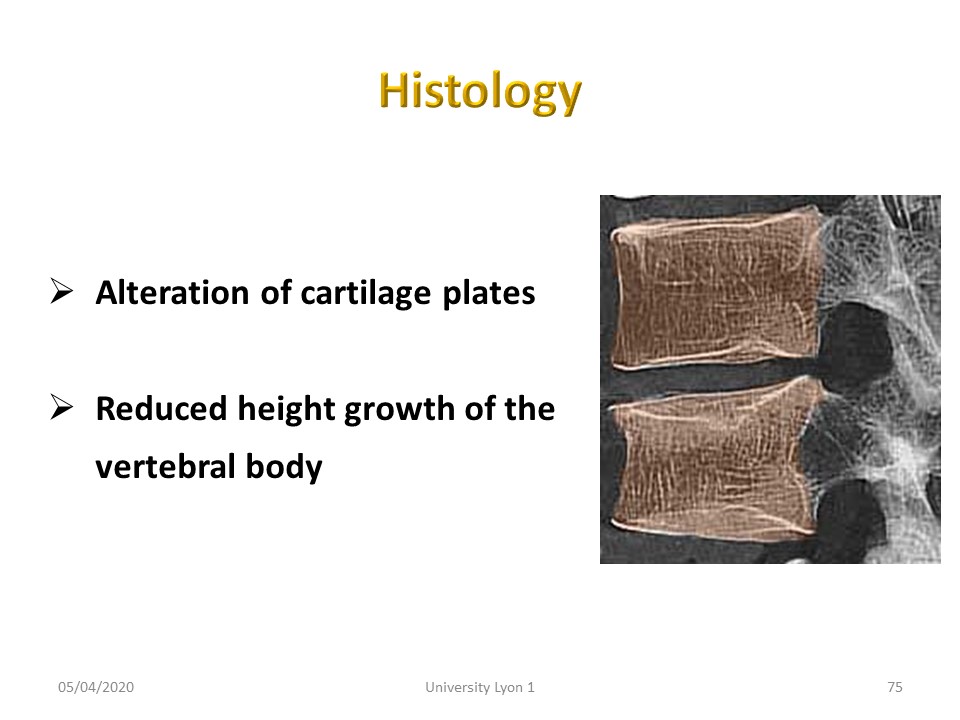 |
Histologically, this is a defect in the growth plate of the vertebral body. |
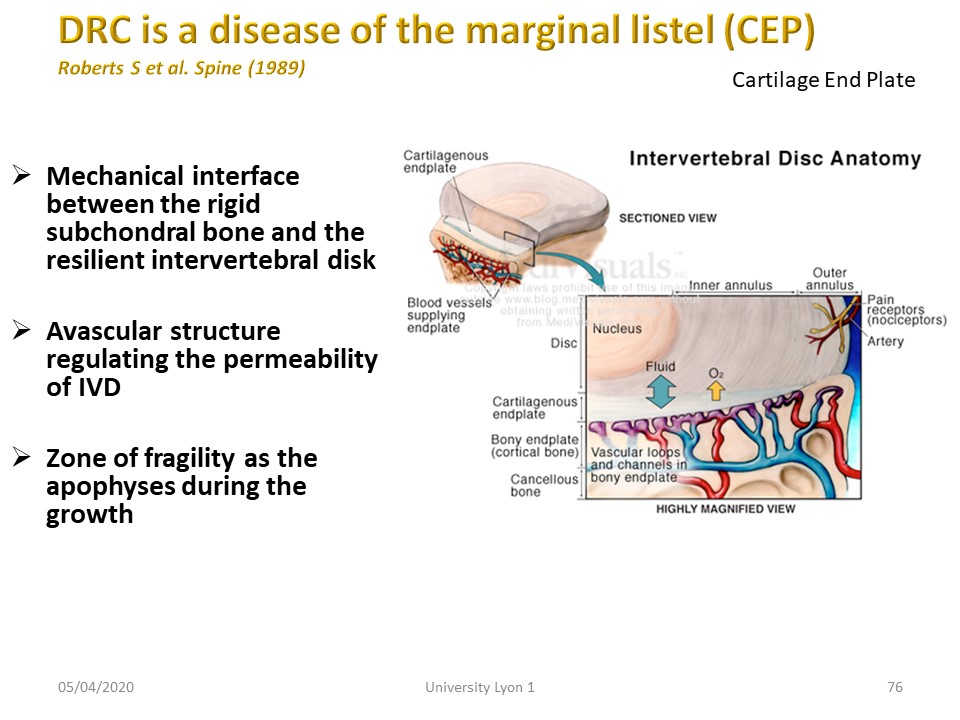 |
The Cartilage End Plate is a mechanical interface between the rigid subchondral bone and the resilient intervertebral disk. The structure is avascular regulating the permeability of IVD. It is a zone of fragility as the apophyses during the growth. |
 |
The Scheuermann's disease, often familial, weakens the vertebral body. In sport, microtrauma associates with fragility to cause deformations of the vertebral body. |
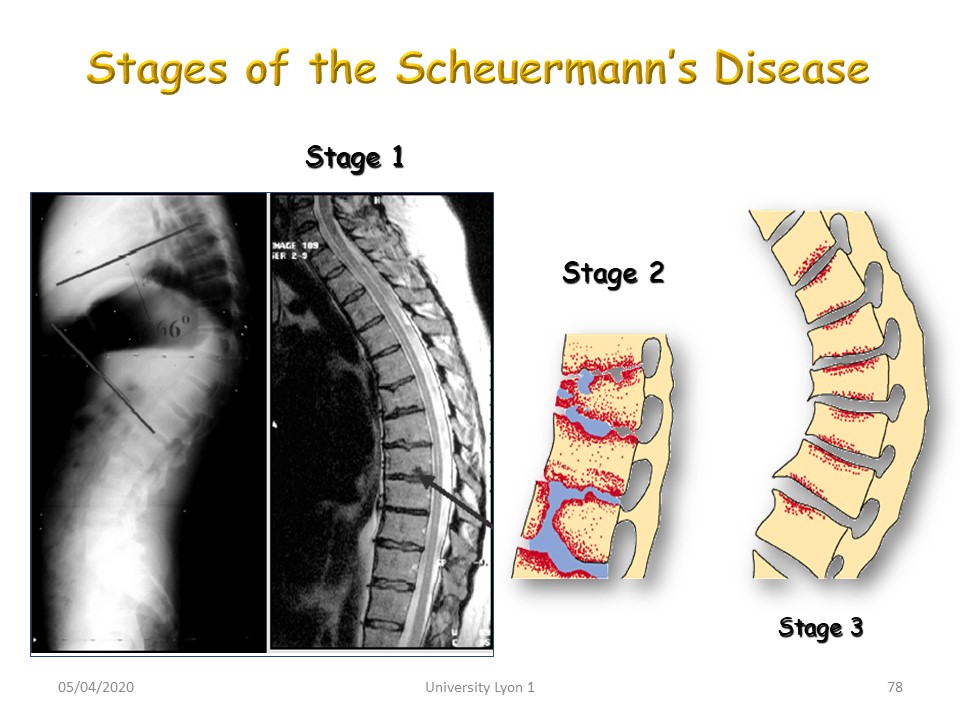 |
There are 3 stages: Stage 1. with irregular cartilaginous plates. Stage 2. with cuneiformization of the vertebral body, but respect of the posterior wall and stage 3. with collapse of the entire vertebral body. |
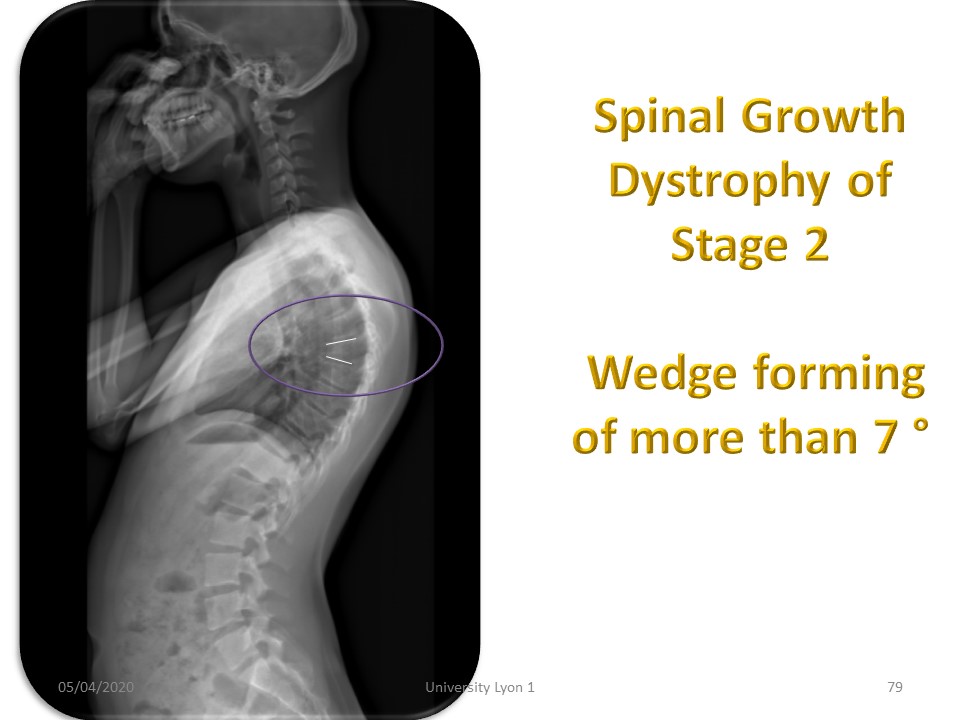 |
Scheuermann stage 2 in this patient with wedging of more than 7° of the vertebral body (physiological limit). |
 |
Spinal Growth Dystrophy stage 3, with significant and diffuse alteration on several vertebral bodies. The anterior wall is very dystrophic. |
 |
MRI is often much more impaired than simple radiography. At this stage, there is frequently a flattening of the vertebral bodies or platyspondyly. |
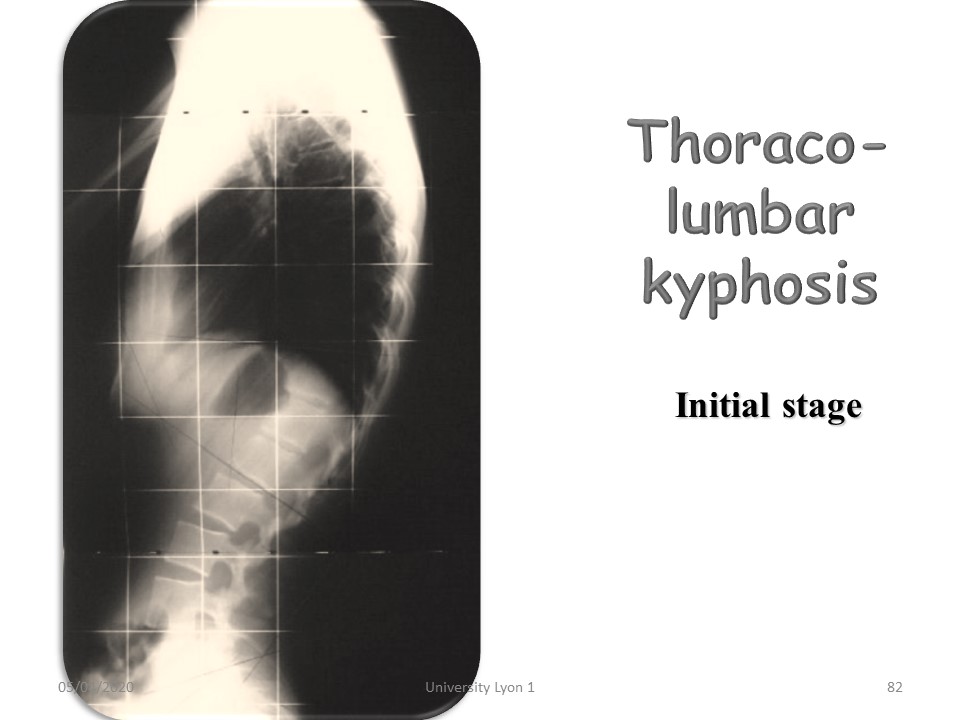 |
Early stage thoracolumbar kyphosis. |
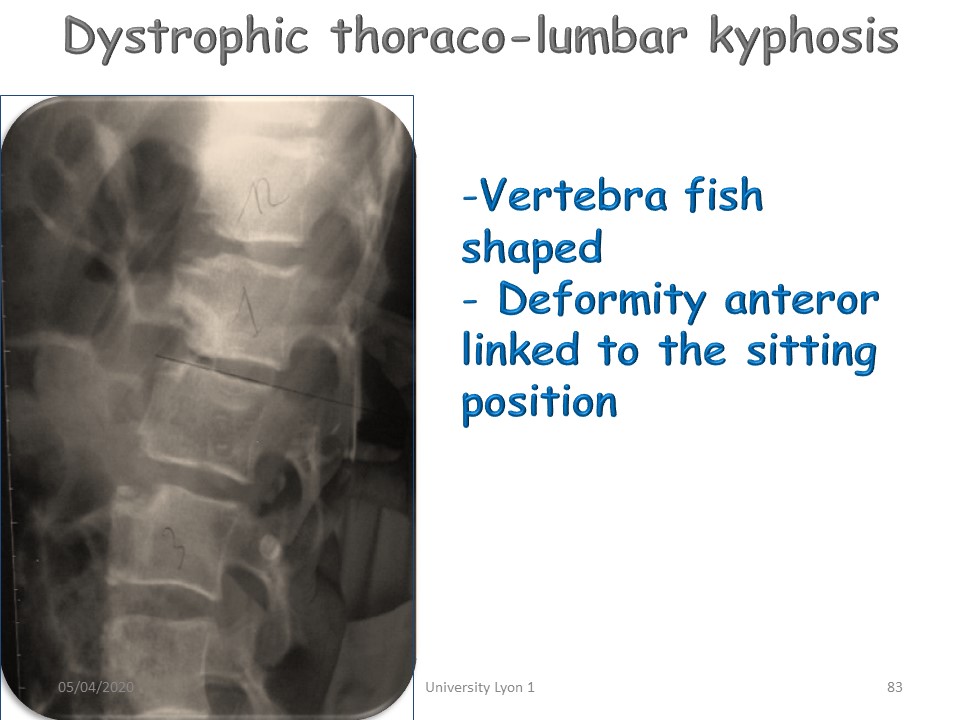 |
Dystrophic, fish-like vertebra, common in the thoracolumbar region. The remaining epiphysis remains visible and in principle is not altered. |
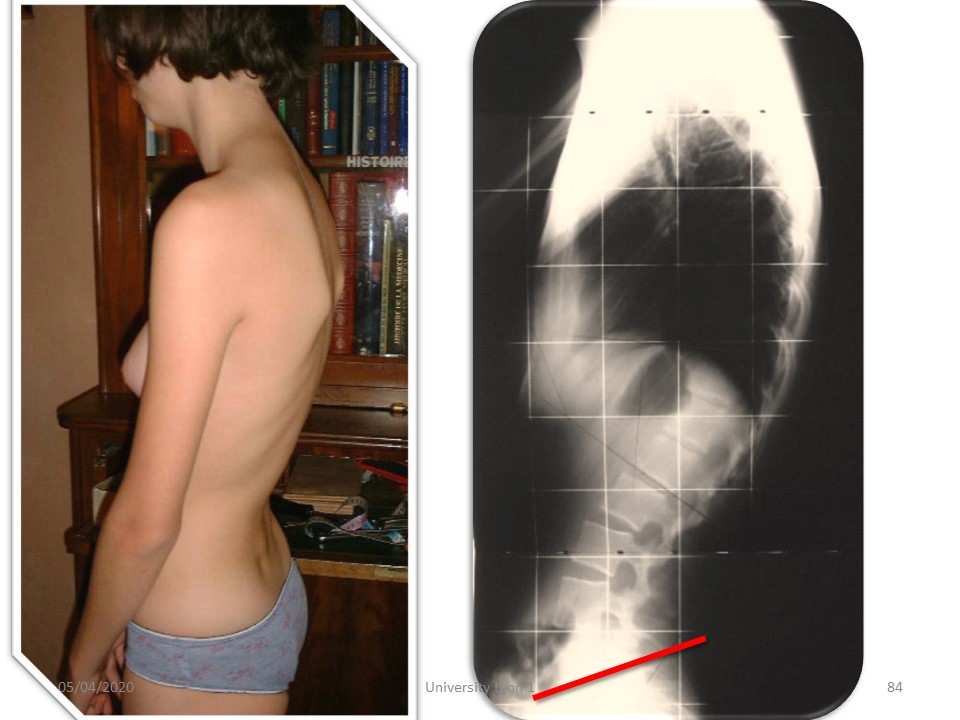 |
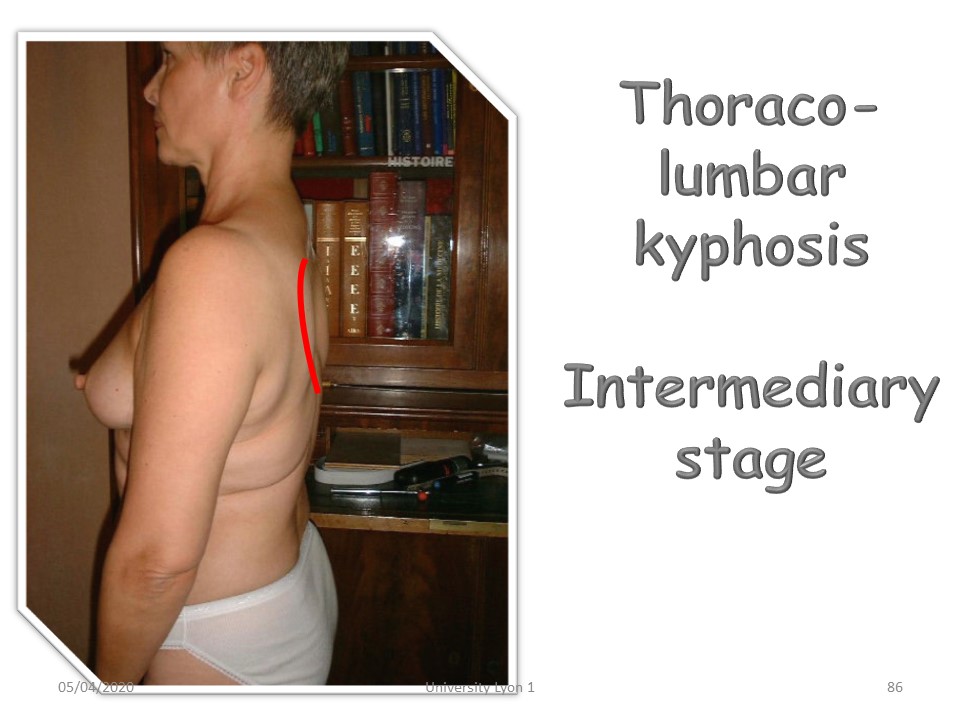
Evolution of thoracolumbar kyphosis during adolescence. |
