")
")
")
")
")
 |
|
 |
|
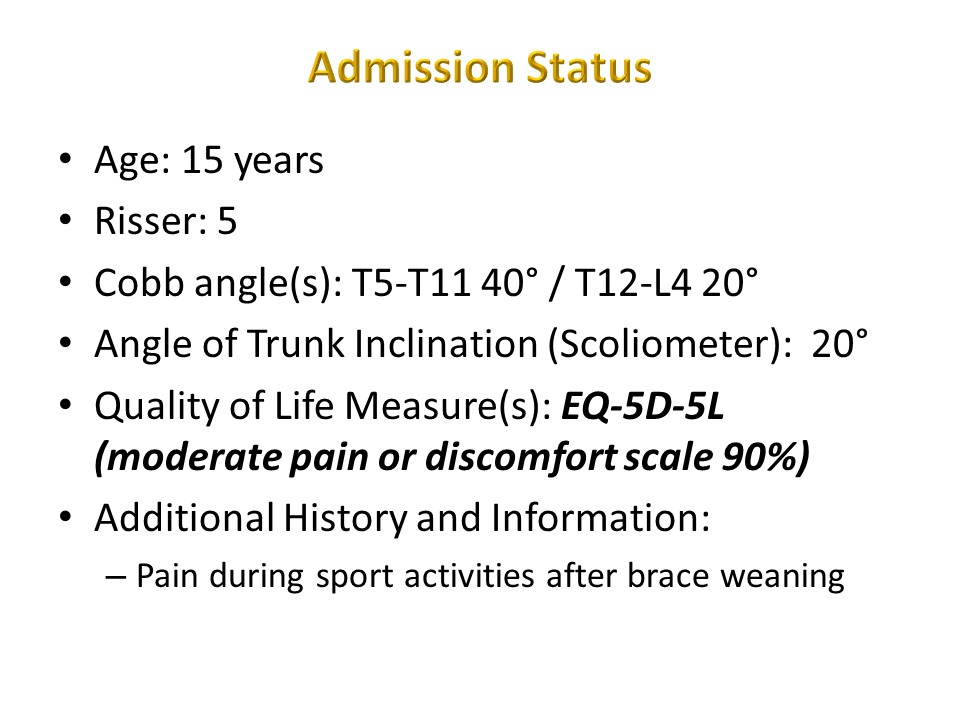 |
In the past 40 years; many educational videos have been produced. We have chosen the most characteristic with exercises carried out by the most competent physiotherapists in the Lyon method: - Jean Noël Voutey, lecturer at Lyon 1 University and who was my physiotherapist at the Clinique du Parc for more than 10 years - Jean François Müller, responsible in France for continuing professional training for physiotherapists (ALISTER), with whom I had the honor of working in the physiotherapy department of Jean Sengler at Mönschberg. The main patient presents a scoliosis with predominantly right thoracic 40 °, painful on exertion, at the end of statural growth. At the parents' request, non-surgical treatment was carried out. |
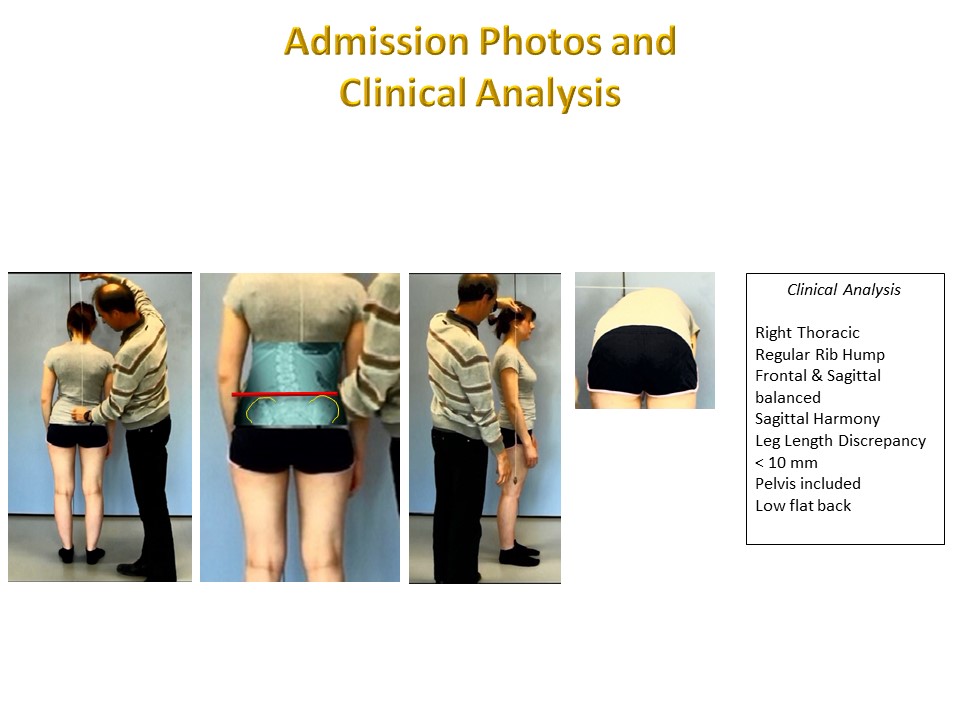 |
For idiopathic scoliosis, the initial clinical assessment is essentially static with plumb line measurements in the sagittal plane and in the frontal plane. A dynamic assessment in search of stiffness both in the spine and in the girdles will complete the static assessment. |
The video shows us the details of the traditional plumb line clinical examination with, in the sagittal plane, measurement of the lumbar lordosis arrow, of the C7 lordosis arrow. In the frontal plane, the occipital axis is balanced. At the pelvis, the imbalance is appreciated at the level of