 |
The SOSORT guidelines concerning the practice of sport are clear. Sport is not a treatment for scoliosis, the practice of sport is recommended, the practice of a sport should not be interrupted by treatment except during the total time period when the wearing of the brace is incompatible with sport practice.
|
 |
.
|
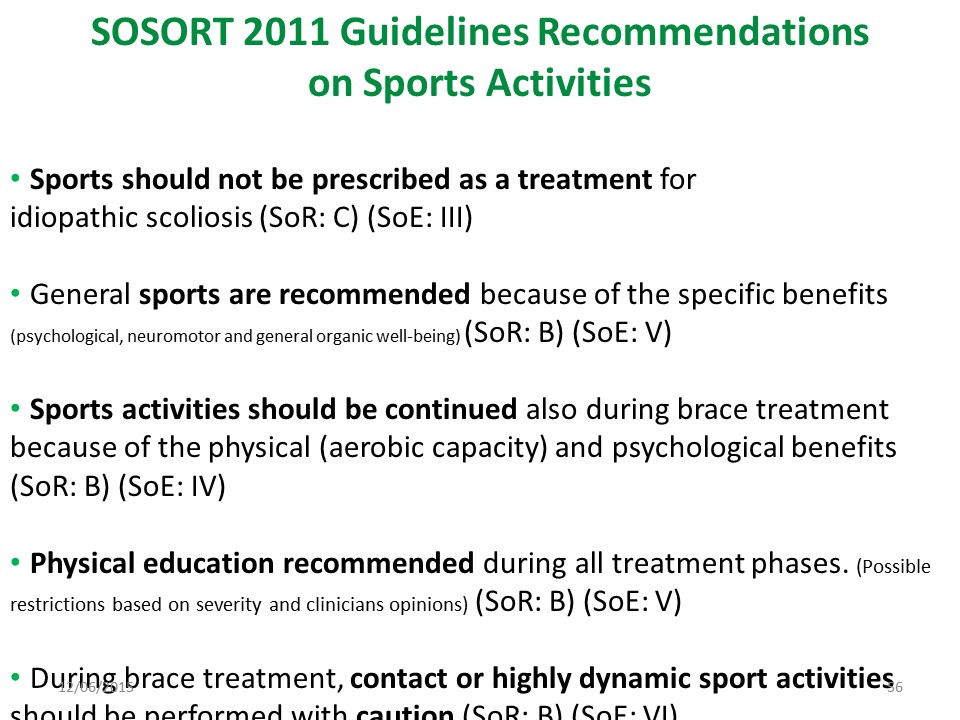 |
The SOSORT guidelines concerning the practice of sport are clear. Sport is not a treatment for scoliosis, the practice of sport is recommended, the practice of a sport should not be interrupted by treatment except during the total time period when the wearing of the brace is incompatible with sport practice.
|
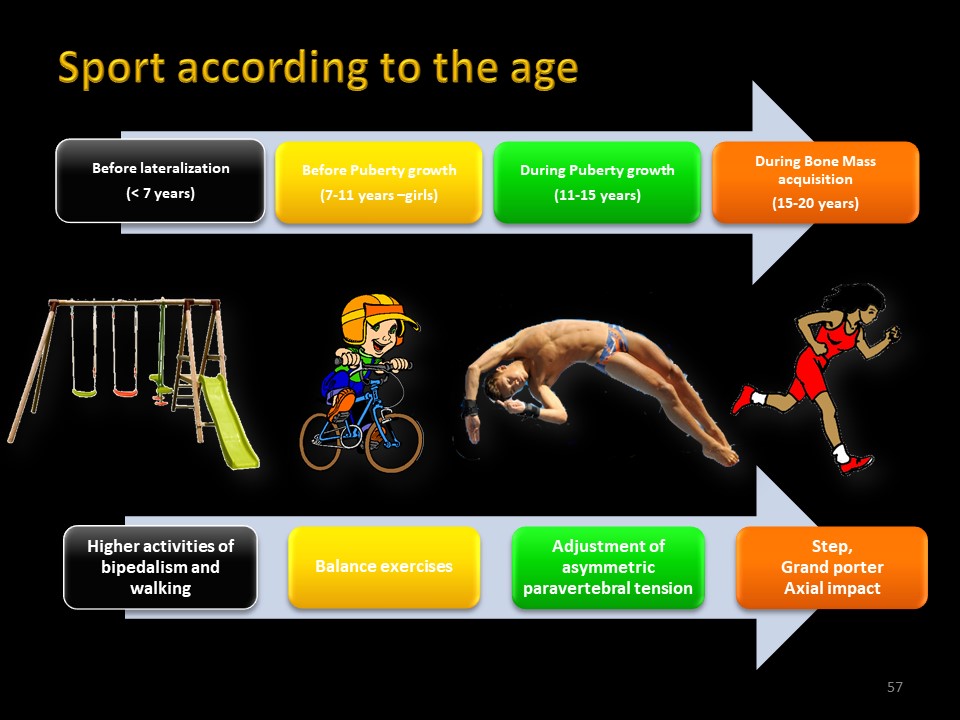 |
The practice of sport must be adapted to the age of the child. Before the age of 7, the child registers in the extra-pyramidal system (reticulospinal tract) all the automatisms of the bipedal station, of walking and running which is the characteristic of homo sapiens. Between 7 years and the start of puberty, the activities of balancing the vestibulo, rubro and tecto-spinal tracts will be favoured: cycling, gymnastics, ball games, dance ... During the pubertal phase, which corresponds to a 25 cm growth at the spine level, the adjustment of paravertebral tensions will be favoured by swimming, combat sports, climbing. .. At the end of height growth, period of maximum fragility of the bone, it is necessary to favour activities with an axial impact such as jogging, running ...
|
 |
At the Center des Massues until the 1980s, sport was integrated into physiotherapy and the sporting gesture possibly modified depending on the pathology.
|
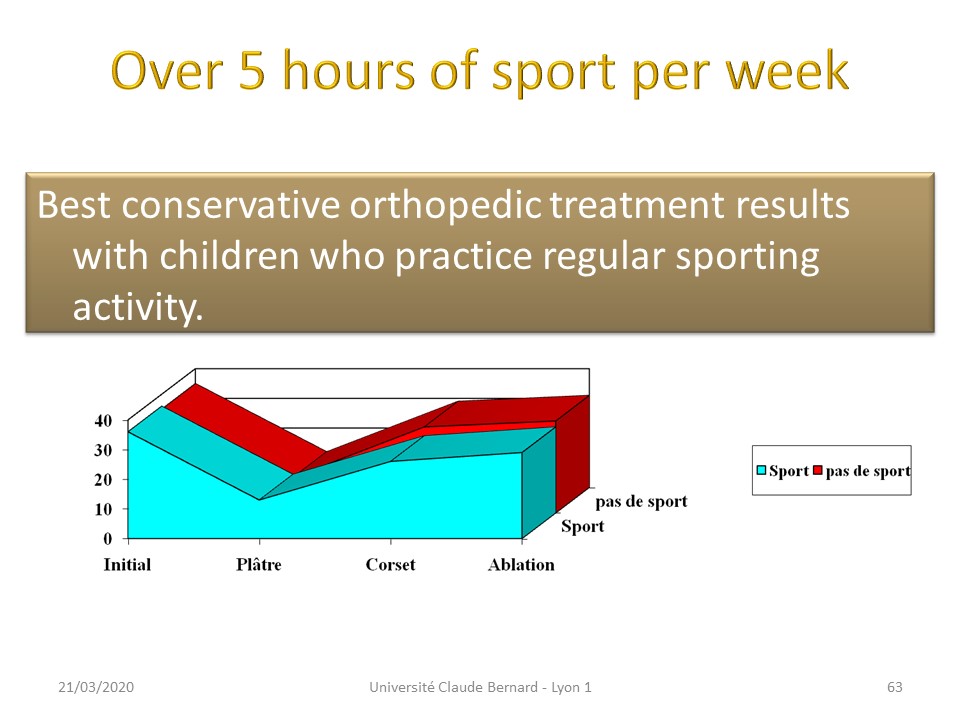 |
During the statistical evaluation of treatments by the Lyon brace, we isolated the patients practicing more than 5 hours of sport per week and compared the results with those of the general statistics. The results are significantly better with sport activity.
|
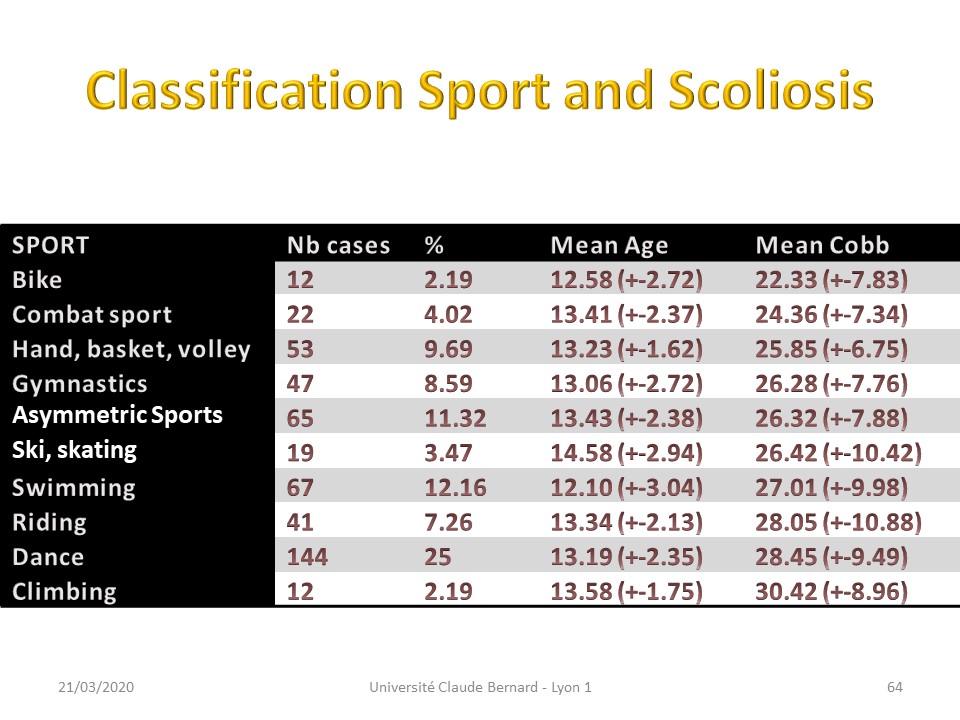 |
Parents often ask the question of the best sport to practice in scoliosis. It is difficult to statistically compare different sports. The only indication is the average initial angulation of scoliosis at the first specialized examination. If we admit that low initial angulation is a factor in the success of orthopaedic treatment, cycling and combat sports would be advisable.