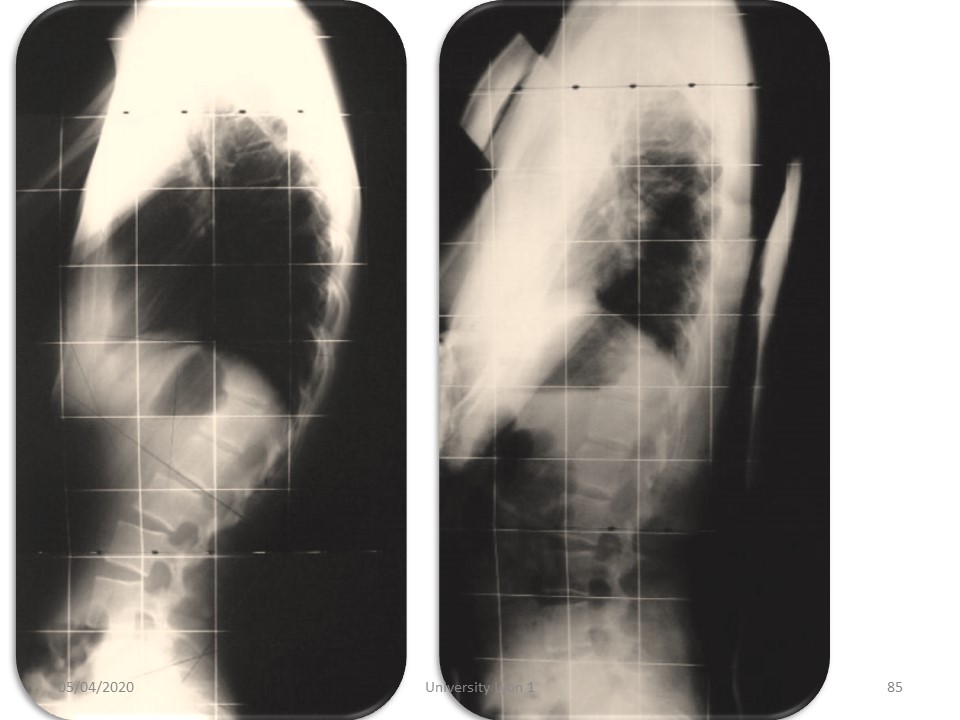 |
The plastered cast corrects this kyphosis and will stretch the anterior longitudinal ligament. |
 |
In adulthood, thoracolumbar kyphosis may be associated with an overlying thoracic flat back causing vertebral inversion. |
 |
Here we note the beginning of L2-L3 sagittal dislocation with retrolisthesis. |
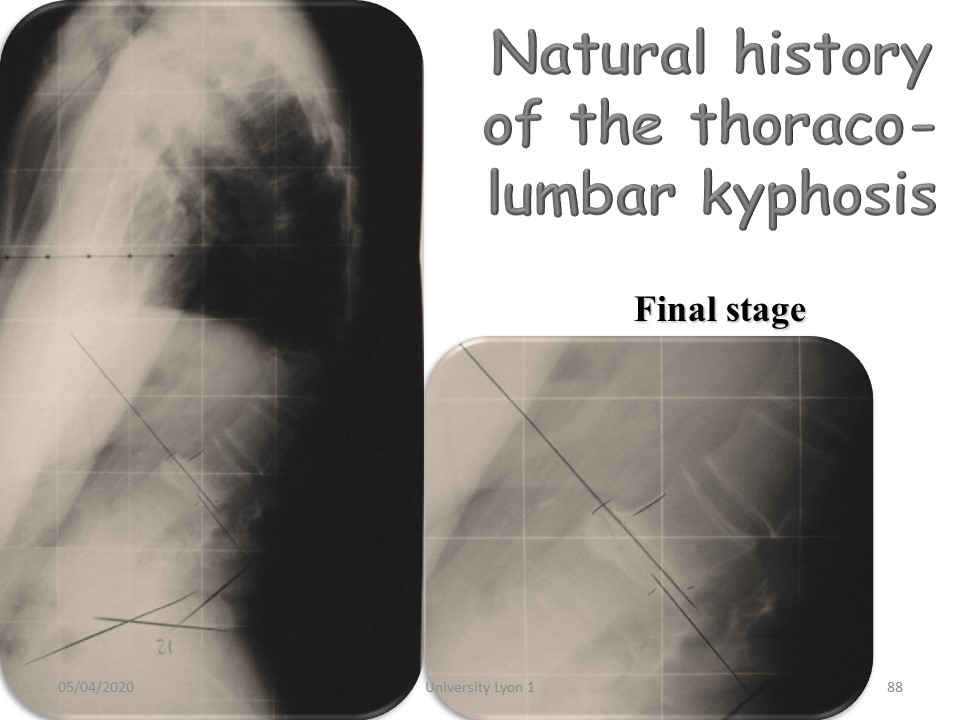 |
In the final stage: Retrolisthesis L2-L3 spontaneously stabilized by performing a kind of arthrodesis. |
 |
The evolution can still continue with pelvic retroversion and horizontalization of the sacral slope. |
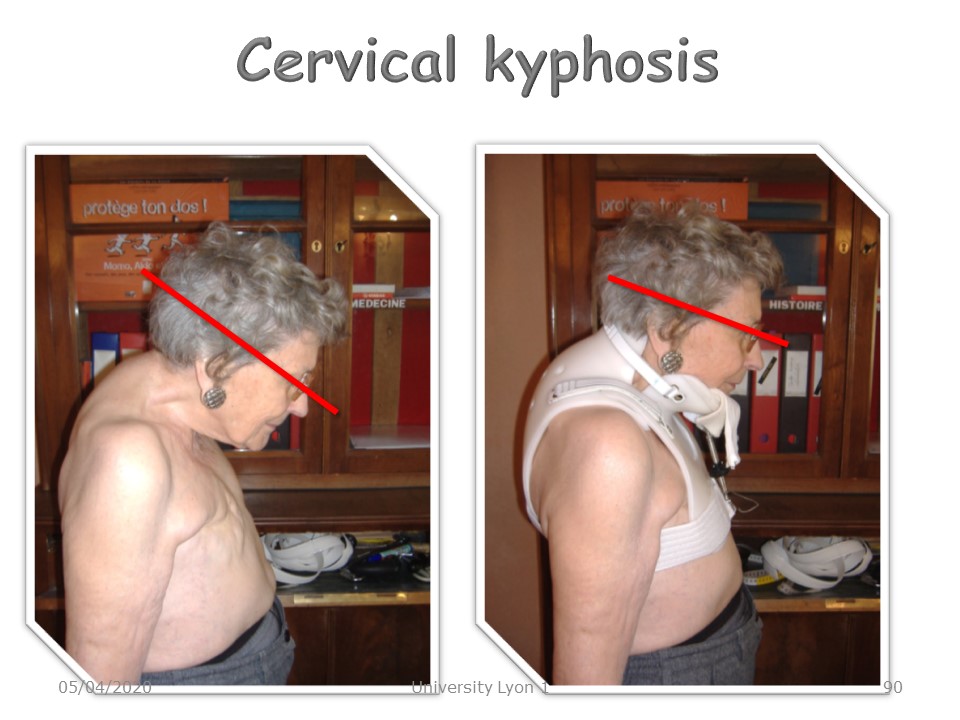 |
Upper cervical kyphosis is a particular clinical pattern with a major postural consequence, as the horizontal semicircular canals are no longer horizontal. |
 |
|
 |
Non-surgical conservative orthopaedic treatment of kyphosis has benefited, as in the case of scoliosis, from the contribution of new technologies. Considerable progress has been made since the time when malformed newborns were abandoned on the slopes of Mount Taygete in ancient Greece. |
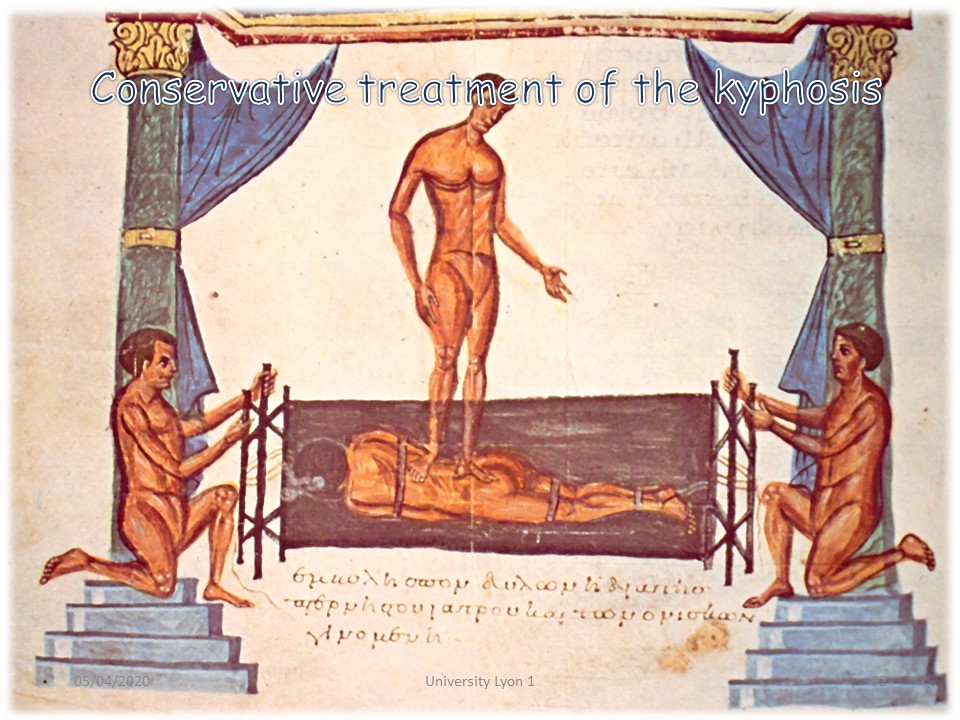 |
In Hippocrates' time, the reduction technique already included a translation along the longitudinal axis of the spine and a 3-point system in a transverse horizontal plane. |
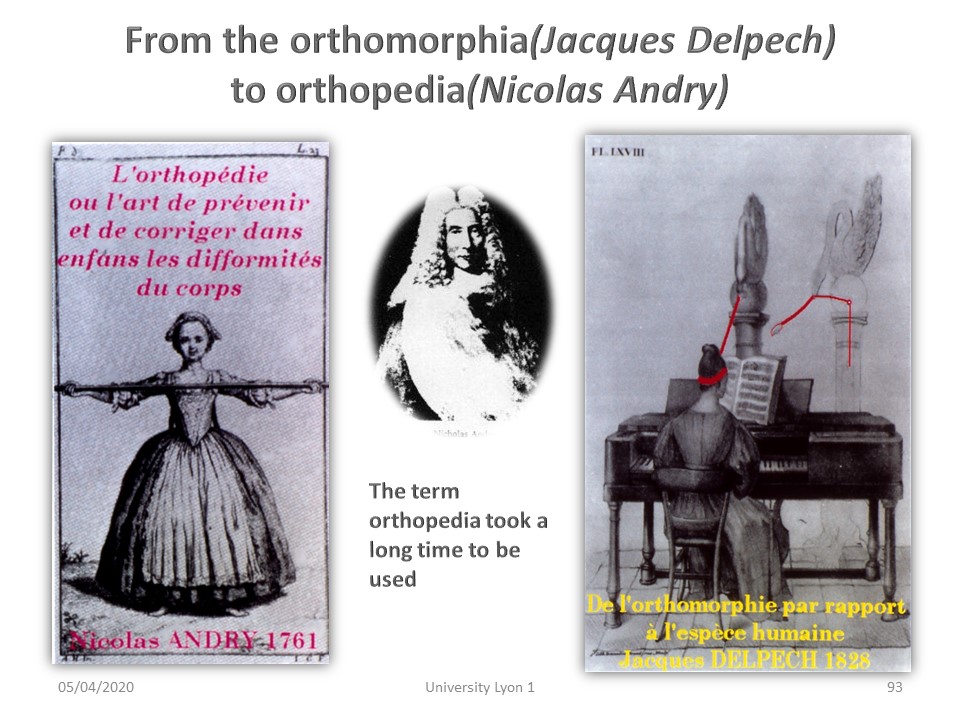 |
But orthopaedics really began in the middle of the 18th century with Nicolas Andry. |
 |
In the 19th century, the first orthopaedic treatment centres appeared where mechanical means were concentrated, such as the Pravaz Institute in Lyon. |
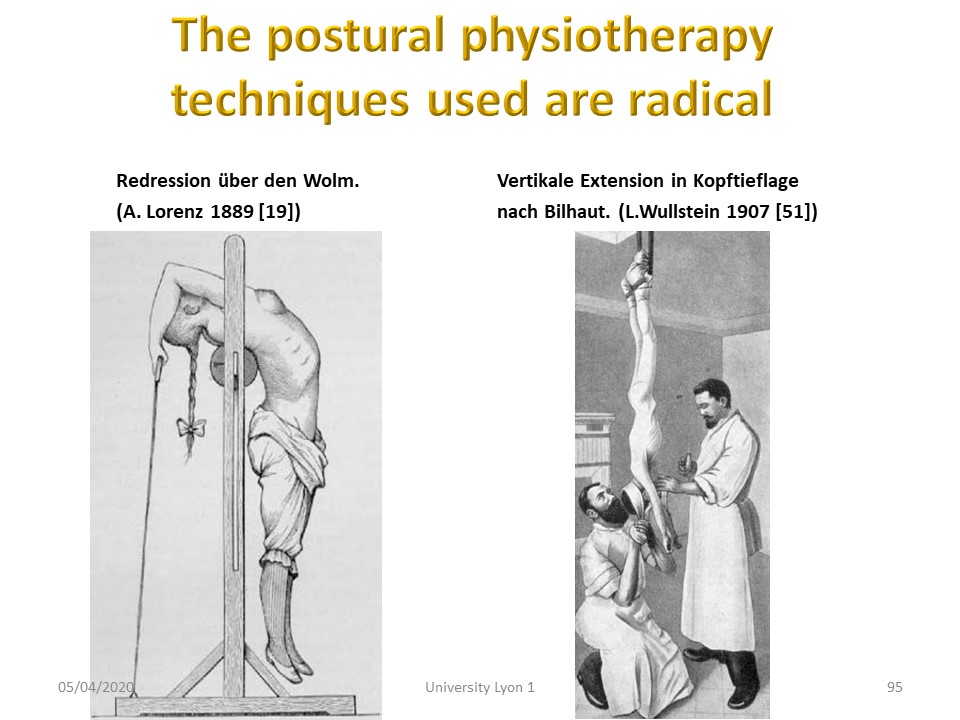 |
Postural physiotherapy techniques used in Germany are based on hyperextension and vertebral inversion. |