the iliac crests: here minus 10 mm on the right. The plumb line rib hump during the Adams test. At the thoracic level 1mm corresponds approximately to 1 ° of Cobb angle. The hamstrings stiffness is measured by the popliteal angle (full extension is limited and the angulation between the axis of the leg and the vertical is measured). In this same position, a possible asymmetry of rotation of the hips is also measured. At the level of the upper limbs the asymmetry of the pectoralis muscles is appreciated by the elbow-table distance. |
|
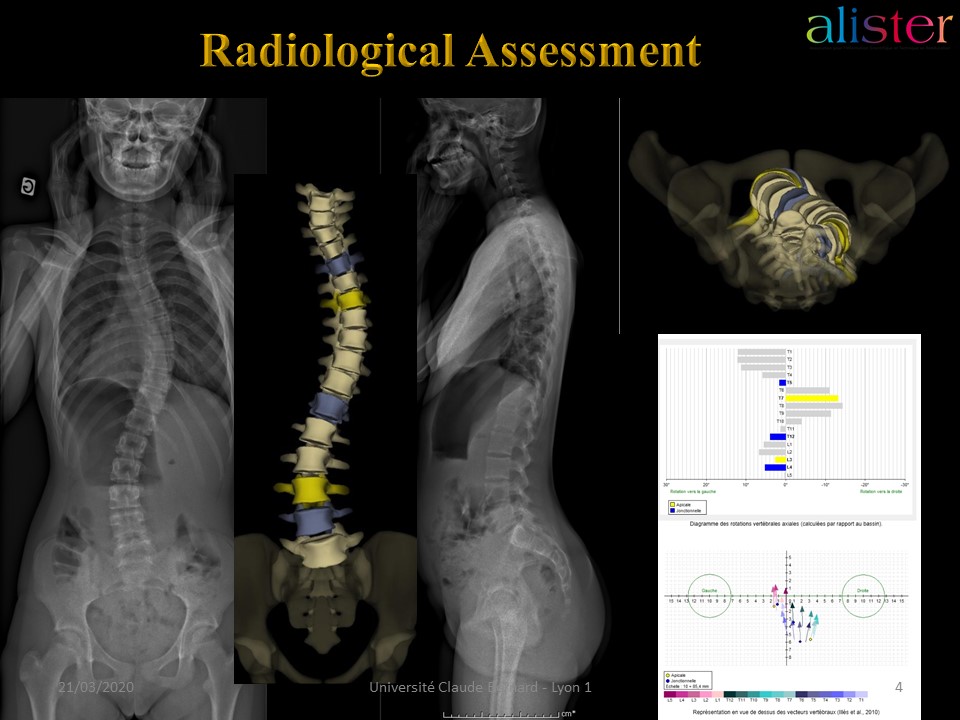 |
The radiological assessment, when done with EOS, allows the visualization of segmental rotations in the horizontal plane. We chose a double curvature scoliosis as a type of description. The 3D representation shows the importance of thoracic rotation. |
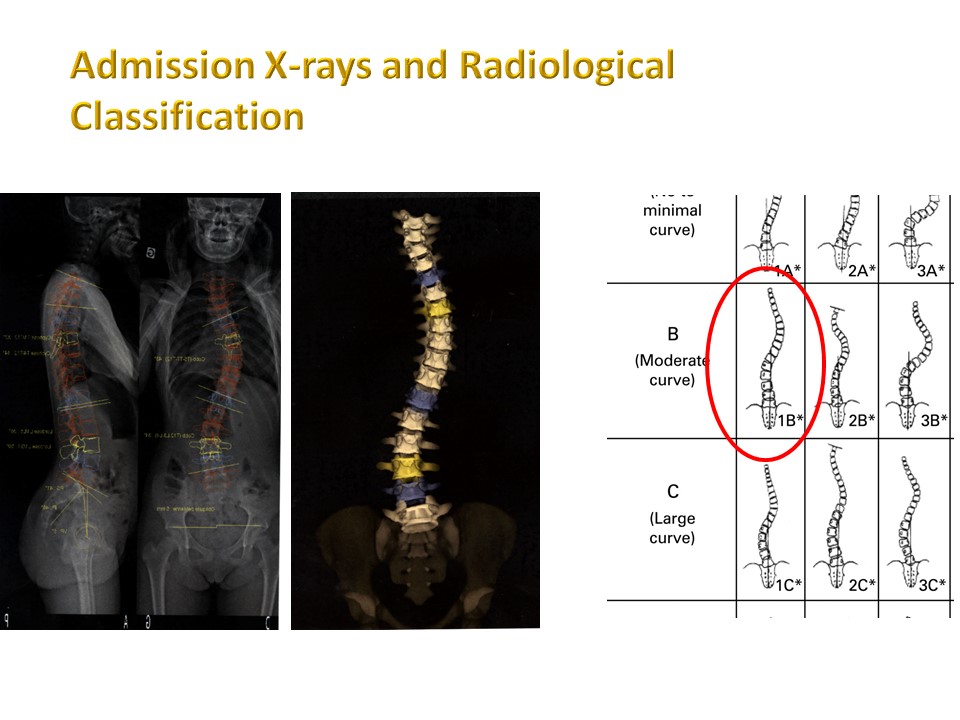 |
There are many radiological classifications. Here we have two curves with a main thoracic curve and a lumbar counter-curve without less rotation. |
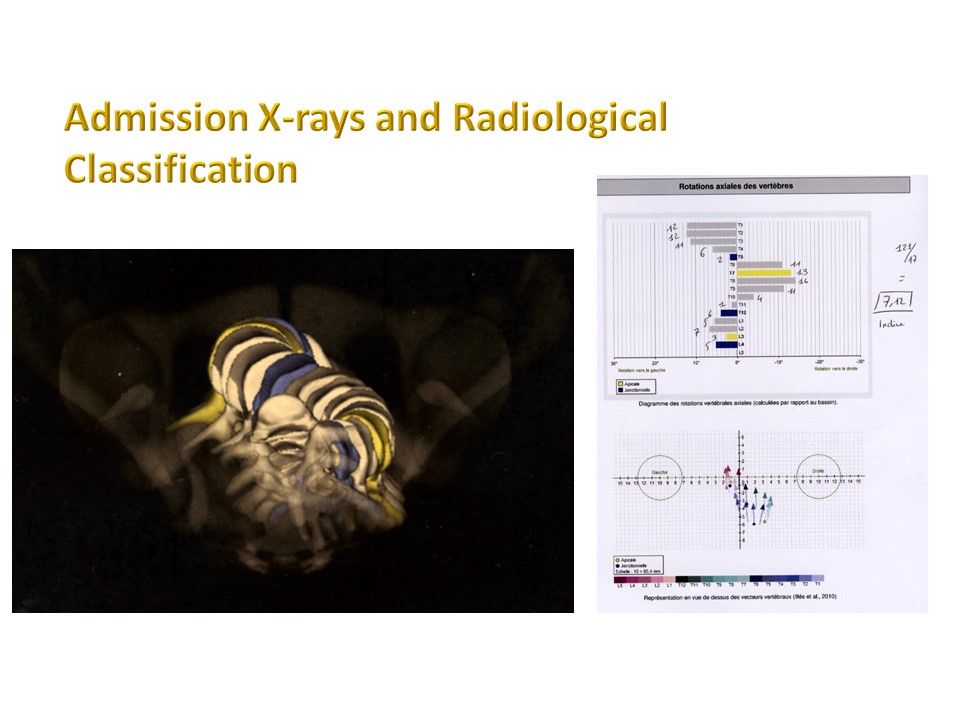 |
The EOS 3D representation confirms the existence of rotations at the counter-curves. On the left, the Da Vinci view and on the right the segmental rotation for each vertebra. |
 |