|
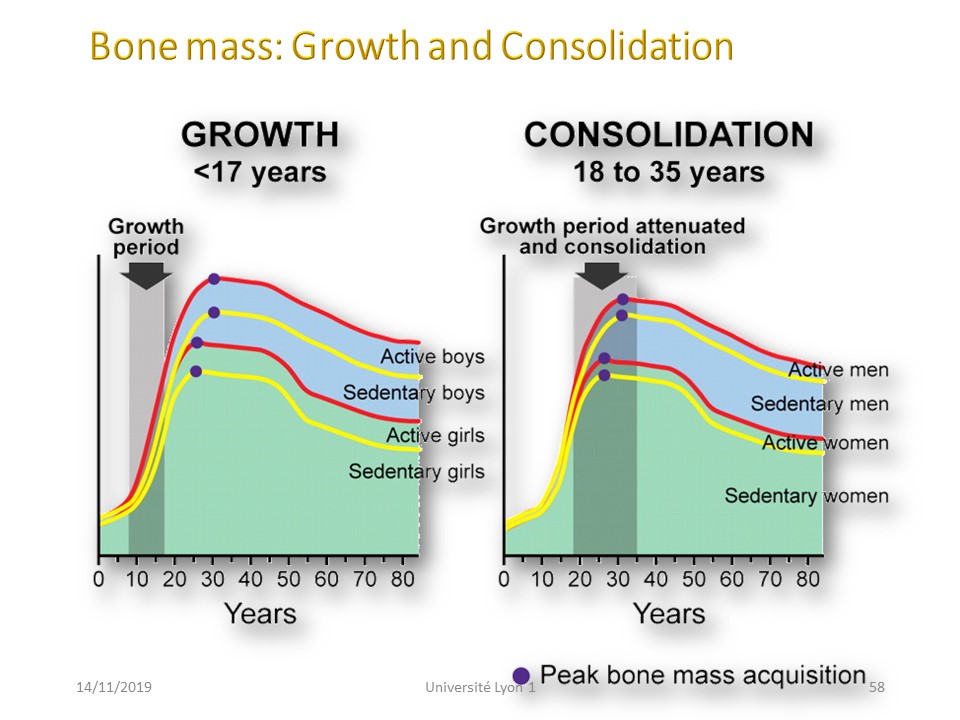 |
Puberty growth is unique to homo sapiens and theoretically allows it to reproduce in a shorter time. However, it does not accelerate bone mass, which in girls will double between 14 and 21 years of age. It is the mechanical energy directly transmitted by the impact of the foot on the ground that will transform into piezoelectric current at the level of the spine and promote the fixation of calcium on the bone. In case of scoliosis, this "bone fragility" explains the evolution of some scoliosis after Risser 3.
|
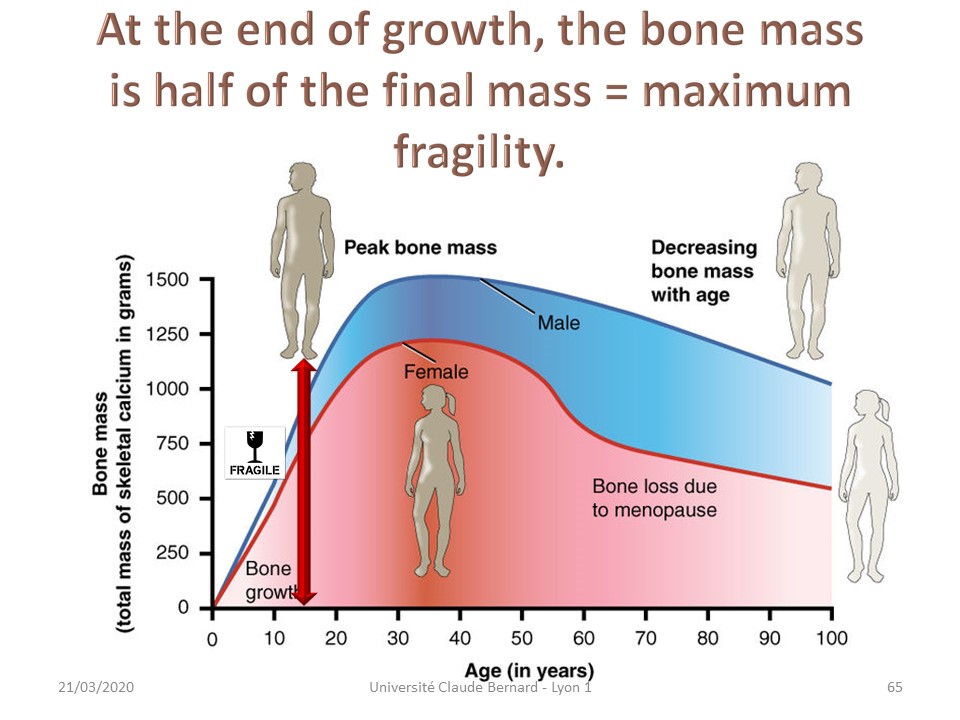 |
A special case concerns scoliosis at the end of the height growth (Risser 4). At this age the bone mass is not totally constituted and the objective is to promote the fixation of Calcium on the bone. The axial impact on the heel will transmit energy to the spine and create a piezoelectric current stimulating osteoformation.
|
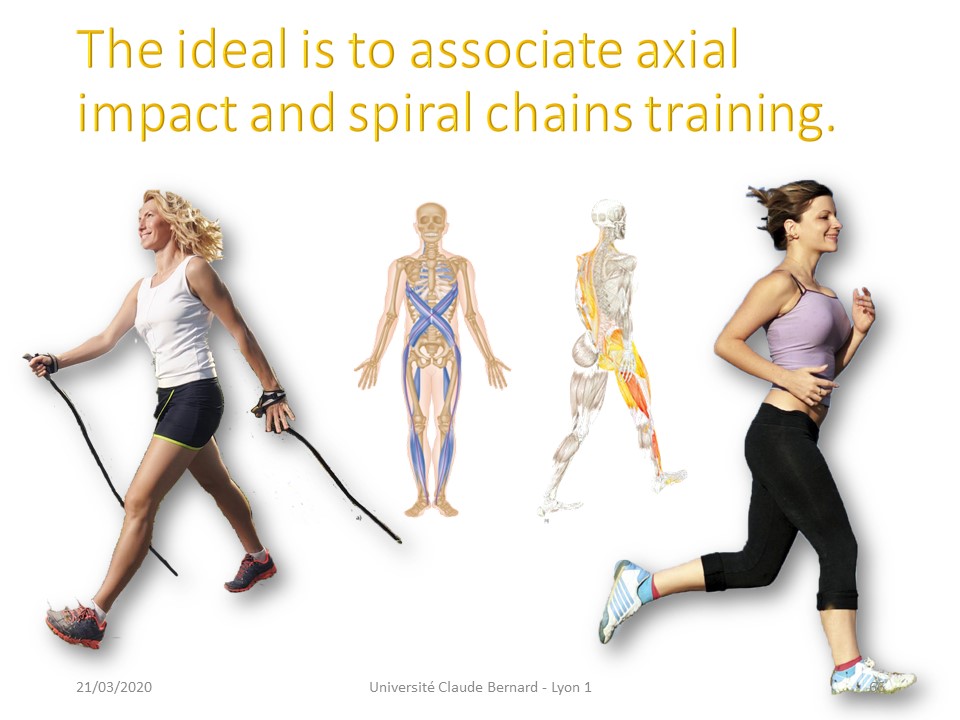 |
Jogging, running, dancing ... are very useful sports at this age, unlike swimming. Fish have no bones.