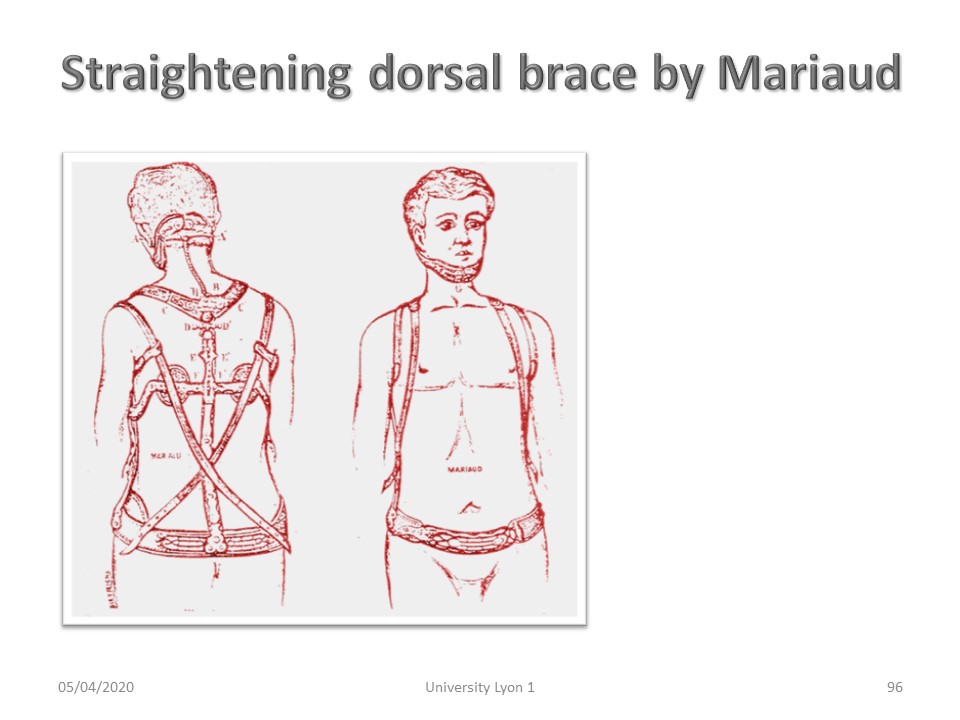 |
Back straightening systems appear in catalogues. |
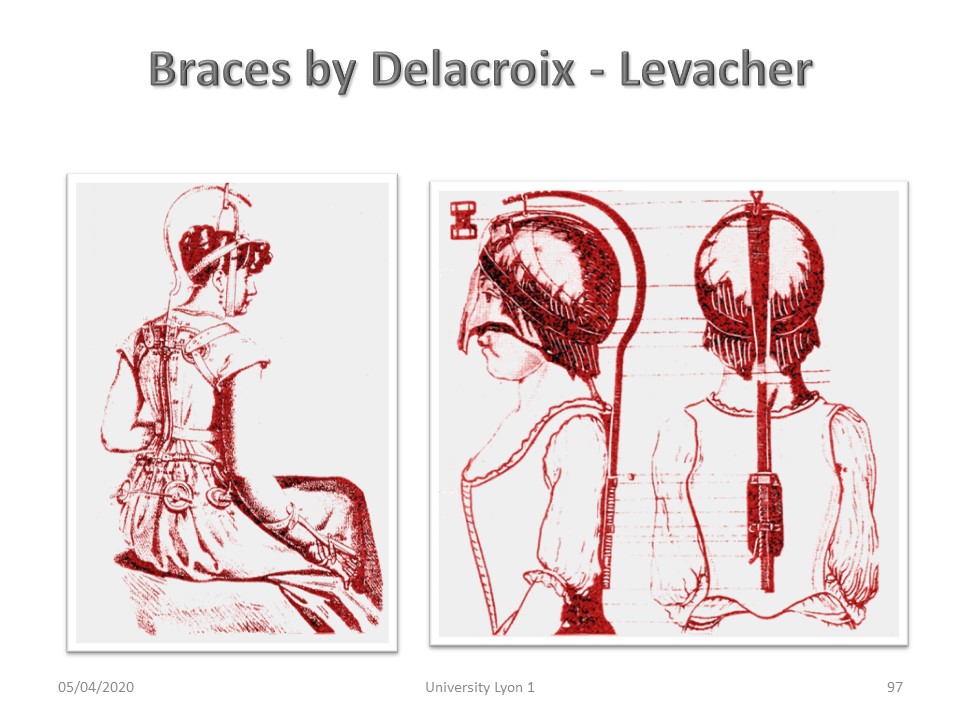 |
The correction by traction along the vertebral longitudinal axis is performed here by means of a helmet. |
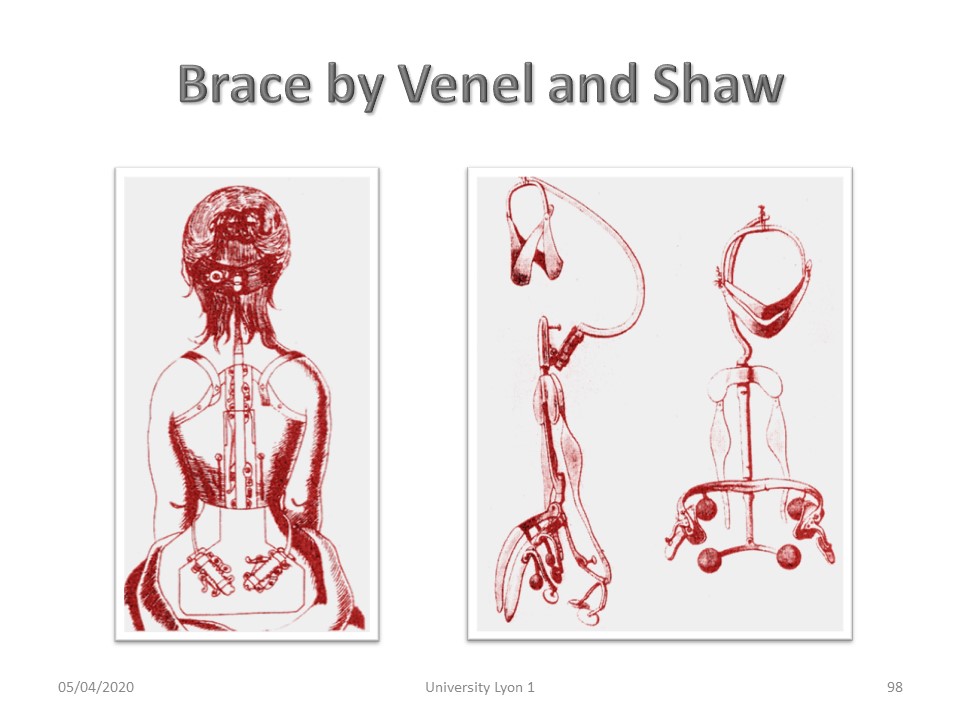 |
The helmet will soon be replaced by an adjustable chin strap. |
 |
Immediate physiotherapy in plaster cast follows the same progression as scoliosis: 1. Control of breathing. The vital capacity is often limited by more than 20%. 2. Mobilization at pelvic and scapular areas. 3. Active axial elongation. 4. Learning compensations in the gestures of everyday life. |
 |
The second phase of physiotherapy aims to stimulate the reticulo-spinal system to prevent atrophy of the deep musculature. All usual balance exercises can be used. |
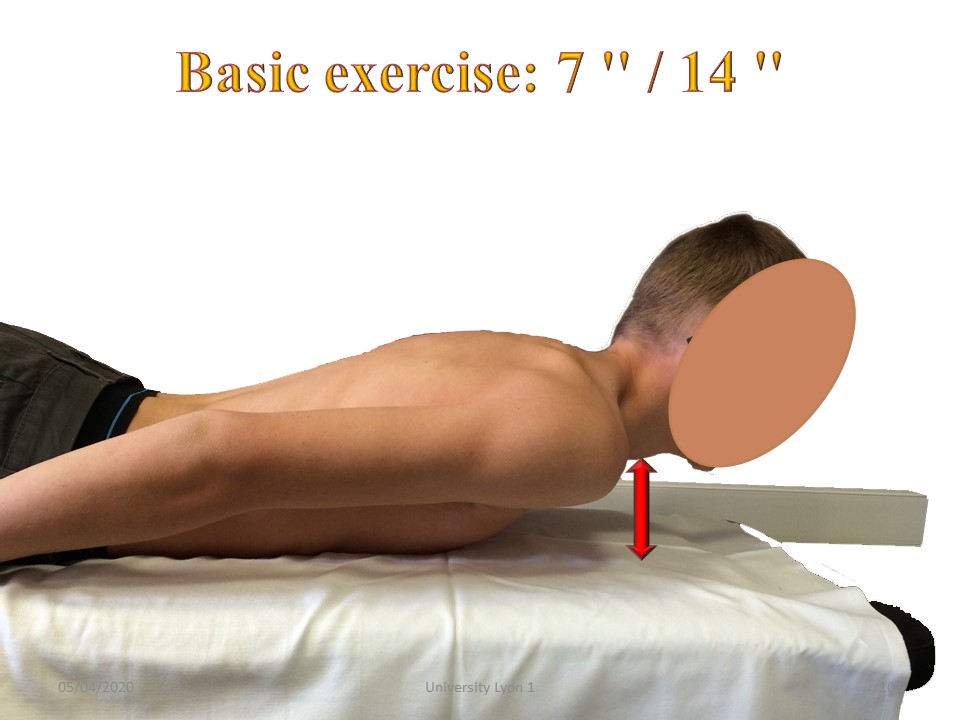 |
Once the plaster has been removed, the basic exercise takes place in procubitus, the arms along the trunk. The child lift the chin and maintains the corrected position for 7 seconds, then rests for 14 seconds. |
 |
The soft corrective postural back brace can be useful when kyphosis is flexible and in addition to physiotherapy. They have the disadvantage of being passive whereas one wishes on the contrary to stimulate the postural mechanisms of self-correction. |
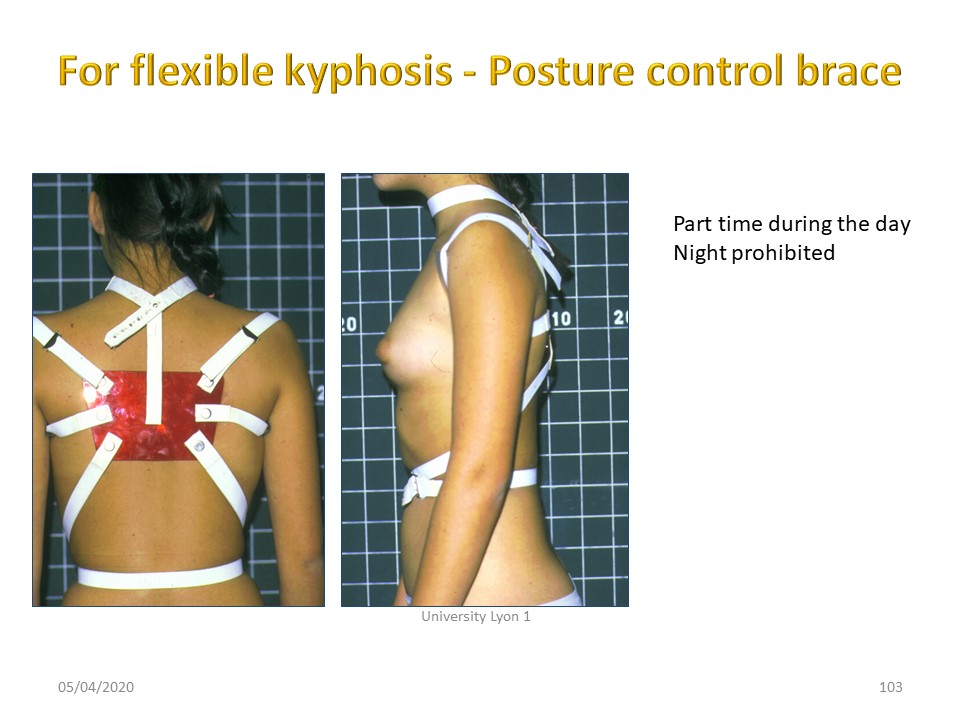 |
A more rigid posture control back brace allows a good stabilization at the base of the rib cage. They facilitate the retropulsion of the shoulders and limit the projection of the neck forward. The use of these orthoses remains limited. |
 |