The initial prescription for the Lyon method includes 30 sessions of 20 'with the physiotherapist, at the rate of one or two sessions per week. A daily repetition of the exercises for 10 'each day is advised.Given the prescription of an ARTbrace, the physiotherapist will insist on the preparation for molding in the corrected position. |
 |
The SOSORT guidelines are very general, but we have specified in the chapter of the Lyon Method principles how to correct in 3D and how to reprogram the sensors of the extra-pyramidal system in the corrected position. At 15 years, even if the final height is acquired, the bone mass has not reached its maximum resistance, which can explain the pain during sport activities and will justify specific indications. |
The first example of typical exercises of the Lyon method is the awareness of postural defects. The child sees the backs of others, but he does not see his own. The first step common to all PSSEs is therefore to show any defects using an orthopaedic mirror, or better using a video, and to explain the vocabulary specific to vertebral deviations. The auto-correction of any defaults will be demonstrated. |
|
 |
|
 |
Charles Gabriel Pravaz, the creator of the Lyon method was not only a doctor, but also an engineer, a pupil of the prestigious polytechnic school of Paris. This explains why he was the inventor of the syringe and why he developed ingenious methods of correcting scoliosis. |
 |
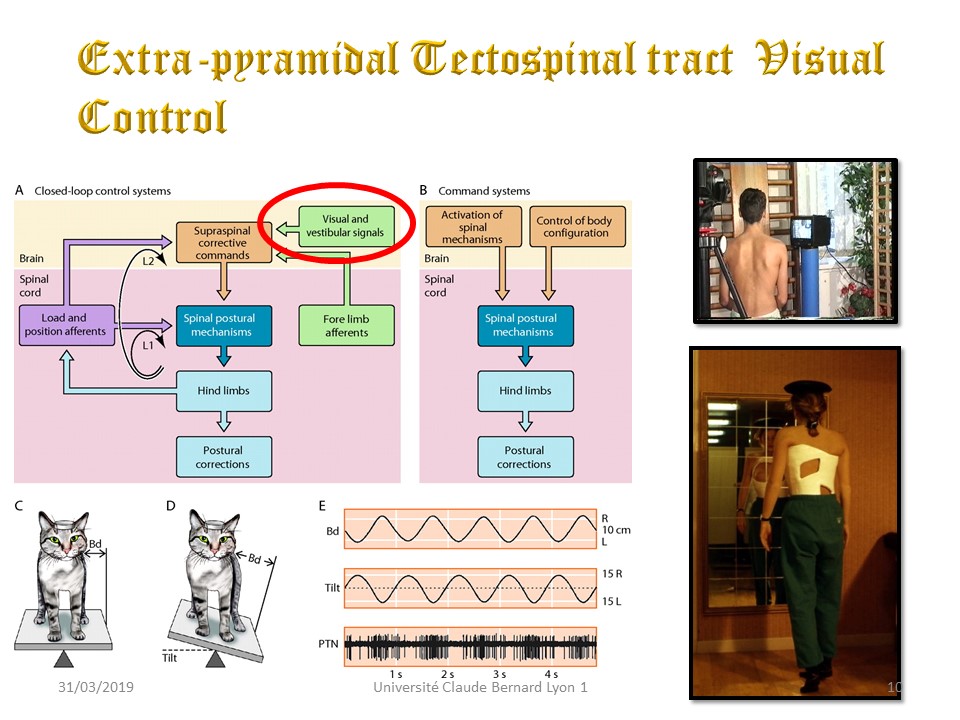