|
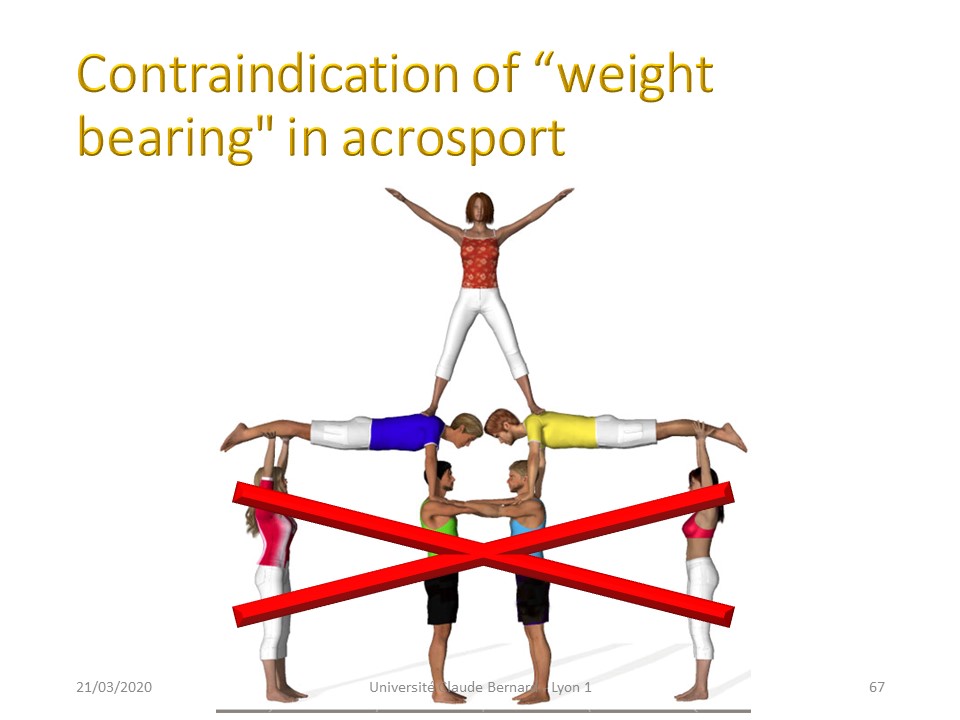 |
On the contrary, excessive axial loads, for example in acrosport, are contraindicated at this age. .
|
 |
.
|
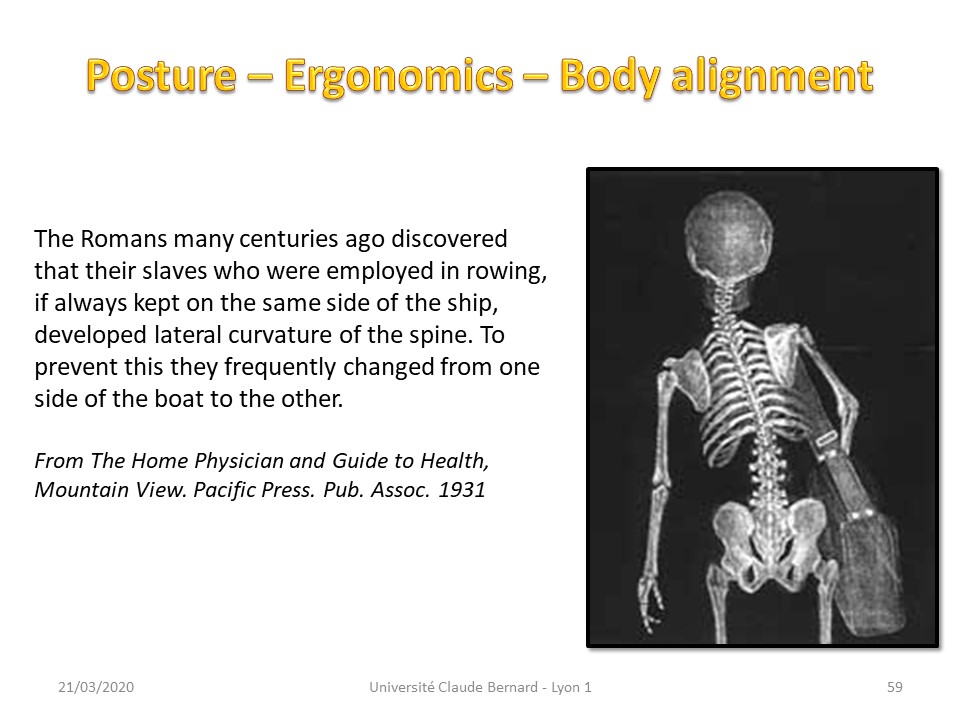 |
Wearing an asymmetric load on the shoulder will create a compensatory, homolateral attitude with contralateral misalignment of the occipital axis which will rebalance the loads at the apical vertebra. A second compensation takes place at the cervical level, because the vestibular system and the head must remain horizontal. As on the Roman galleys, the precautionary principle justifies alternating the load sometimes to the right and sometimes to the left, as we do spontaneously for a heavy load.
|
 |
In general, asymmetrical loads on the shoulders are to be avoided.
|
 |
It is preferable to wear the back pack balanced on both shoulders.
|
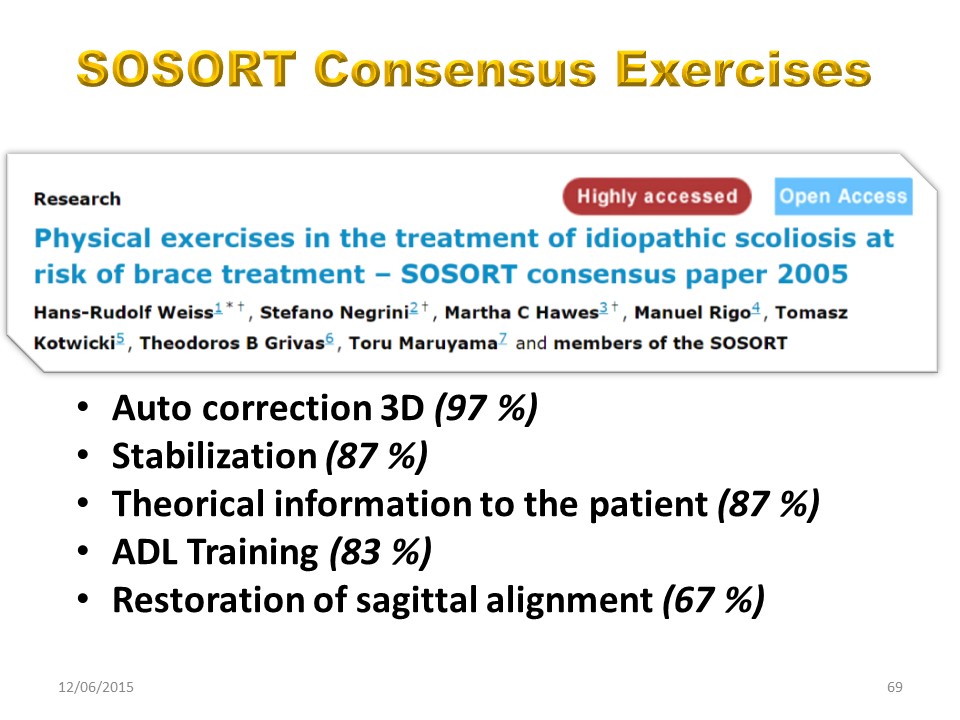 |
In conclusion, this already old publication highlighted the 3D self-correction exercises without explaining how to obtain it. In the same way the restoration of the sagittal alignment was evoked while all the techniques of the time went in the direction of the accentuation of the flat back. We now have the technological means to achieve these two objectives.
|
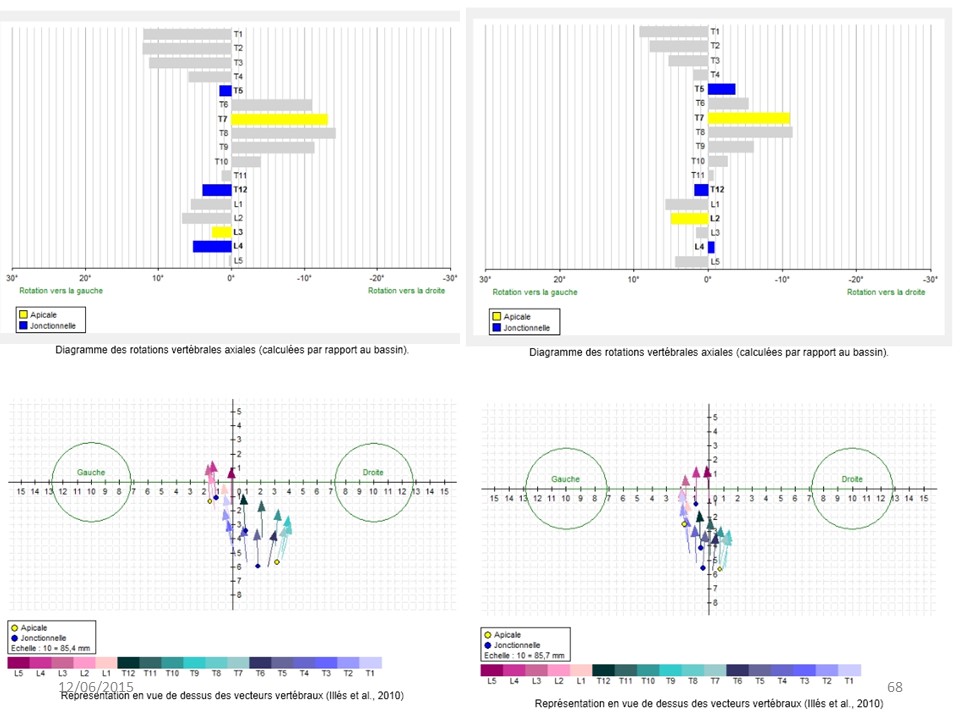 |
The evaluations by EOS, allow us to see scoliosis in 3 dimensions, especially since the brace is only the synthesis of all the corrections made by the physiotherapist.
|
 |
Physiotherapists now have the means to give the scoliotic child the best possible chance.
|
 |
|
 |
With Patrick Faouën our ergonomist, we realized this module to specify the adaptation of the sitting position for a schooled child, according to the morphotype.
|
 |
Sitting has often been parodied and is a major concern for parents. Computer use, more and more integrated to the professional activity, justifies indeed a correct sitting position.