Lowe's meta-analysis highlights delays in diagnosis due to poor knowledge of Orthopaedic Medicine. When conservative treatments are used, they are not very effective, because often the plastic deformation of the powerful common anterior vertebral ligament, which is the most retracted part of the deep front line, is not realized. |
 |
In 1987, Sachs presented the results of the Milwaukee brace with only 22% worsening compared to initial angulation. |
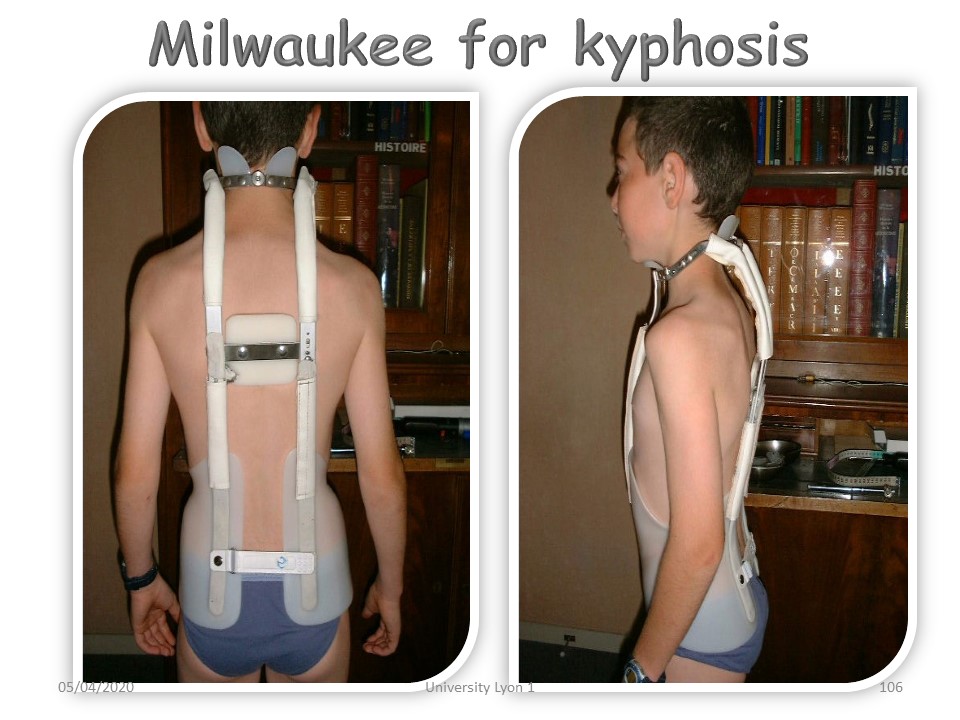 |
The night bracing is very effective before the beginning of pubertal growth. The nocturnal wearing guides the growth during the night, redirects the nucleus of the disc forward and achieves a stretching of the deep front line. |
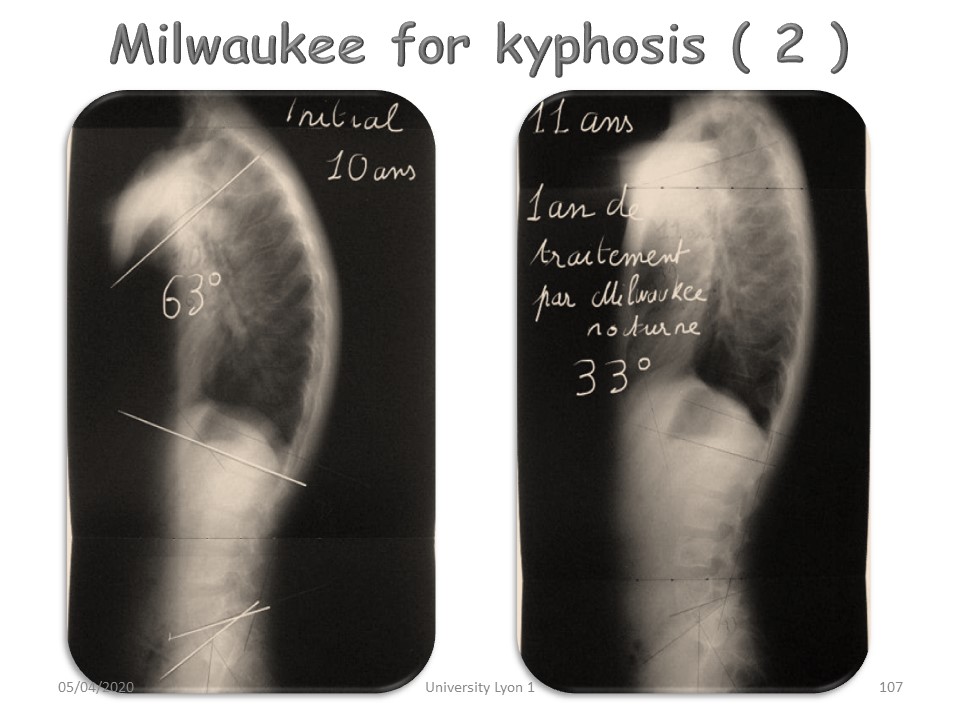 |
Excellent results can be obtained when the curvature is still reducible and with a good compliance. Here complete correction of an idiopathic hyperkyphosis between 10 and 11 years. |
 |
This patient had a congenital vertebral malformation with cervical kyphosis of 48° at the age of 3 years. In the absence of any surgical indication, she was entrusted to us for the realization of a brace. |
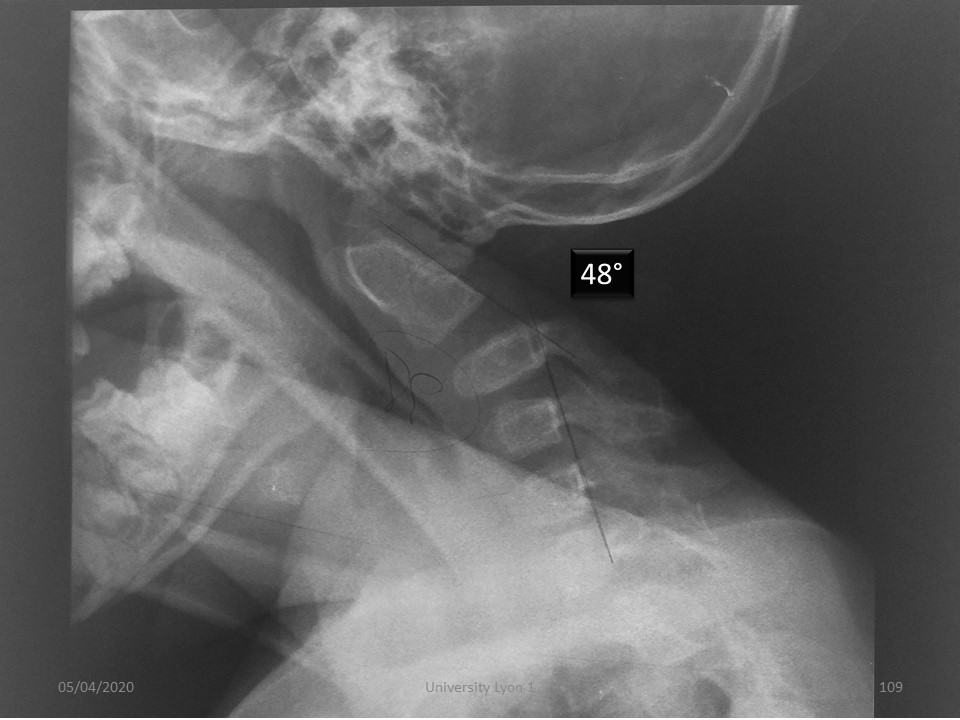 |
In this exceptional case of posterior agenesis C1-C2, with progressive hyperkyphosis C2-C3 of 48 °. the night Milwaukee brace was chosen from 3 years to 15 years. |
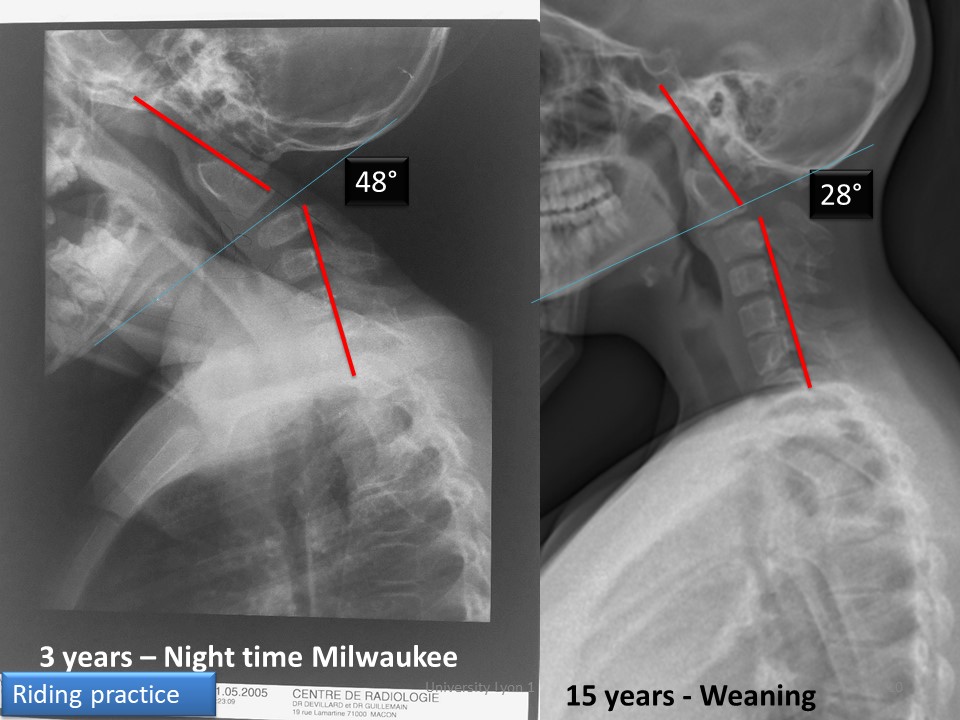 |
The result at the end of growth is spectacular. The child has led a normal life with riding practice. |
 |
The result at the end of growth is spectacular. The child has led a normal life with riding practice. |
 |
These indications are exceptional. In the majority of cases, the classic Lyon method is used with reduction by corrective plaster cast and then adaptation of a 5-point brace made of high-rigidity plastic. |
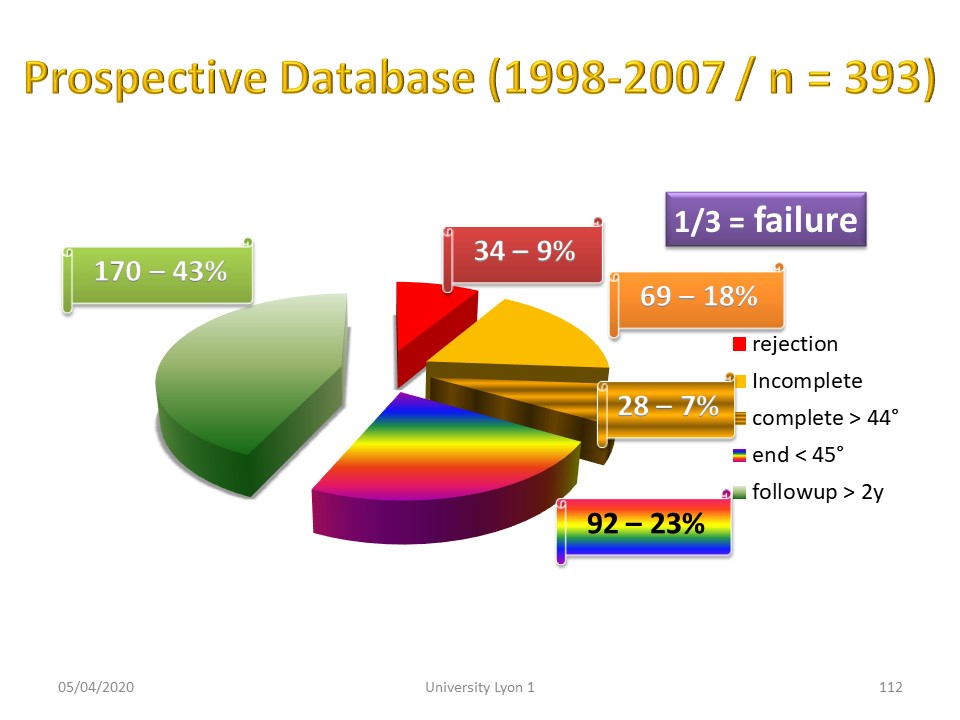 |
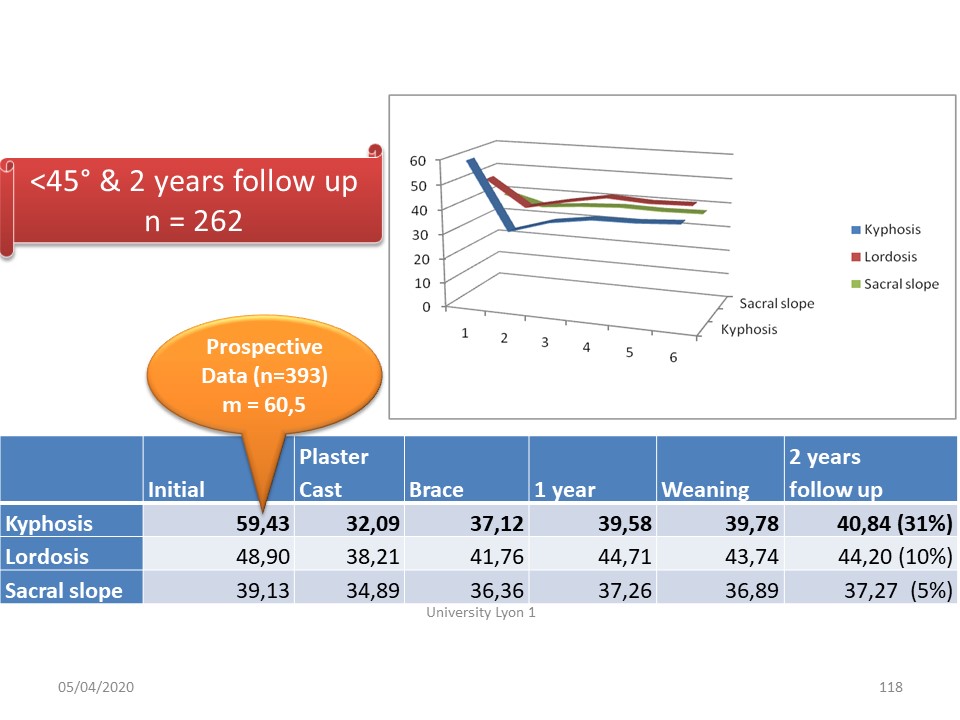
The results were presented through a retrospective study using a prospective database started in 1998. 43% of patients were seen 2 years after the orthosis was removed. |
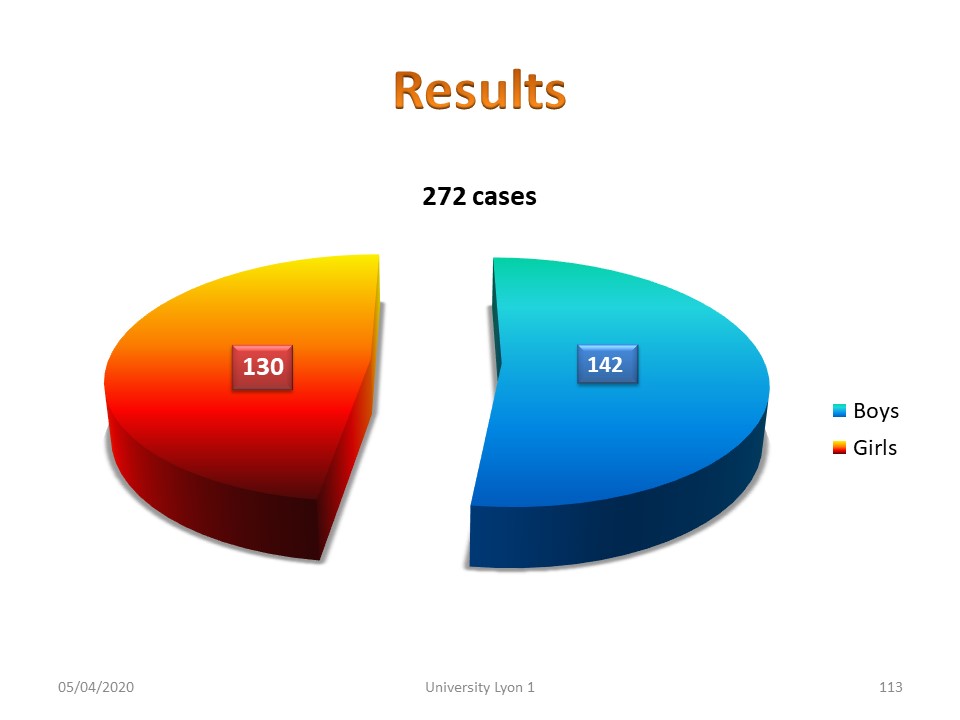 |
Contrary to scoliosis, the number of boys is slightly higher than that of girls. |
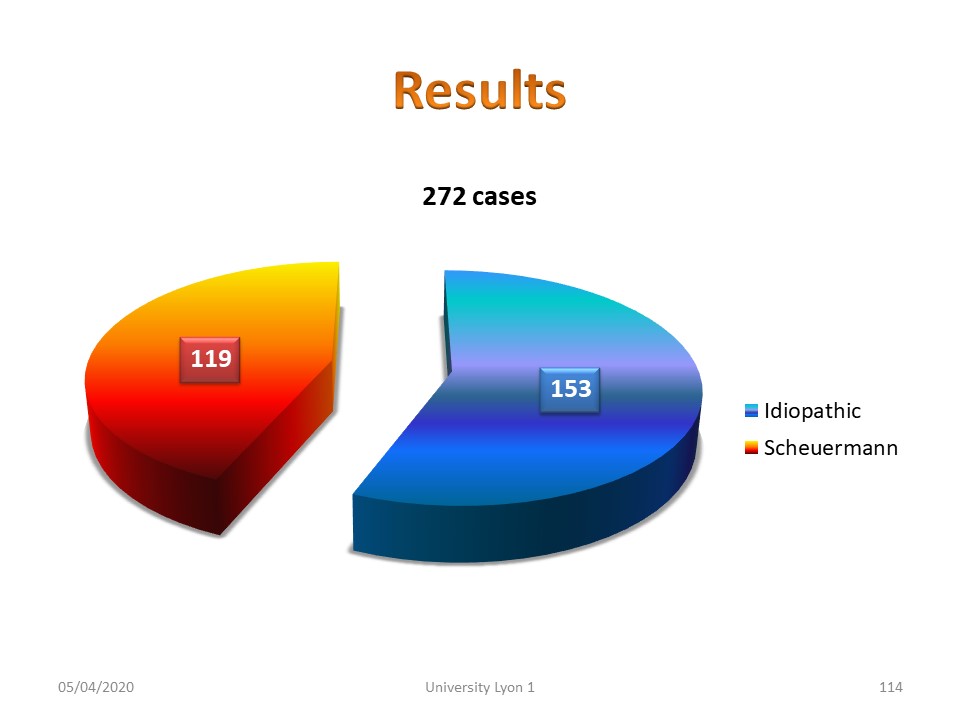 |
Similarly, unlike scoliosis, kyphosis due to Scheuermann's disease accounts for almost half of the patients. When the radiological lesions are minimal, we speak of idiopathic kyphosis. |
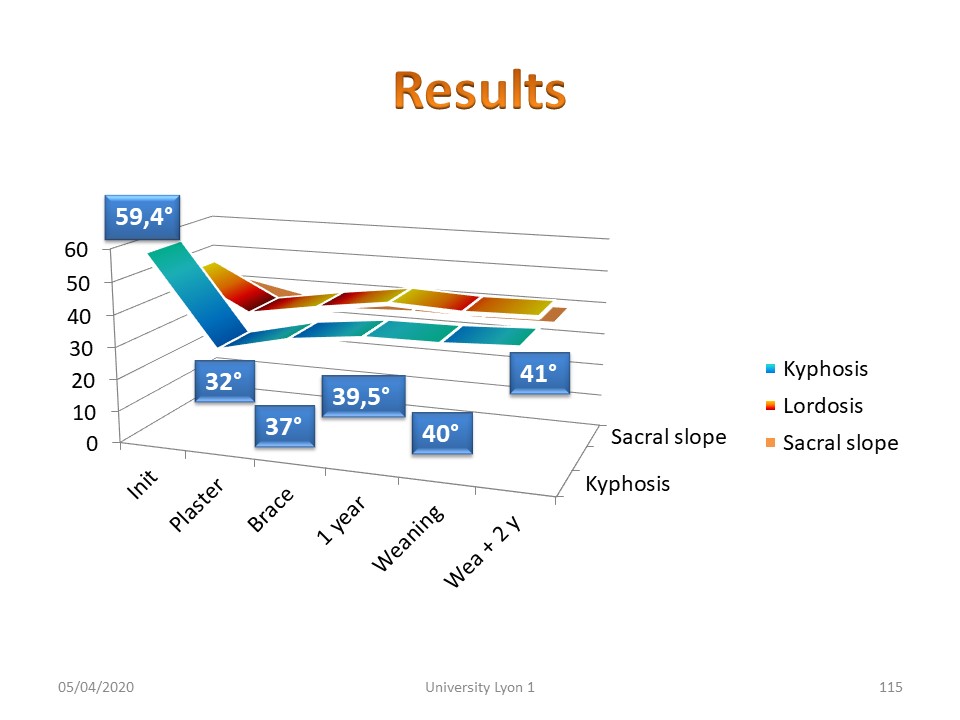 |
The Lyon method with plastic deformation gives very satisfactory results close to the average kyphosis in the general population. |
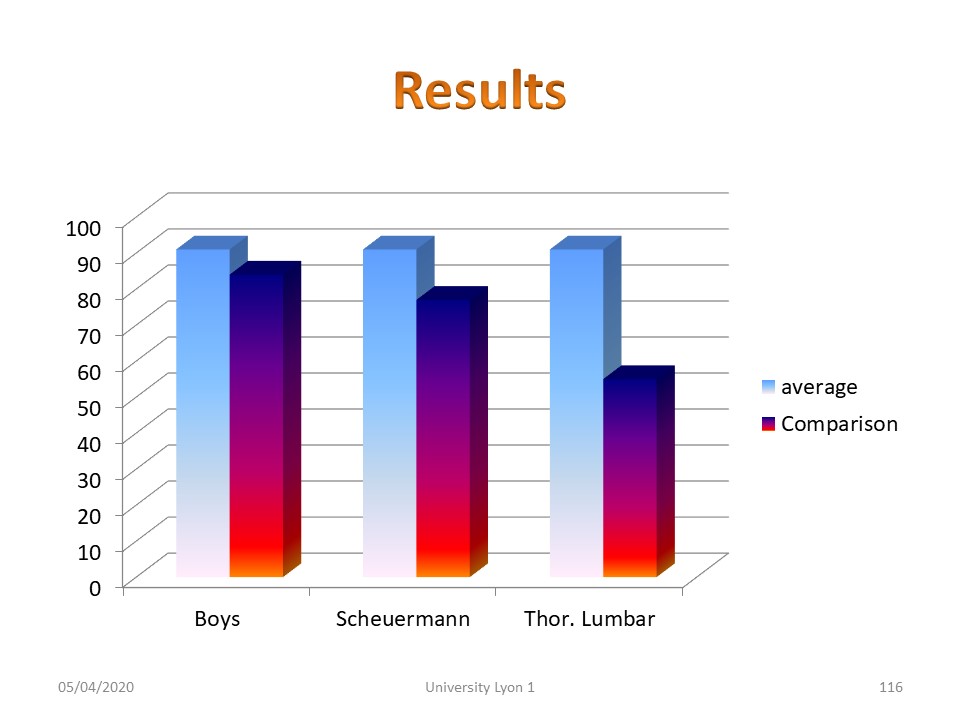 |
When comparing group averages, boys scored slightly lower than girls. The same is true for Scheuermann's radiological lesions. The worst results are obtained for thoracolumbar kyphosis. |
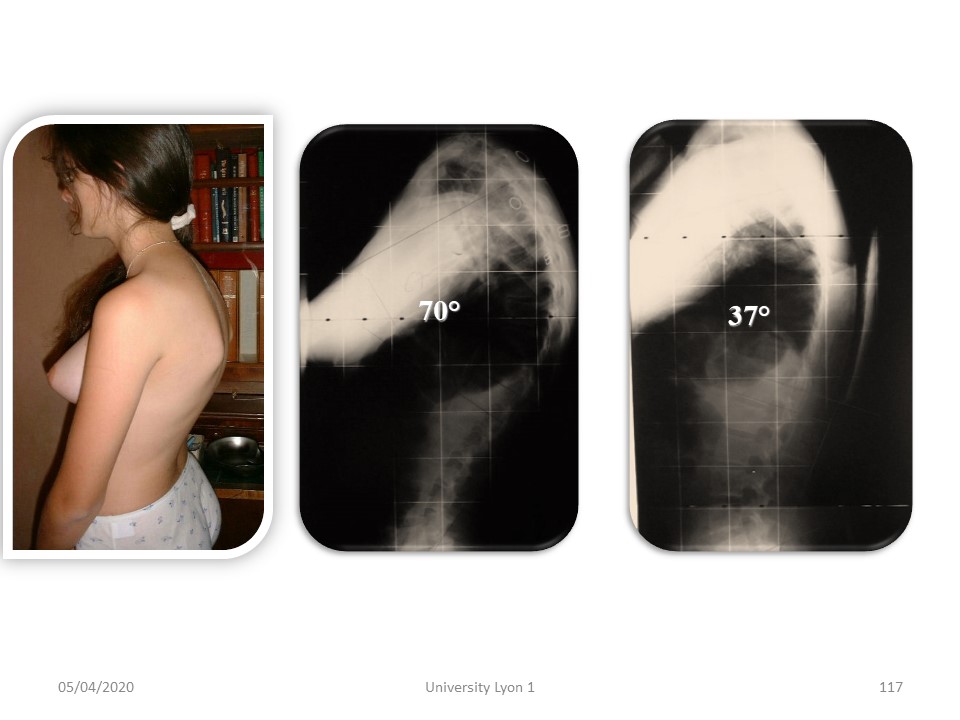 |
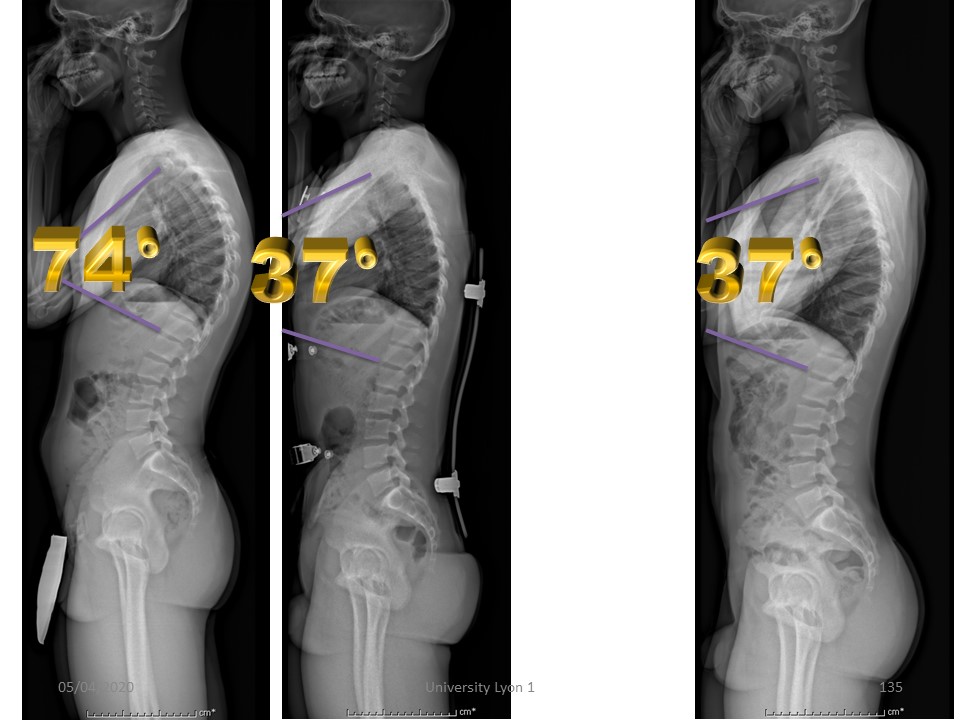
Here is a typical example of plaster cast reduction, reducing an angulation of 70° to a physiological angulation of 37°. |
 |
The correction obtained is maintained afterwards during the treatment. |
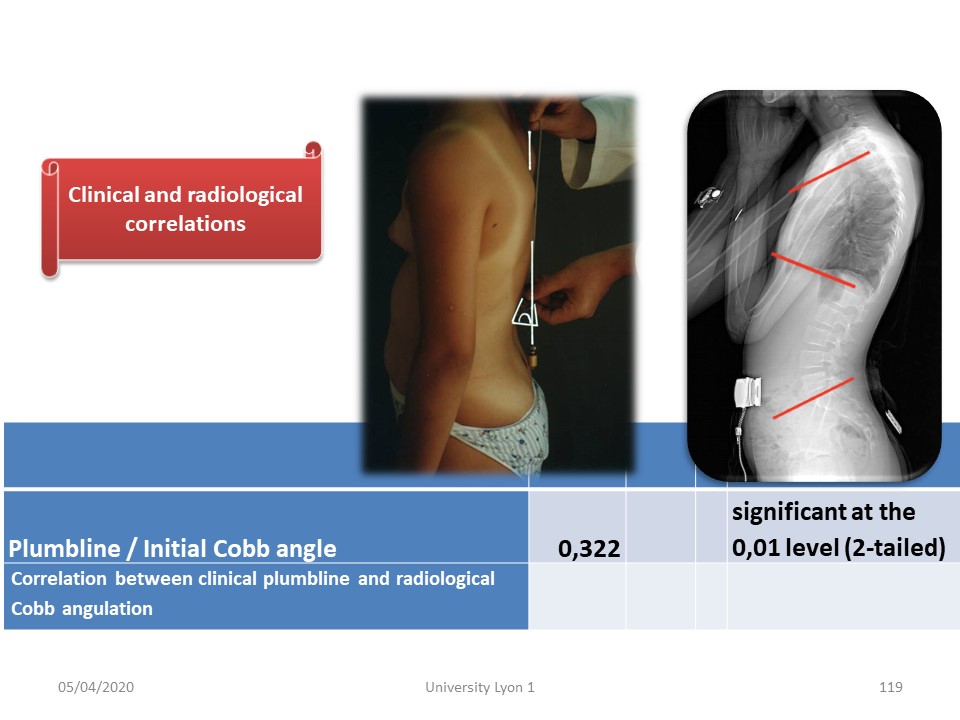 |
In contrast to scoliosis, there is a good correlation between clinical assessment with plumb line and radiology. |
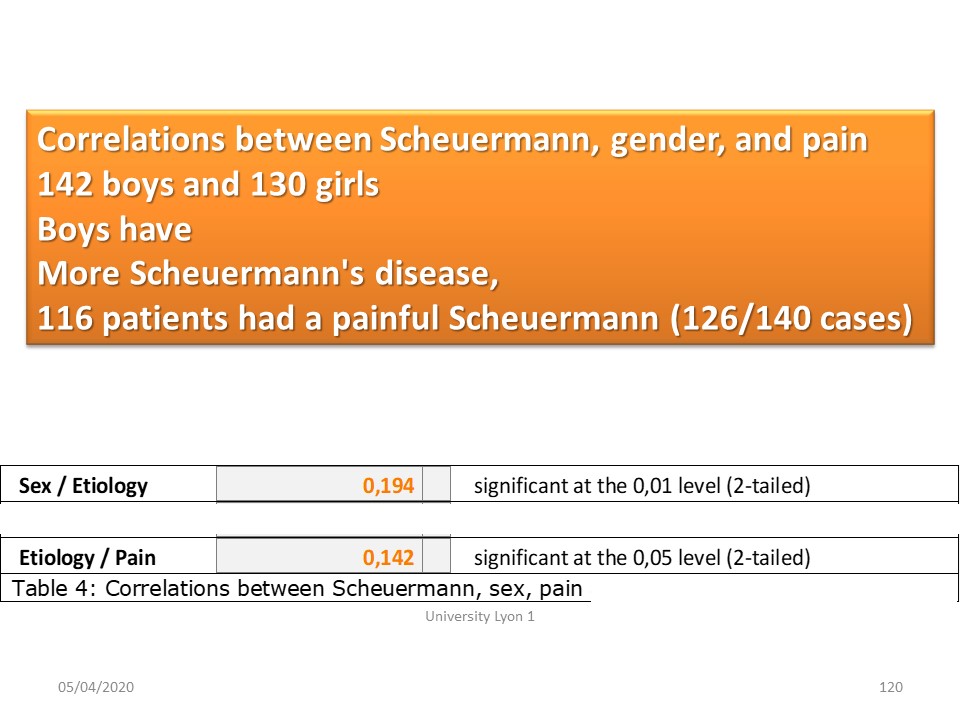 |
There is a moderate correlation by gender. Boys have a little more Scheuermann and therefore more pain. |
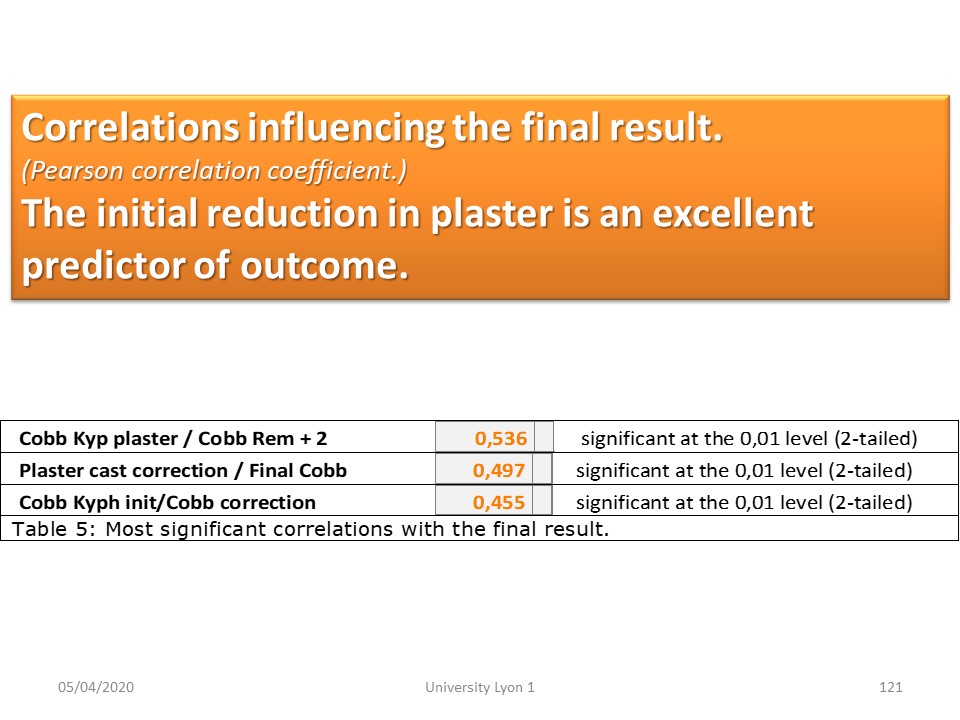 |