|
 |
The usual habitual sitting position has always been on the ground with hips in external rotation. Only the king was sitting on a throne.
|
 |
Even during the Middle Ages, monks often copied books while standing.
|
 |
Young children at school begin to use the chair, but we can see that the postures are very varied.
|
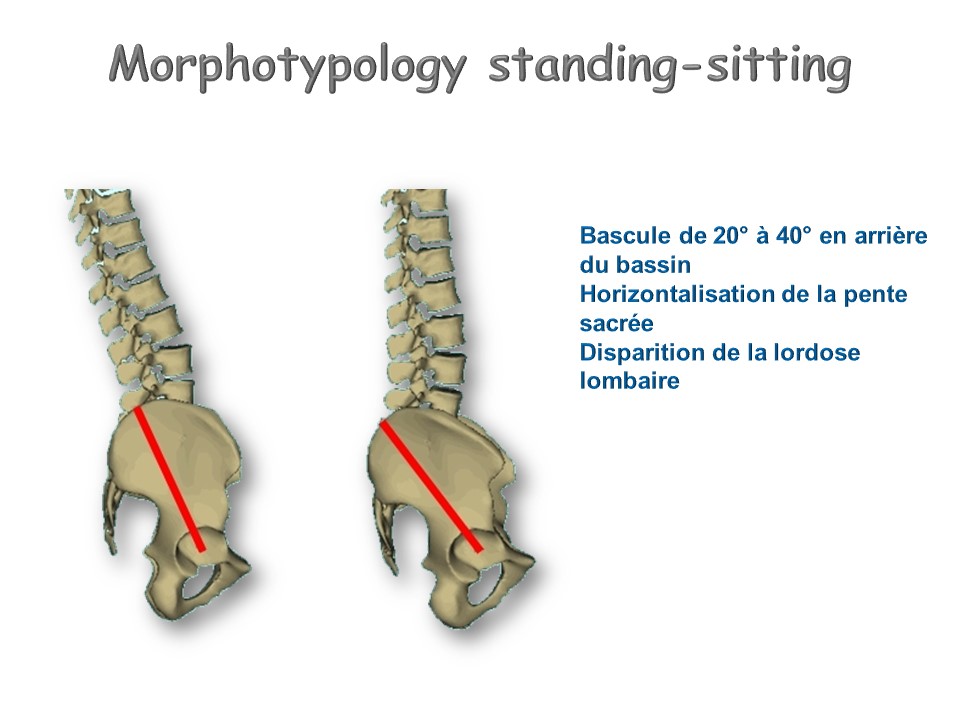 |
The sitting position entails the following changes: Flip backwards of the pelvis from 20 ° to 40 °, Horizontalization of the sacred slope, Decrease of lumbar lordosis. Note that the pelvic tilt is not modified according to the pelvic version. This results for extreme cases, a maladjustment requiring a change in the sitting position.
|
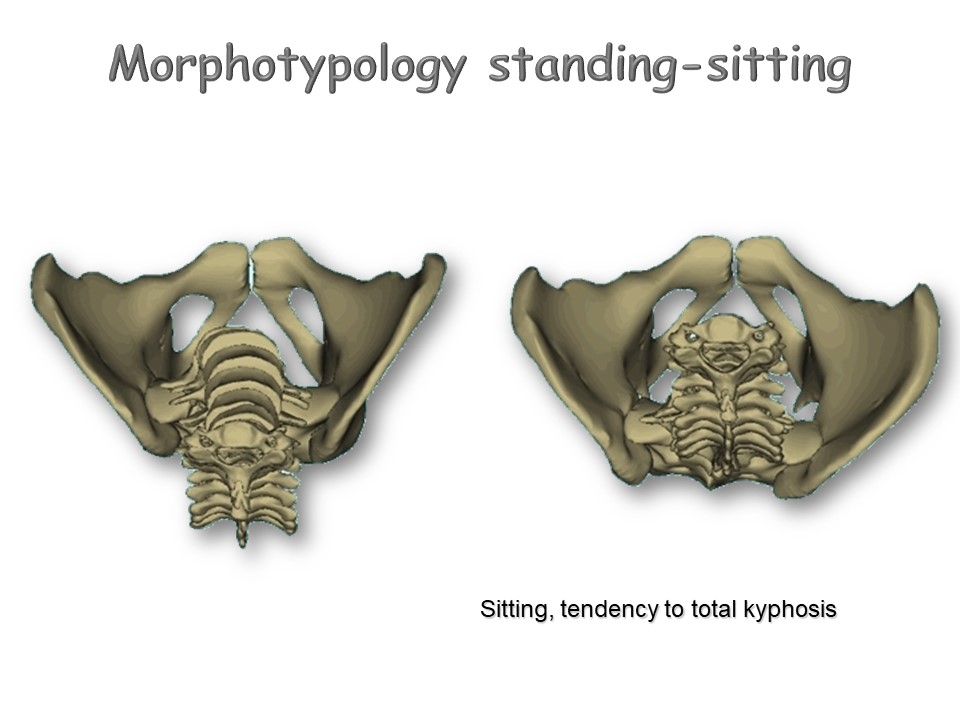 |
The modifications do not concern only the lumbar spine. The sitting position is often responsible for thoracic hyperkyphosis.
|
 |
The adaptation of the workstation begins with the first physiotherapy exercises in the nineteenth century and the multiplication of chairs of different designs.
|
 |
At the beginning of the 20th century, height-adjustable chairs appear.
|
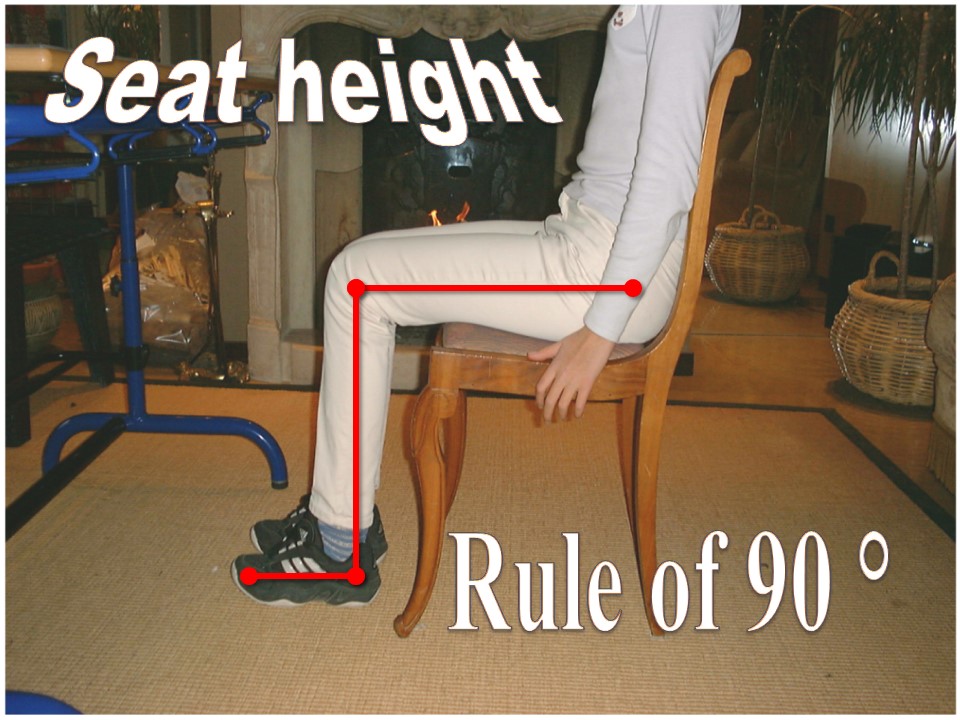 |
At the same time in Germany, Staffel defined the 90 ° rule. Feet, legs and thighs must form a 90 ° angle. This position defines the height of the seat according to the patient.
|
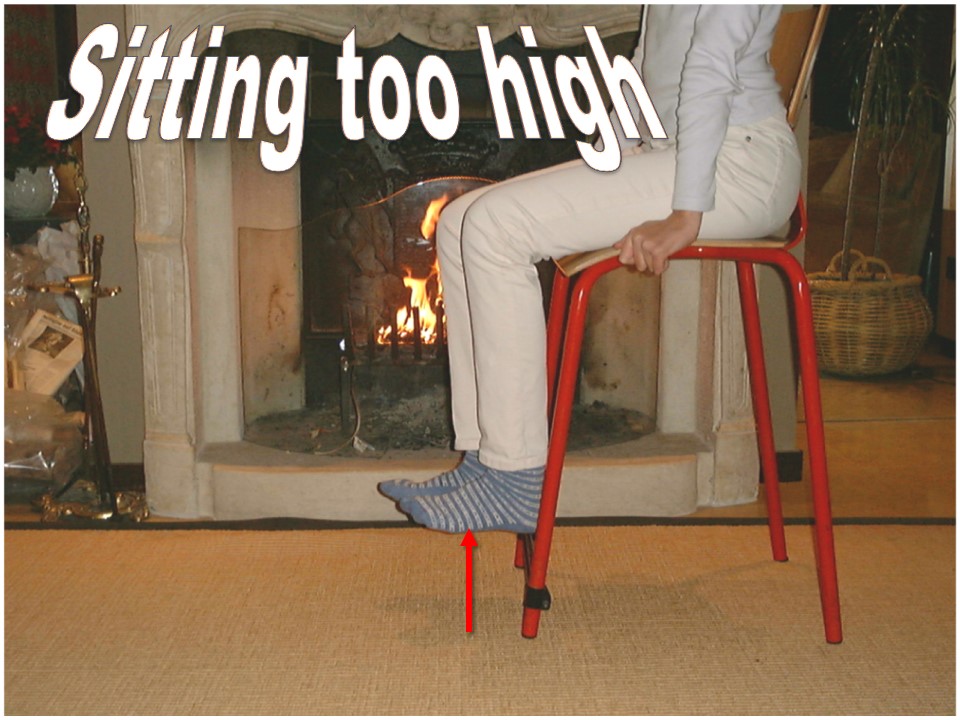 |
Here the seat is too high, type bar chair. The thighs tend to lean forward and the feet do not touch the ground. The disadvantage can be compensated by a crossbar fixed on the 2 front feet of the chair. Lumbar hyperlordosis is excessive.