The correlations are more important with regard to the correction obtained in plaster cast and the final result of the treatment. |
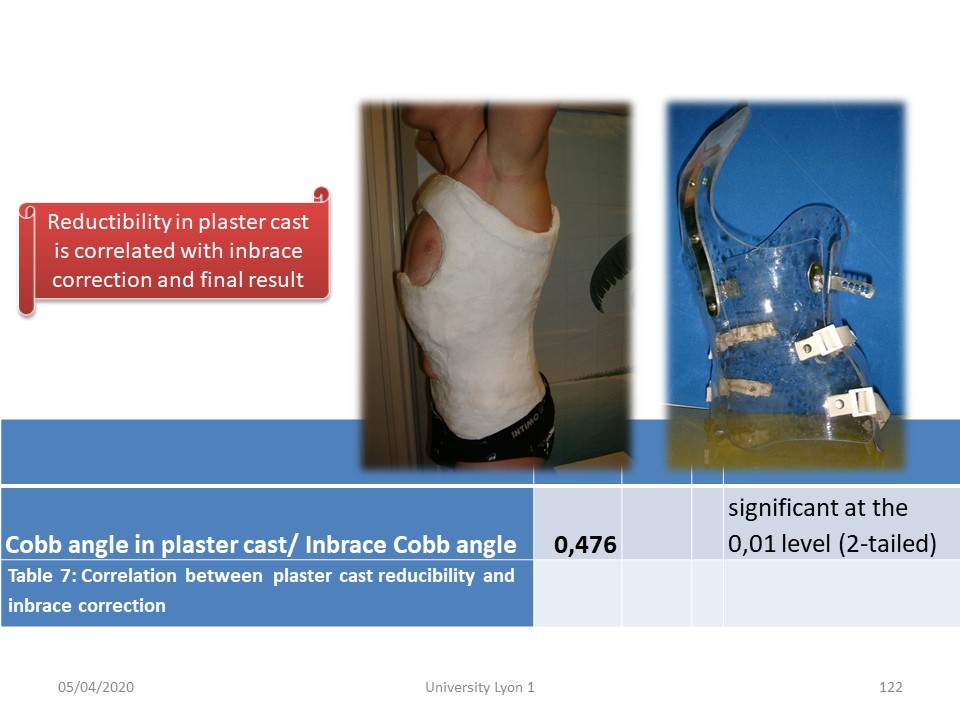 |
The reducibility of kyphosis and thus the stiffness of the curvature is therefore an essential prognostic element. |
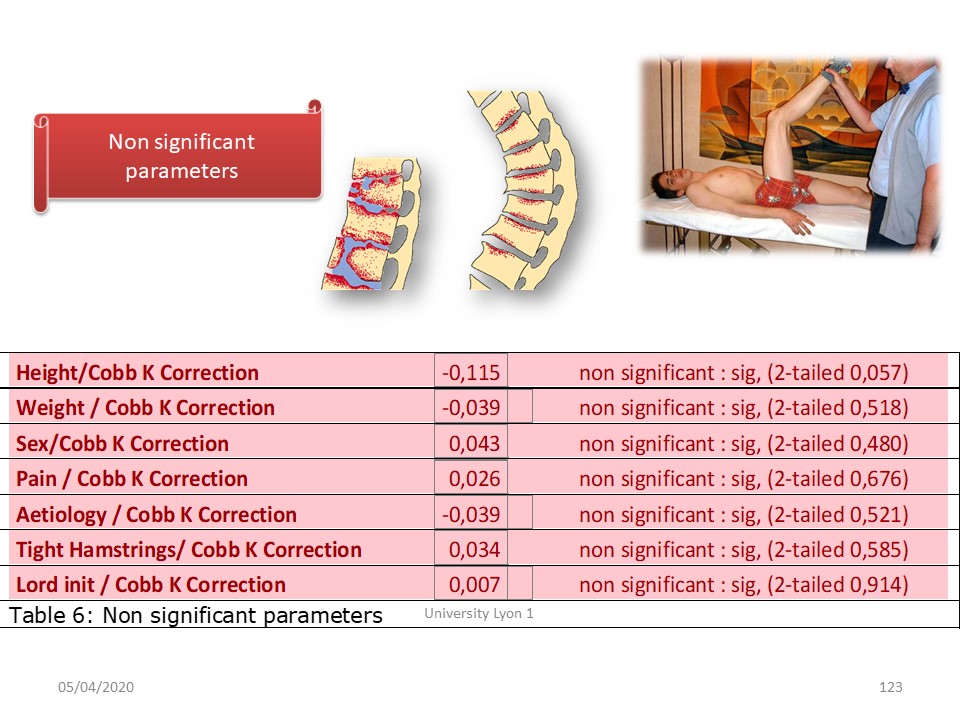 |
However, there are few predictive parameters for this plaster cast correction. Height, weight, sub-pelvic stiffness, gender, aetiology, pain, lordosis are not statistically significant. |
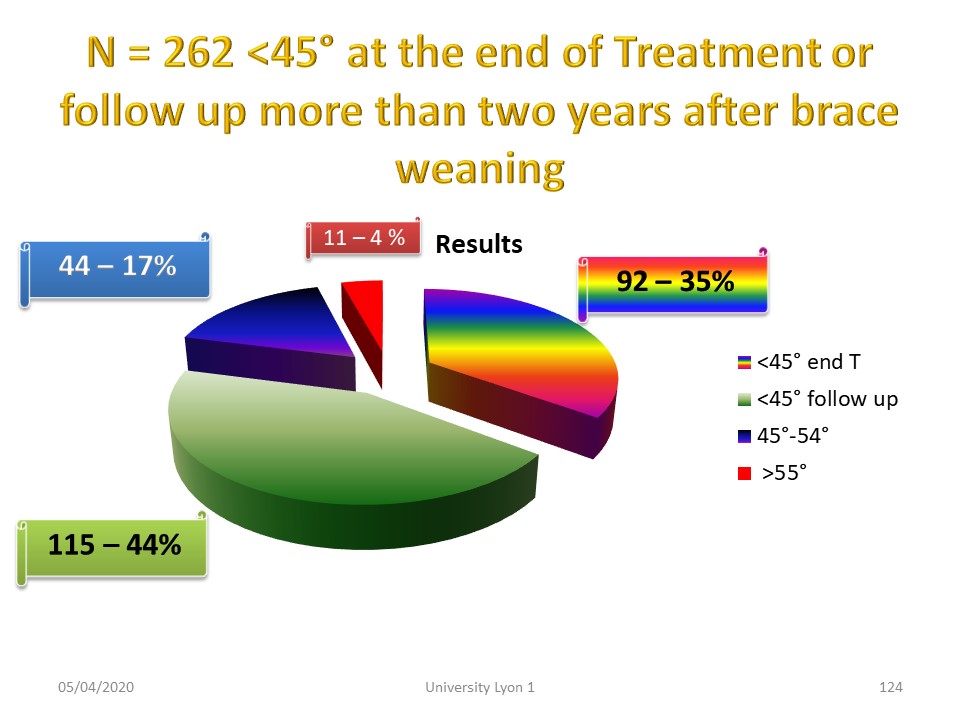 |
Interpretation of the results is difficult in kyphosis. Globally nearly 80% of patients have an angulation of less than 45° at the end of treatment, i.e. a quasi-physiological angulation. |
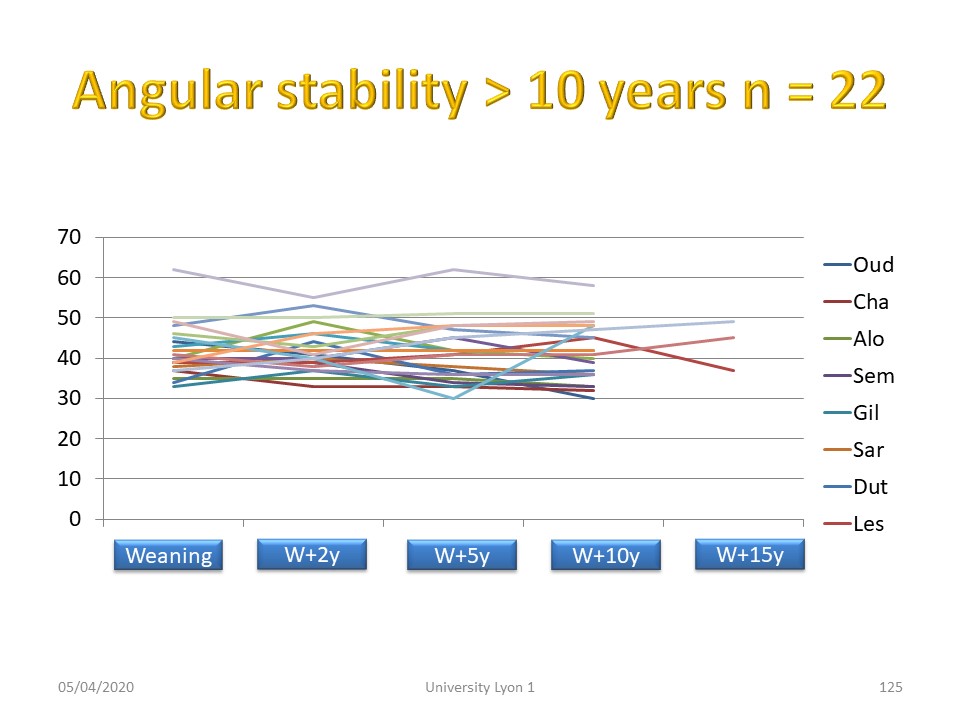 |
Stability is excellent in 22 patients seen more than 10 years after weaning. |
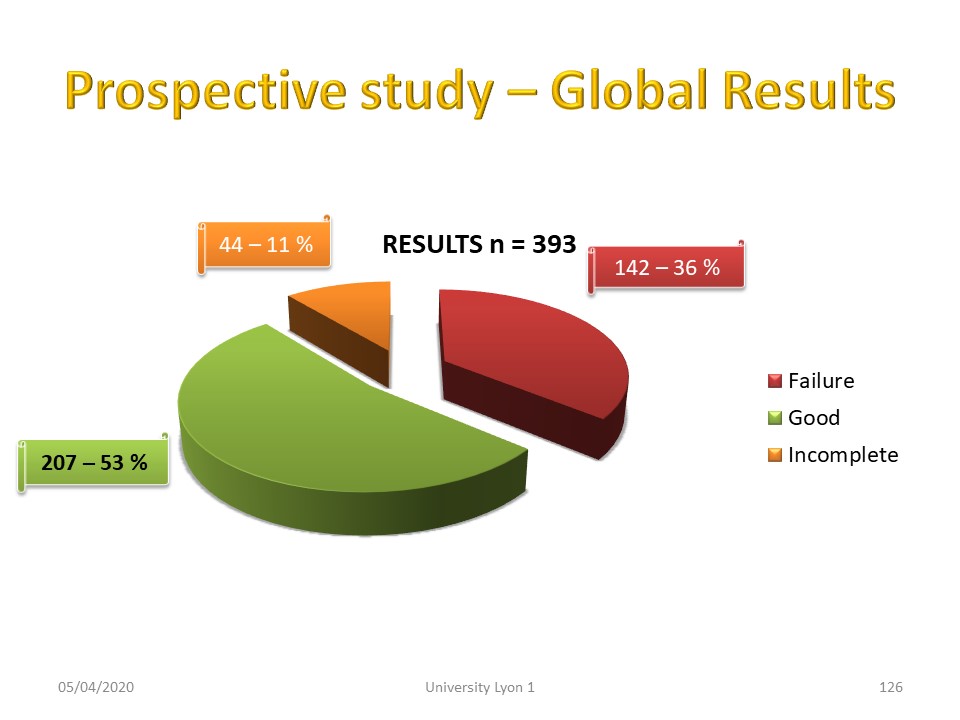 |
Including all treated patients, results are insufficient in almost 50% of patients, which explains the mistrust of doctors towards brace treatment. |
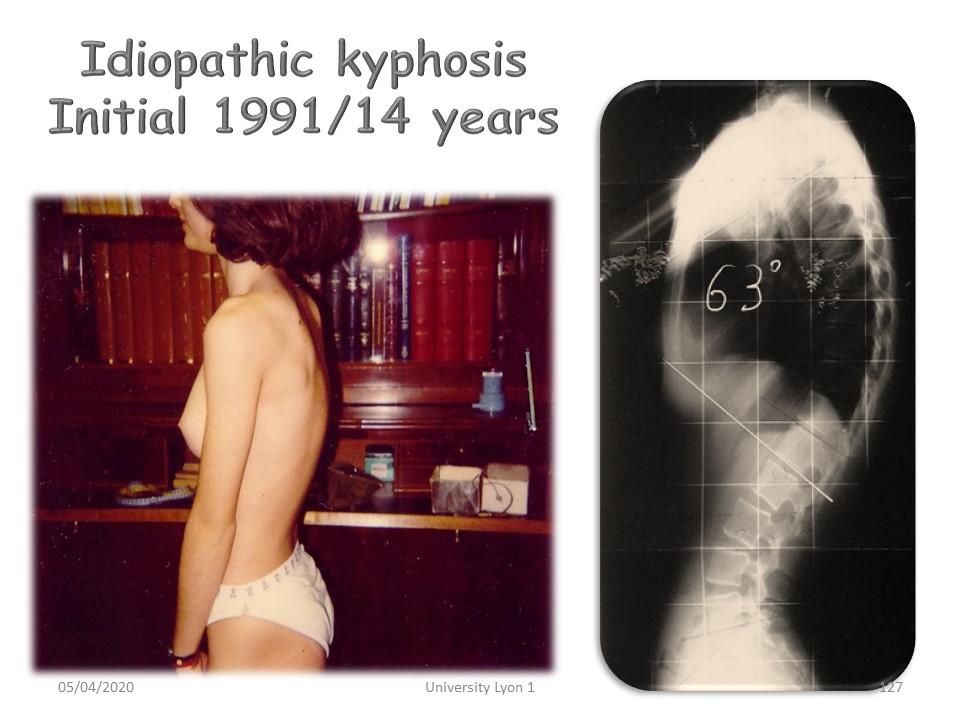 |
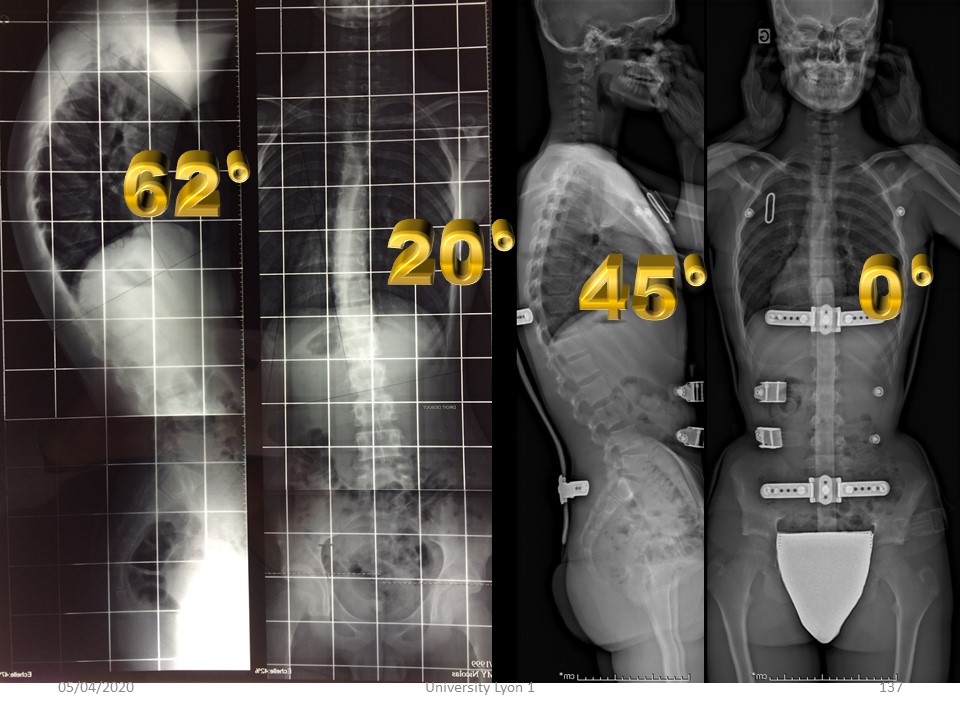
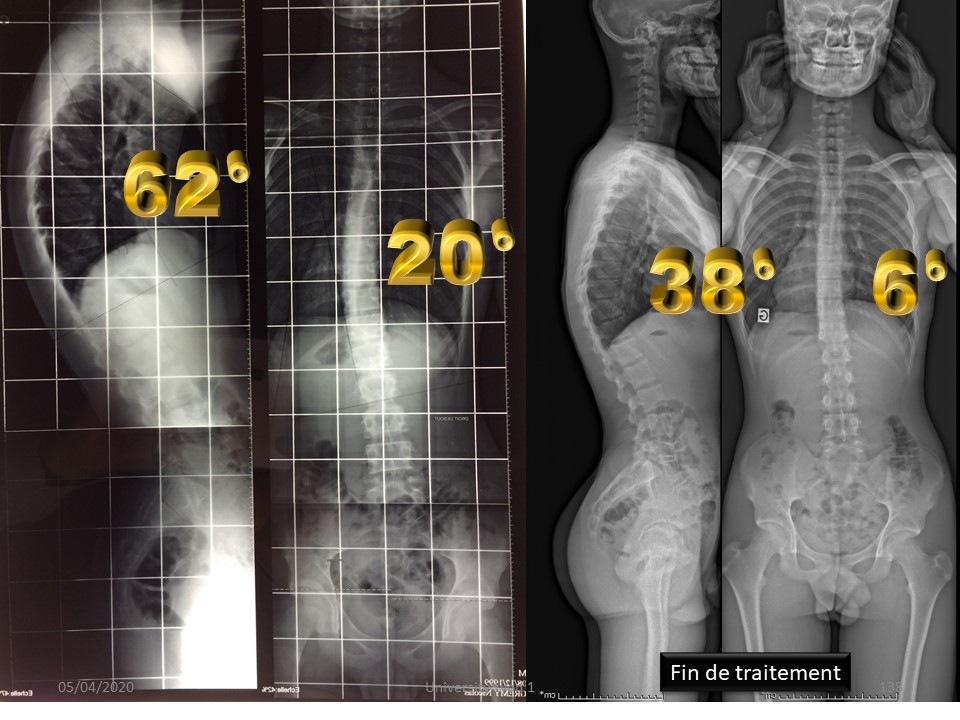
This child had kyphosis of more than 60° at the age of 14. |
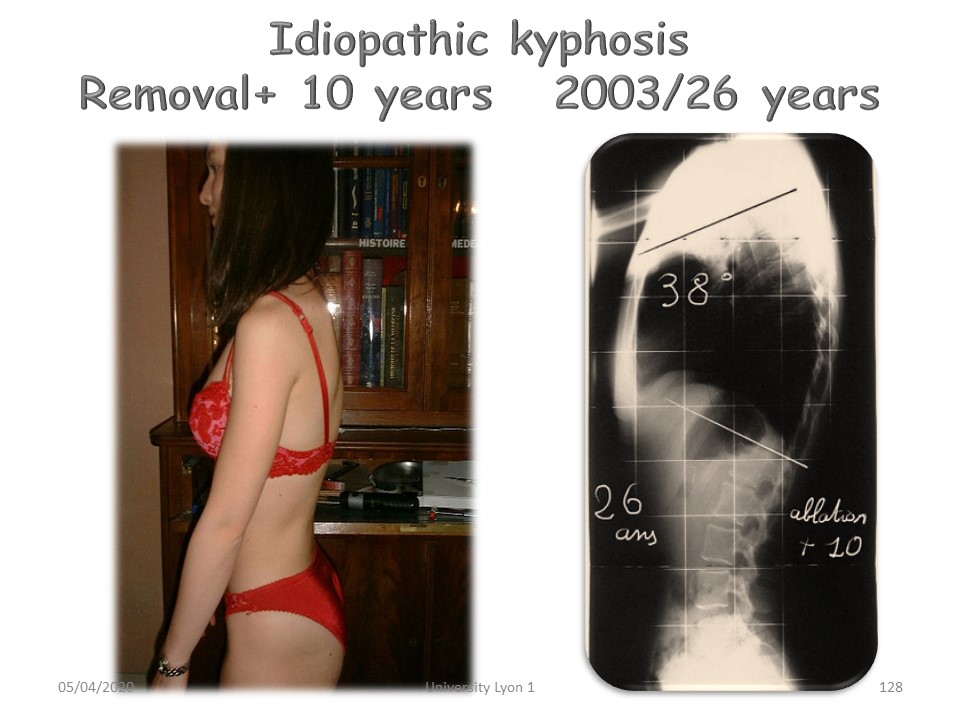 |
She was treated by the classical Lyon method and 10 years after the removal of the brace the angulation of the physiological kyphosis is maintained. |
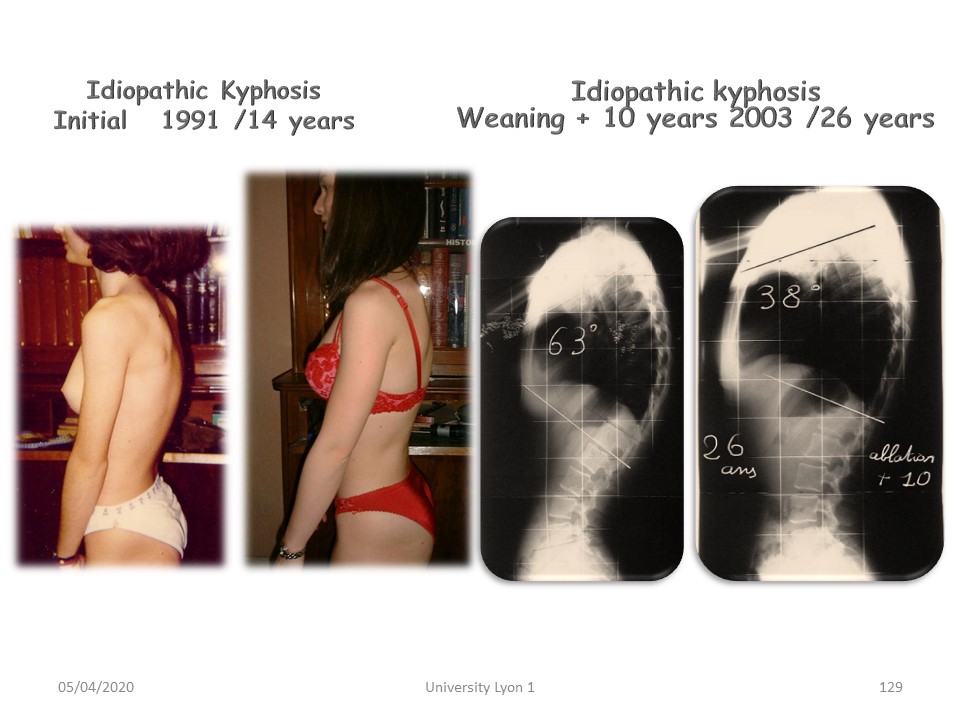 |
Non-surgical orthopaedic treatment can therefore be effective, as long as the protocol includes plastic deformation. |
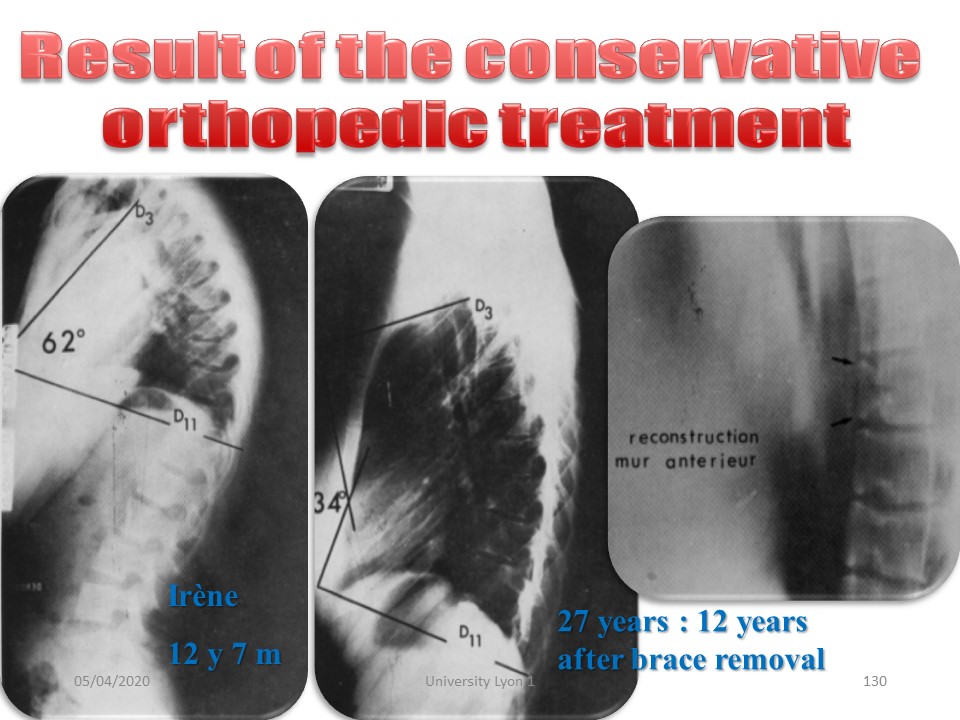 |
In some cases of Scheuermann disease, reconstitution of the anterior wall from the listel has been demonstrated. |
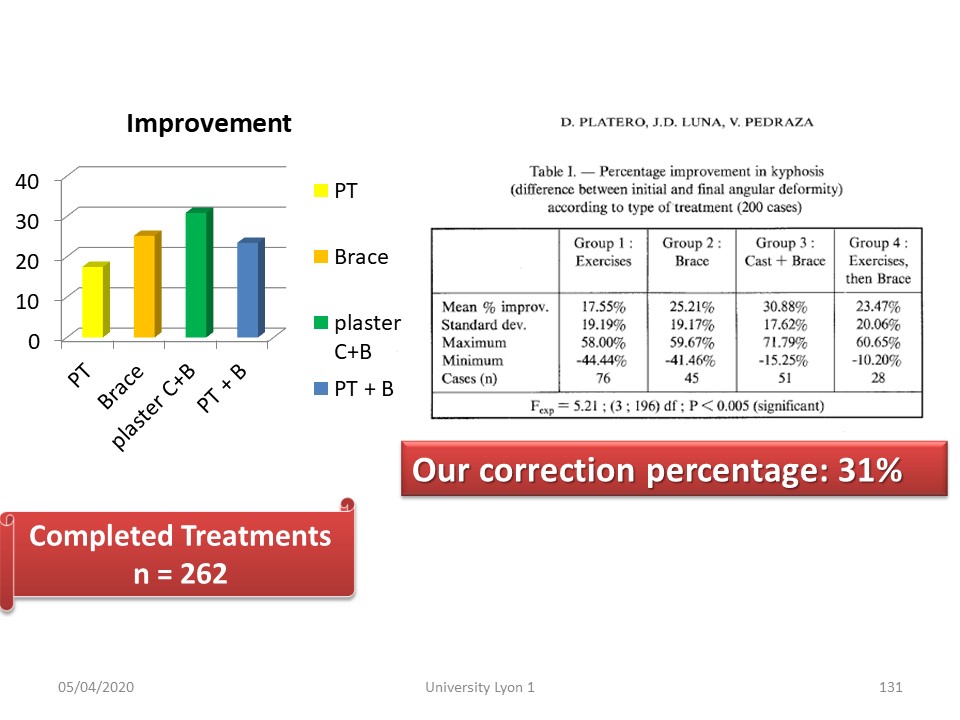 |
In Spain, Platero confirms that the best final correction is obtained in the group combining plaster cast and brace. |
Comment in the certification part of the website
|
|
 |
Europlex’O has the advantage of being lighter, stronger and more insulating than the old polymethacrylate. |
 |
The brace here is made of Europlex'O bivalves nested on the side. The Sforzesco brace without asymmetrical padding or the ARTbrace can also be used. |
 |
The total correction obtained in ARTbrace is maintained at the end of treatment, on an X ray without brace. |
 |
The kyphosis ARTbrace is closer to that of adult scoliosis with the posterior part stopping under the apex of the kyphosis backwards and the sub axillary trim line going forward towards the clavicle. |
 |
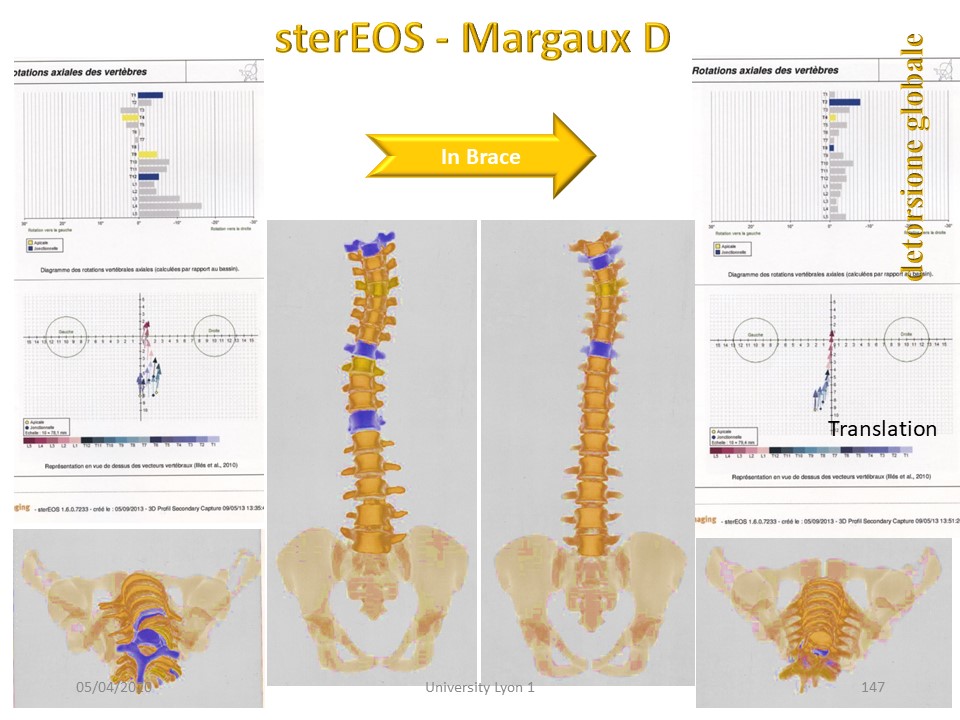
When the hyperkyphosis is associated with a frontal deviation, the ARTbrace remains the ideal brace. It controls both scoliosis and kyphosis. In brace, correction of scoliosis is total, and correction of kyphosis partial. |
 |
But the correction in the sagittal plane will continue throughout the treatment with, at the end of treatment, restoration of almost physiological curvatures. |
 |
Here is the clinical aspect at the end of treatment. |
 |
The reducibility test shows that there is still a small reserve in spine extension. |
 |
In this 10-year-old patient, scoliosis is associated with a flat back. |
 |
In the ARTbrace, scoliosis and pelvic rotation are well corrected. |
 |
In the sagittal plane, a quasi-physiological thoracic kyphosis is restored. |
 |
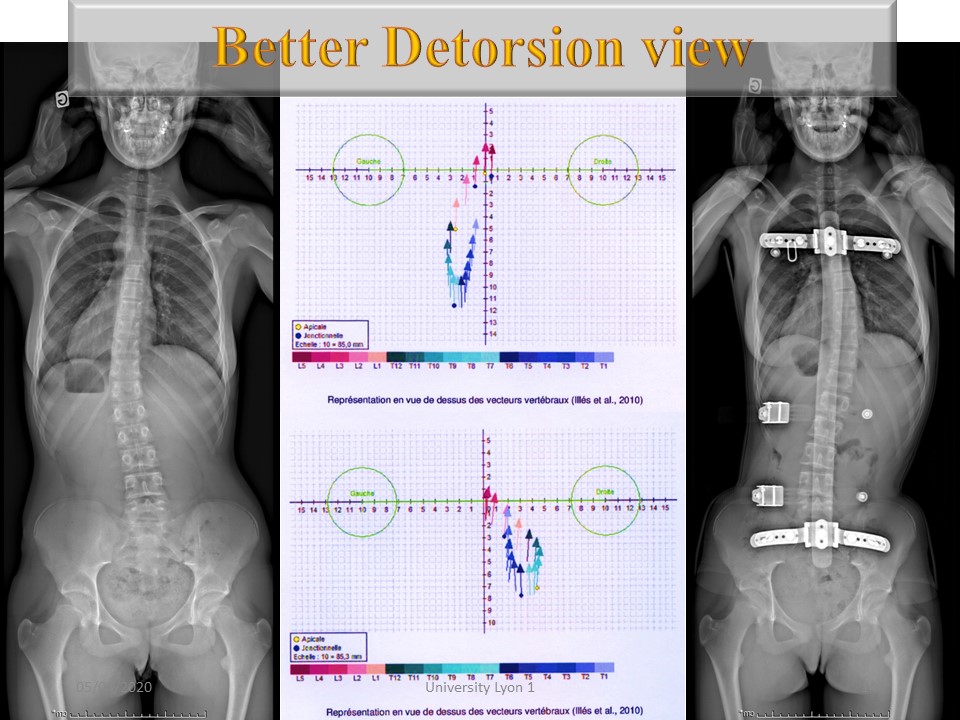
The EOS-3D representation shows the correction in the frontal plane. |