|
 |
Here the seat is too low. Knees and ankles are in extension. Lumbar kyphosis is excessive.
|
 |
In this position, the knee may also be hyperflexion, which can cause circulatory problems. Lumbar kyphosis is identical.
|
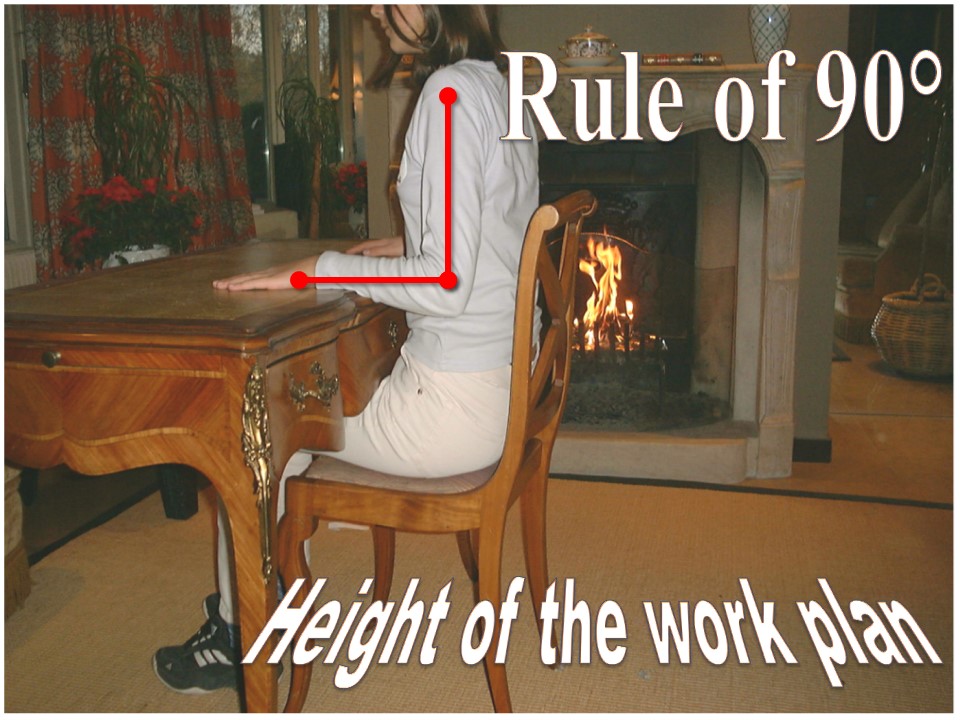 |
Once determined the height of the seat, it remains to determine the height of the work plan. The 90 ° rule also applies to the upper limbs. Arms and forearms are at 90 °.
|
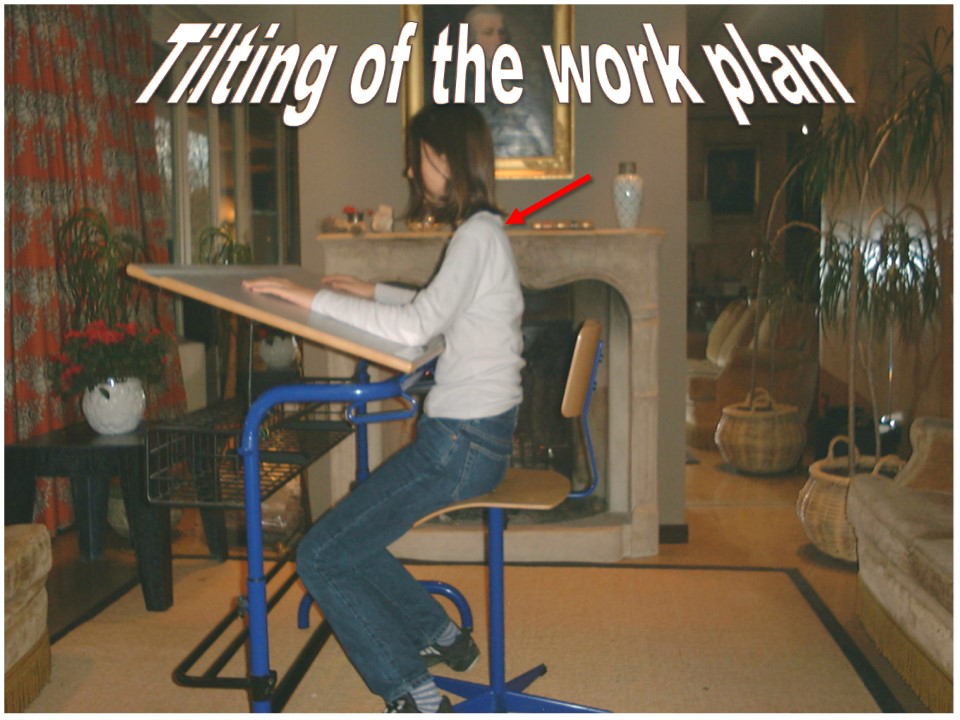 |
Tilting of the worktop is useful for high cervico-thoracic kyphosis. This position is frequently used for industrial drawings and architectural plans.
|
 |
The inclination of the worktop was indispensable for writing with a pen and an inkwell. The use of the bench was the most frequent and intended to stabilize children. The transition to the horizontal worktop is related to the use of the ballpoint pen which worked better in horizontal position. But, some modern designers have reused the old concept.
|
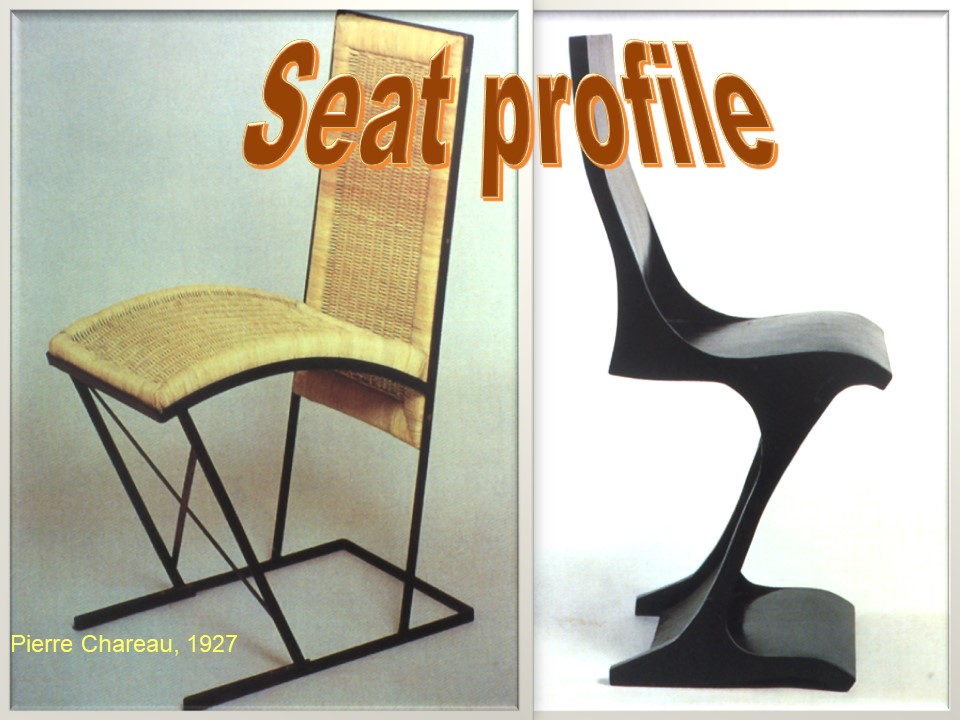 |
The horizontal seat is the most common and the easiest to achieve. The curved seat has the great advantage of improving the posture when one moves from a posture of writing to a posture of listening.
|
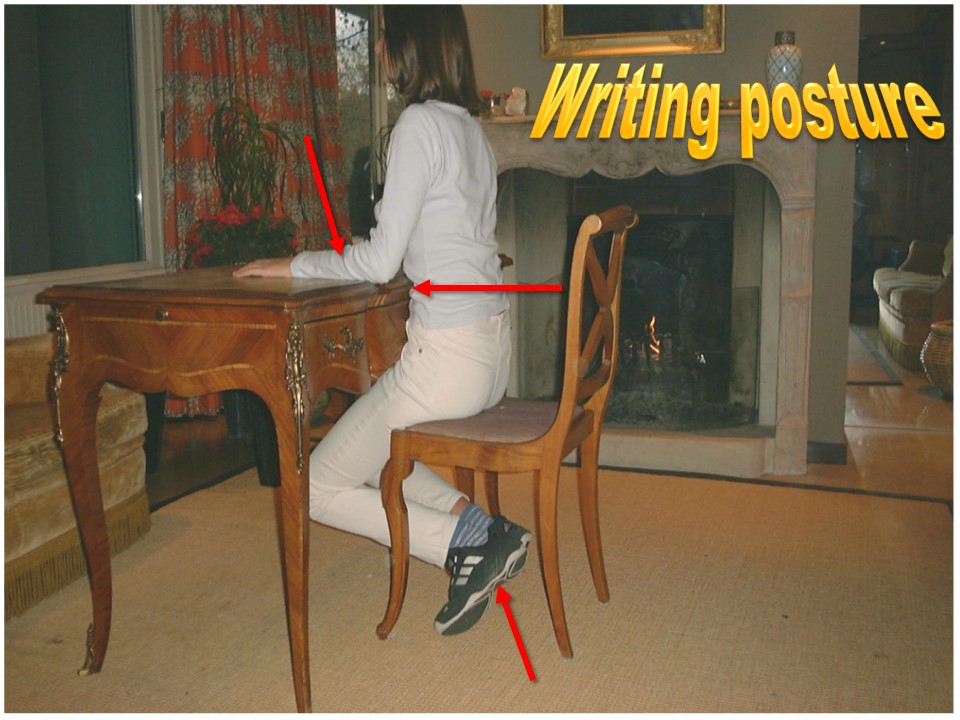 |
In writing posture and from the 90 ° rule, the posture is modified as follows: The feet are below the chair. Thighs are leaning forward, knees to the ground. The buttocks are in front of the seat. The false ribs are in contact with the front edge of the table. The forearms are horizontal on the work surface. This posture is the standard position for all deviations of the spine.
|
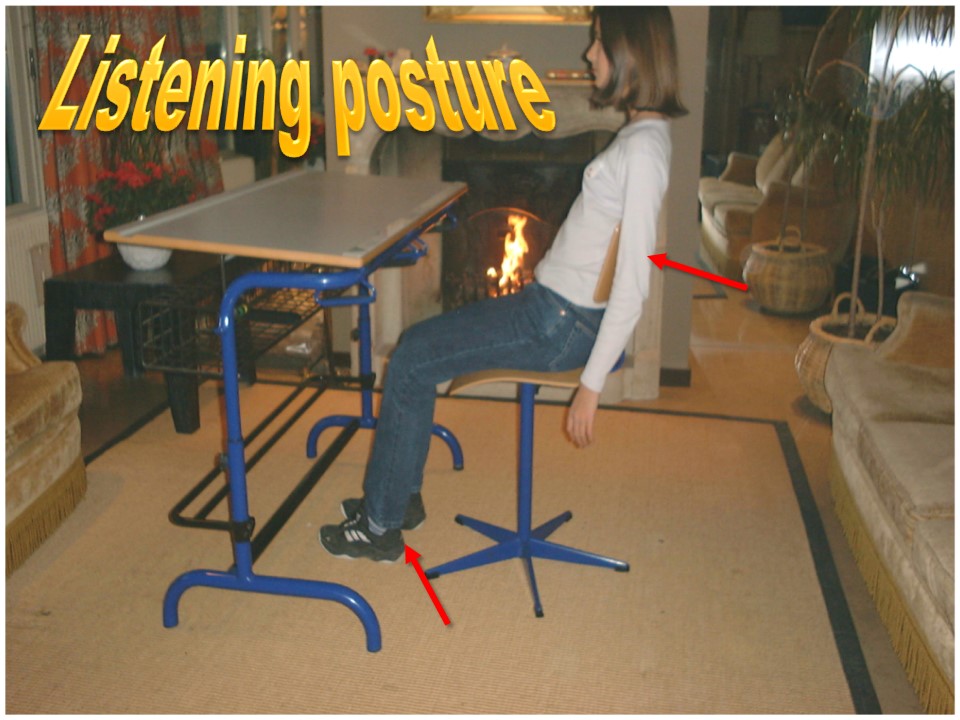 |
The listening position is close to that of the 90 ° rule. the spine is in contact with the back of the chair. Hips, knees and ankles are slightly extended.
|
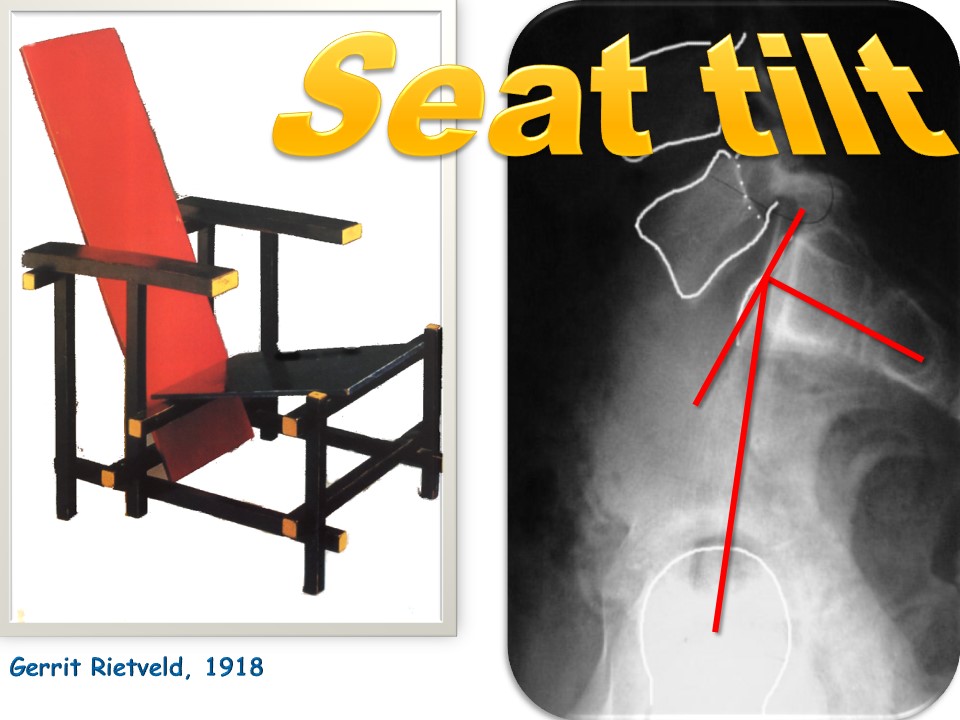 |
When the sacral base is very tilted on the horizontal, as often in spondylolisthesis, there remains a tilt and lordosis when sitting. Indeed, the tilting of the sacral base is limited to 40 ° C maximum between standing and sitting position. Under these conditions, this defect can be compensated by tilting back the seat or using a triangular cushion on a normal seat.
|
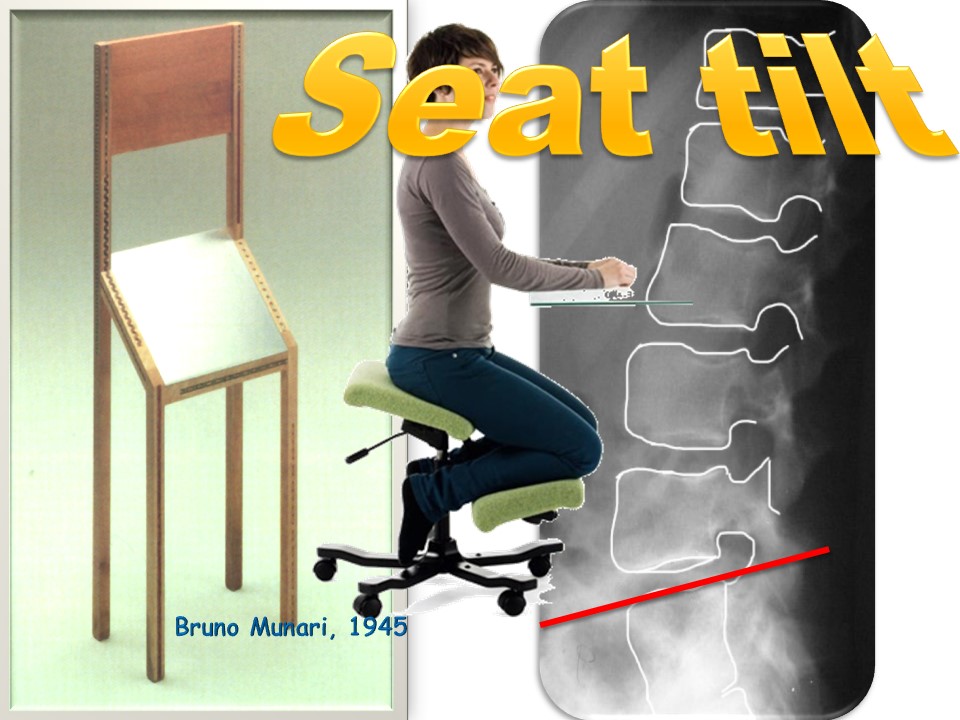 |
Conversely, when the sacral base is too horizontal, it tilts back in sitting position, which causes lumbar kyphosis. The forward inclination of the seat compensates for the defect. The problem is the risk of slippage that will be compensated by a support for the knees. It is the ergonomic kneeling chair.
|
 |
The structure of the seat is important. It must avoid slipping, sweating. It must cushion when the sitting position is prolonged.
|
 |
The shape of the seat gives way to many designs.