 |
And the restoration of kyphosis in the sagittal plane. |
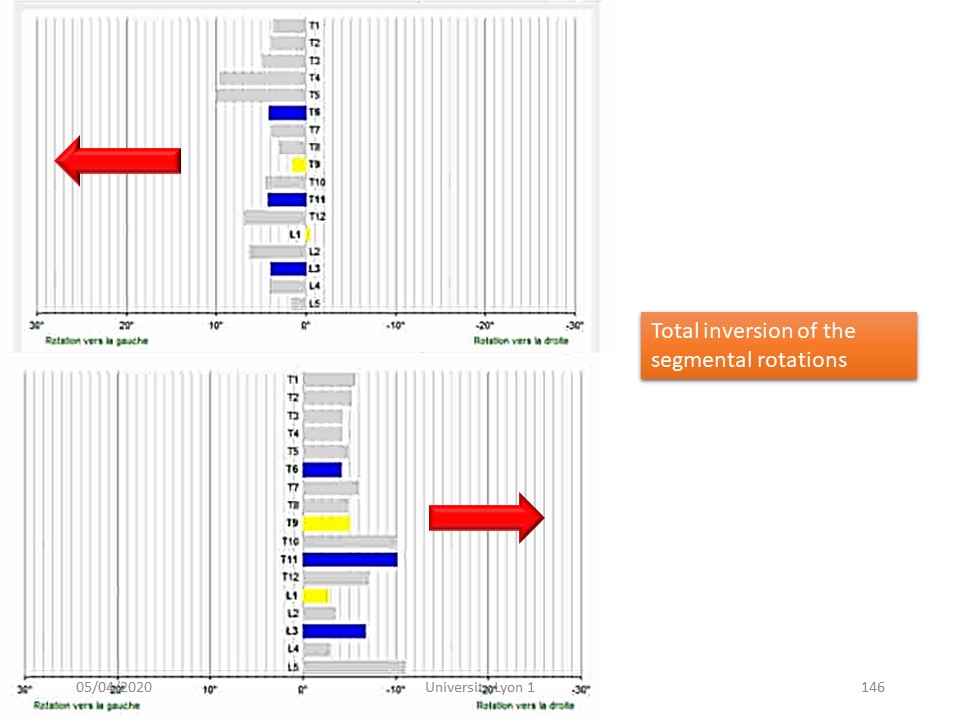 |
In the horizontal plane, the rotations are generally reversed. |
 |
The 3D effect of ARTbrace is also significant in the upper thoracic region as seen in this example. |
 |
The torso column in opposite direction of initial scoliosis can totally reverse the curve when there is no deformation of the vertebral body. |
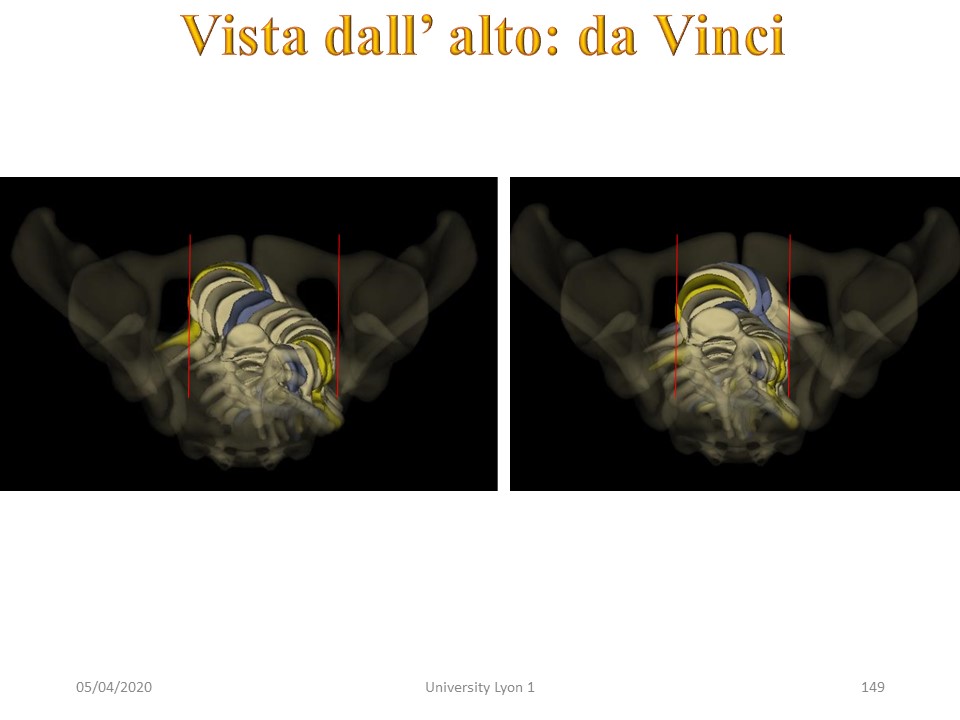 |
This correction in the frontal plane and in the sagittal plane is associated with a refocusing of the vertebral bodies on the line of gravity, clearly visible on this "Da Vinci view". |
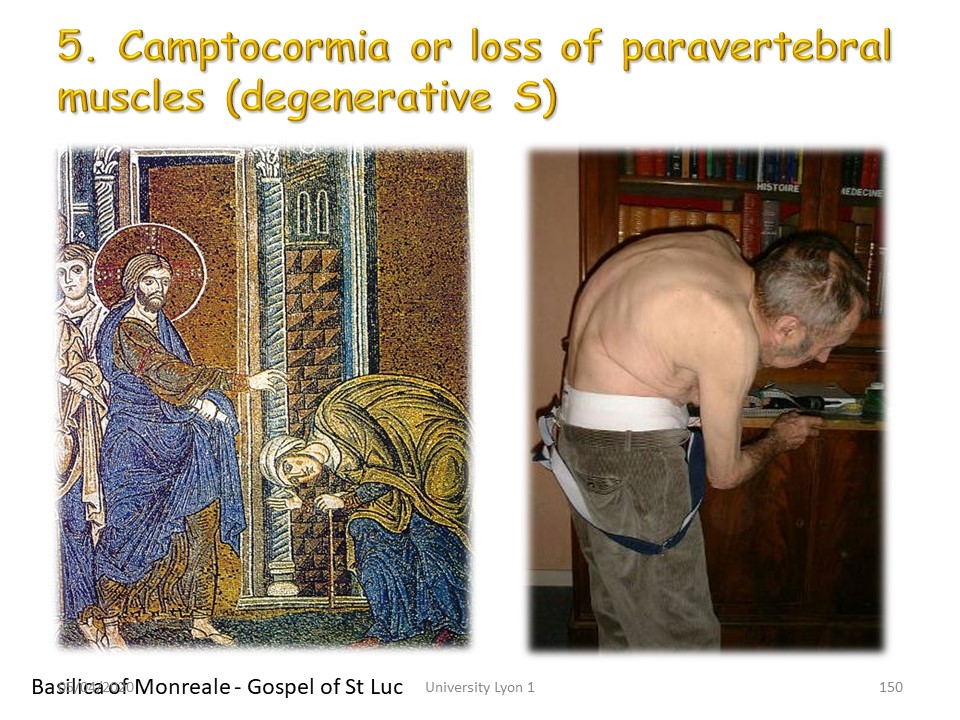 |
We've already discussed Pisa syndrome and camptocormia. Camptocormia is linked to weakness of the deep posterior musculature. The patient increases kyphosis gradually to tighten his weak paravertebral muscles. There is often an extra-pyramidal context of Parkinson's disease. Some have mentioned paravertebral myopathy. The miraculous healing of such kyphosis is quoted in the Gospel of St. Luke and depicted on the mosaics of the Basilica of Montreale in Palermo. |
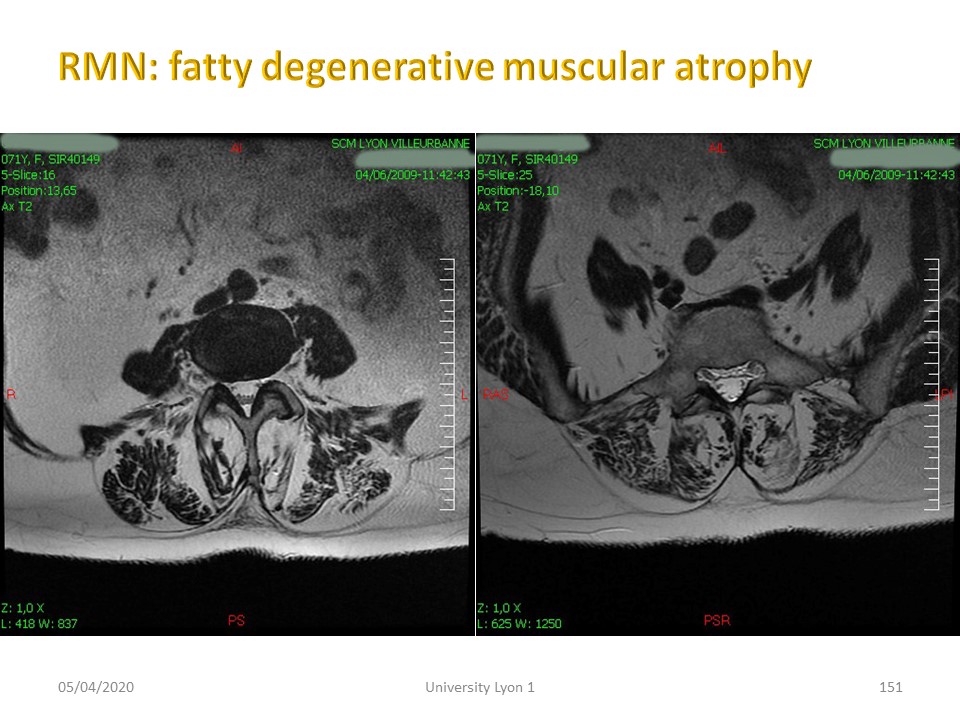 |
MRI cross sections highlight the fatty degeneration usually of extra-pyramidal origin with alteration of the reticulo-spinal system. |
Comment in the certification part of the website
|
|
 |
The new Lyon ARTbrace results from the technological evolution, but especially from the fantastic research work carried out during the last 15 years within the SOSORT. In addition to the technicality of the orthotist, thank the physiotherapist permanently encouraging the child and potentiating the results of the brace. |
 |