|
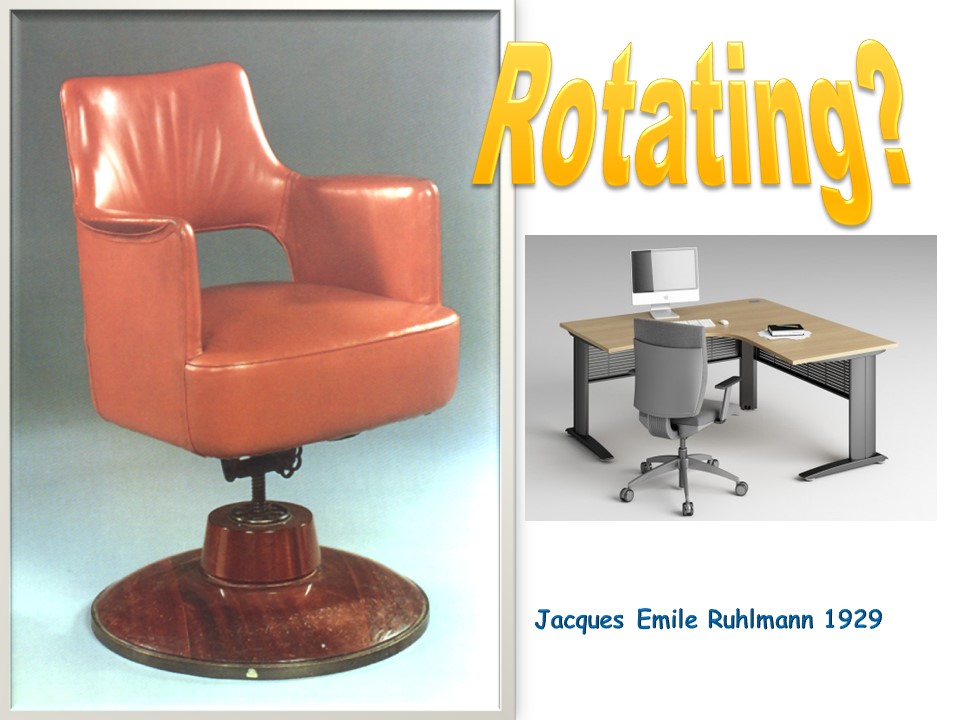 |
The swivel seats are useful when the worktop is L-shaped with 2 planes at 90 °.
|
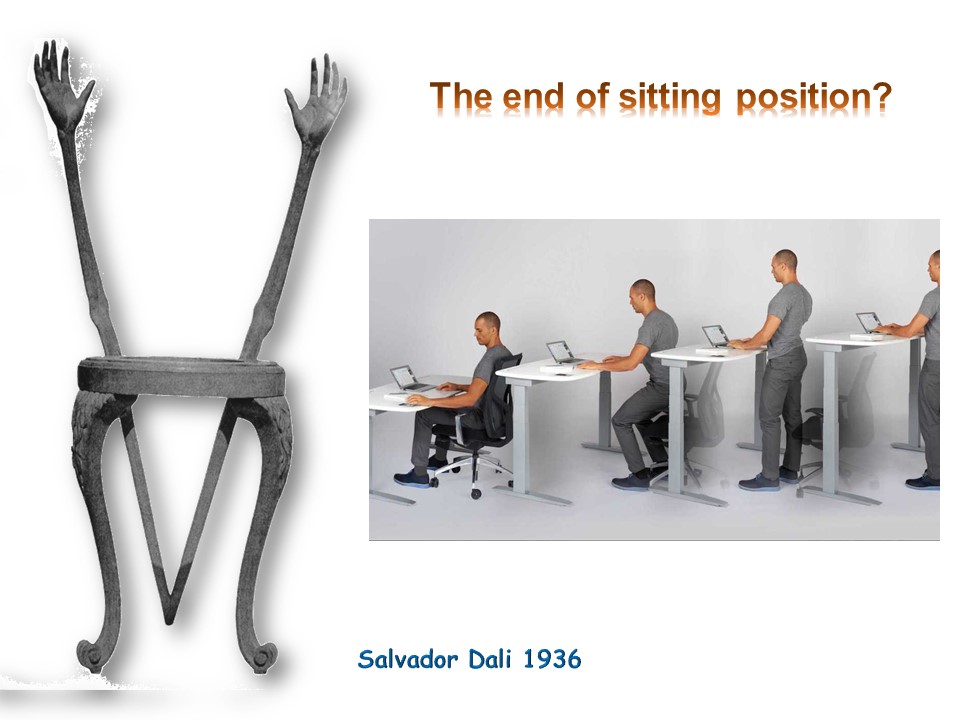 |
Will the sitting position disappear? This seems unlikely, because in standing, mechanical and circulatory constraints in the lower limbs become important. It becomes difficult to work a long time in this posture.
|
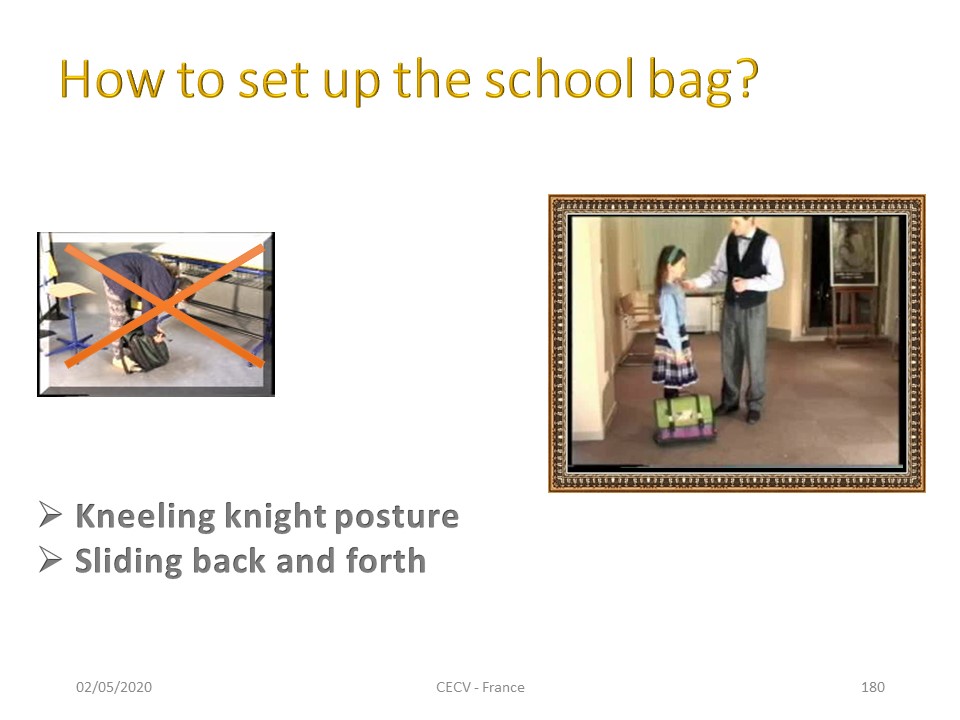 |
During school time physiotherapy can be done with the school bag, which allows to teach the child some rudiments of ergonomics. The school bag represents the knowledge of the child and in Europe the weight of science has no limit. The standing position, trunk bent at 90 ° is to be avoided. Knight's kneeling position is preferable. The child slides the school bag, soil on his knees Then in a second time, fixed on the shoulders through a rotation back and forth.
|
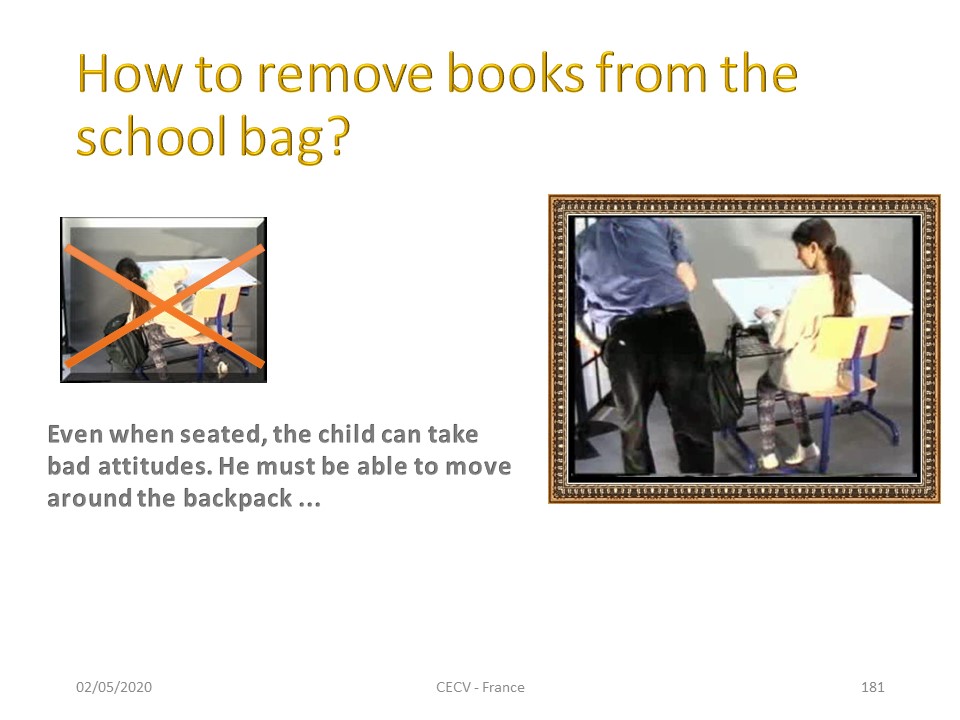 |
The movements associating bending and rotation of the trunk are to be avoided. The same kneeling knight posture will be used to remove the books from the school bag.
|
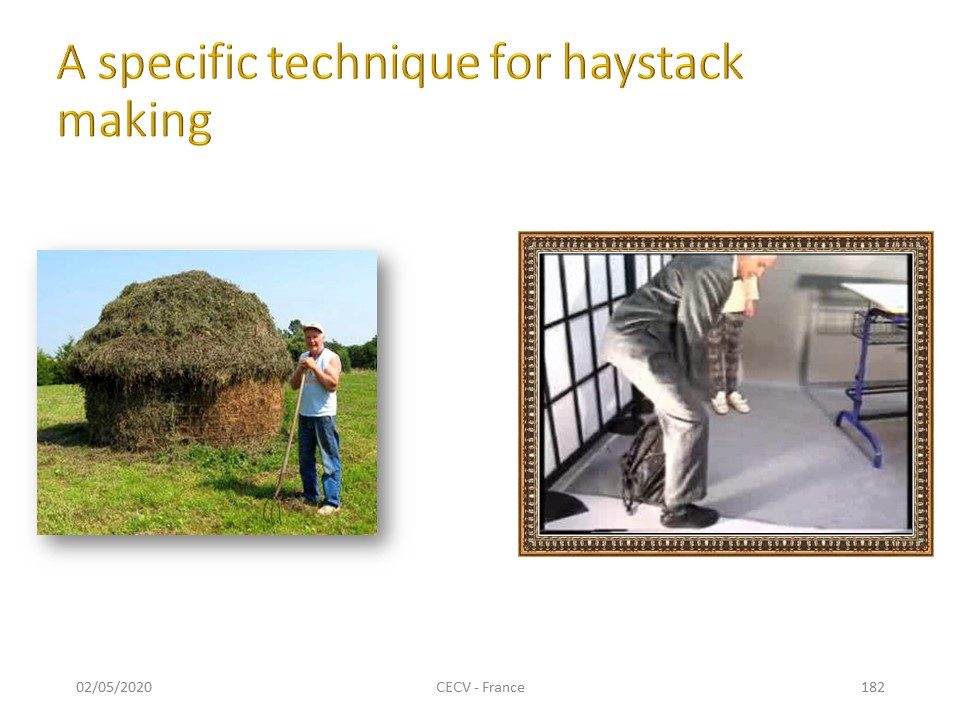 |
Although the majority of farmers used a technique in rotation and extension of the trunk, in France a specific technique of stacking allowed to work only in the sagittal plane of function. The load is placed behind the feet and a balance movement in the sagittal plane facilitates the lifting of the load. The child must choose the starting position to avoid hitting the desk during the pendulum movement and walk forward at the end of the movement.
|
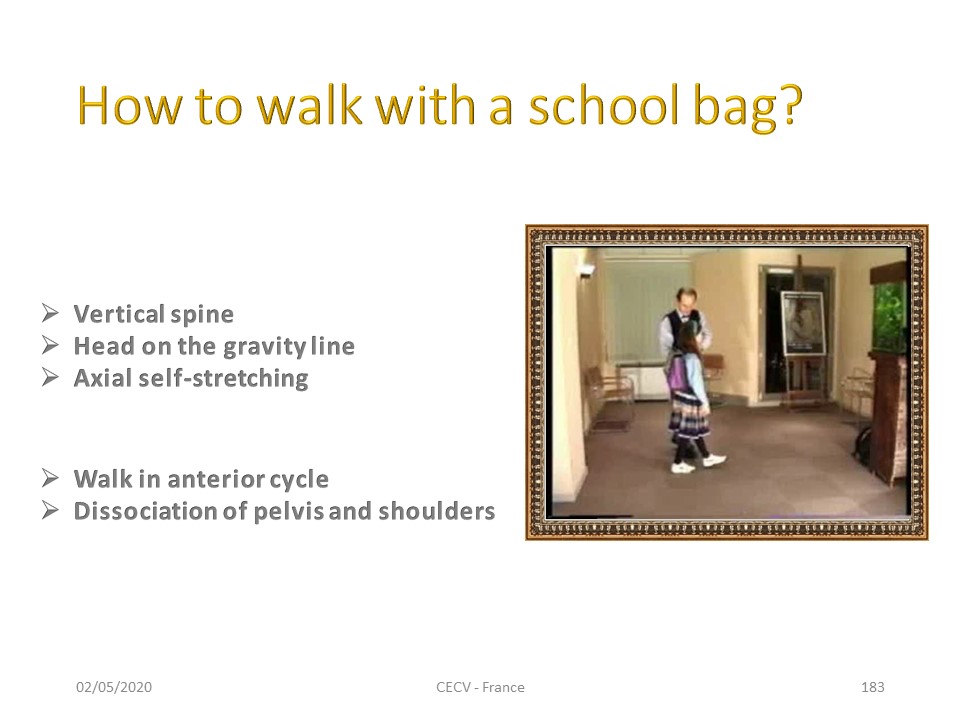 |
The first step is learning the neutral position for a low weight school bag. The spine is vertical with head on the line of gravity. The child performs a translation along the vertical axis as in the “grand porter" of the Lyon method of physiotherapy. When the school bag becomes heavier, the line of gravity tilts backwards and the walking flow is anterior to the line of gravity. This modification in the sagittal plane must be associated with a movement in the horizontal plane peculiar to homo sapiens: it is the dissociation of the pelvis and the shoulders. This movement is automatic with running, which can be done on the spot. The child have to learn how to do it when walking.
|
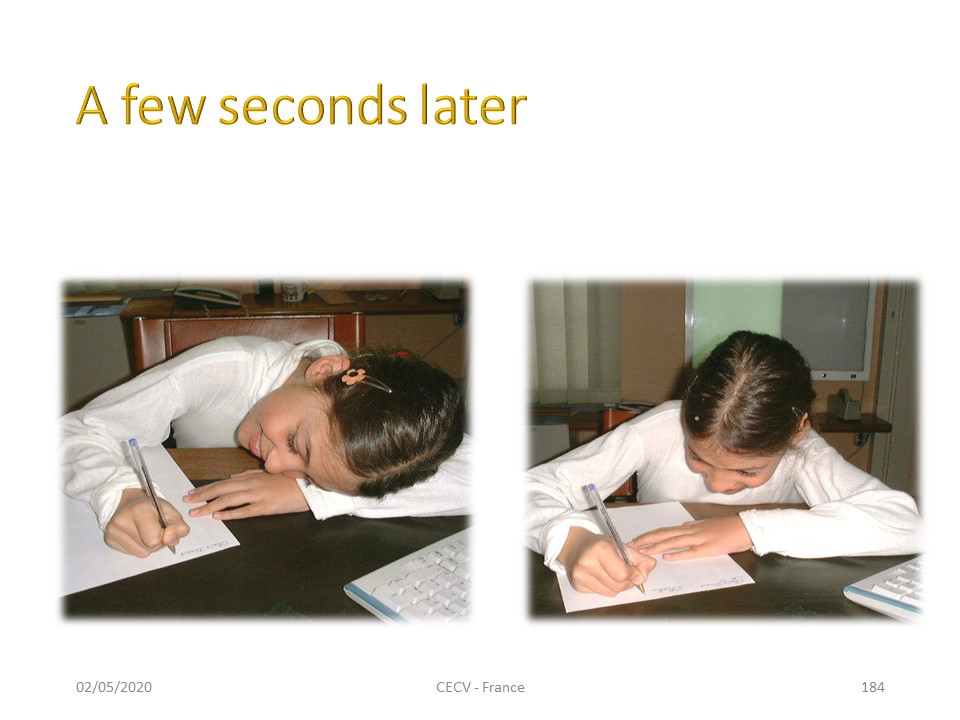 |
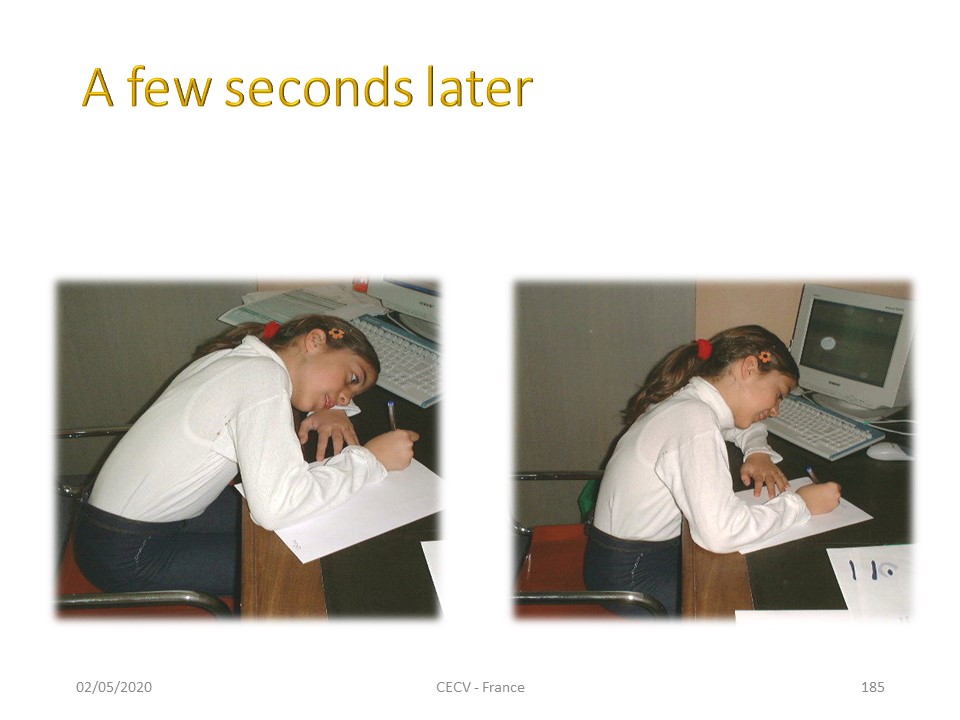
Learning the tridigital pinch to write, improves posture.
|
 |
|
 |

To register for Certification, please contact SSOL

|
")
")
")
")
")