In the tecto-spinal tract, visual information is recorded by the sensory and sensorial integration centers in the parietal and occipital cortex. The information is then transmitted to the motor centers which send a command to the muscles which contract to compensate for the imbalance. Here for example at the quadriceps muscles. The sensorimotor coupling is focused on spatial location. Head movements are recorded at the level of the semicircular canals and are compensated by eye movements. The objective is to keep the visual information allowing anchoring on the environment. The tecto-spinal tract is essential in the recovery reaction after a fall or in sports following a ball like football. |
 |
TNote that the Lyon method uses this tecto-spinal tract in case of cervicalgia for which we prescribe the table-football. |
 |
|
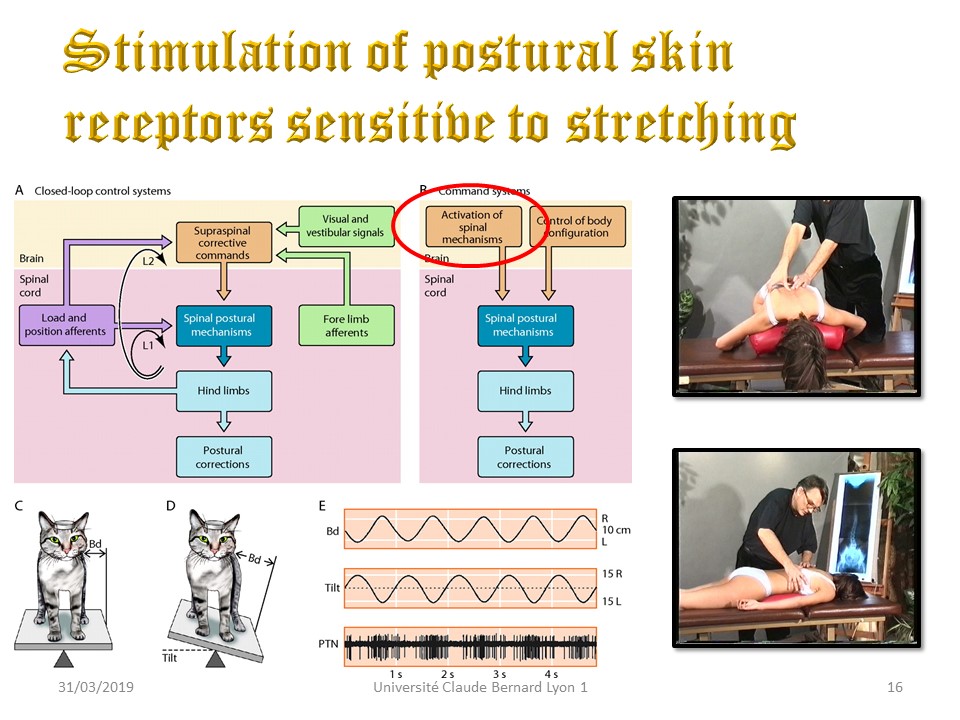
You remember that we have four major positions…The second example of exercise is done in prone. The objective is to stimulate all the sensors of the extrapyramidal system which are sensitive to stretching. The physiotherapist places a cushion under the child's chest to perform this stretch. In this passive axial extension posture, all the facets joints can be mobilized. |
|
In this position, the muscles are stretched into ideal kyphosis. Muscles contain receptors sensitive to stretching. They allow the perception of the length of the muscle that is to say their position, and their variation in length that is to say the movement. The spindles are small fibrous structures, the central part of which is surrounded by a spiral nerve ending. They will code the positions and movements of the muscle and transmit this information to the brain through an afferent fiber. At the joint level, there are also two types of receptors with a different function: Pacini and Ruffini. The Pacini sensor is sensitive to the movement of the joint capsule and ligaments, especially at maximum amplitudes. It is a dynamic or phasic sensor. Ruffini's sensor is more sensitive to position. It allows to know a fixed articular amplitude. It is a static or tonic sensor. The movement corresponds to a change of state. As long as there is movement, the dynamic sensors of Pacini are active. A change of state therefore corresponds to speed information. At the end of the movement, the tonic or static Ruffini sensors code the new position according to the degree of stretching of the muscle, giving amplitude information. |
|
| > | A variant in the event of significant flat back or pain is the use of the fetal kneeling position with heels-buttocks in contact. The upper limbs in the relaxed position accentuate the upper thoracic kyphosis. A cushion is placed under the chest, which allows stretching of the deep back line. |
 |
It is in this position that all ligamental and transverso-costal joints sensors will be stimulated by soft mobilization. |
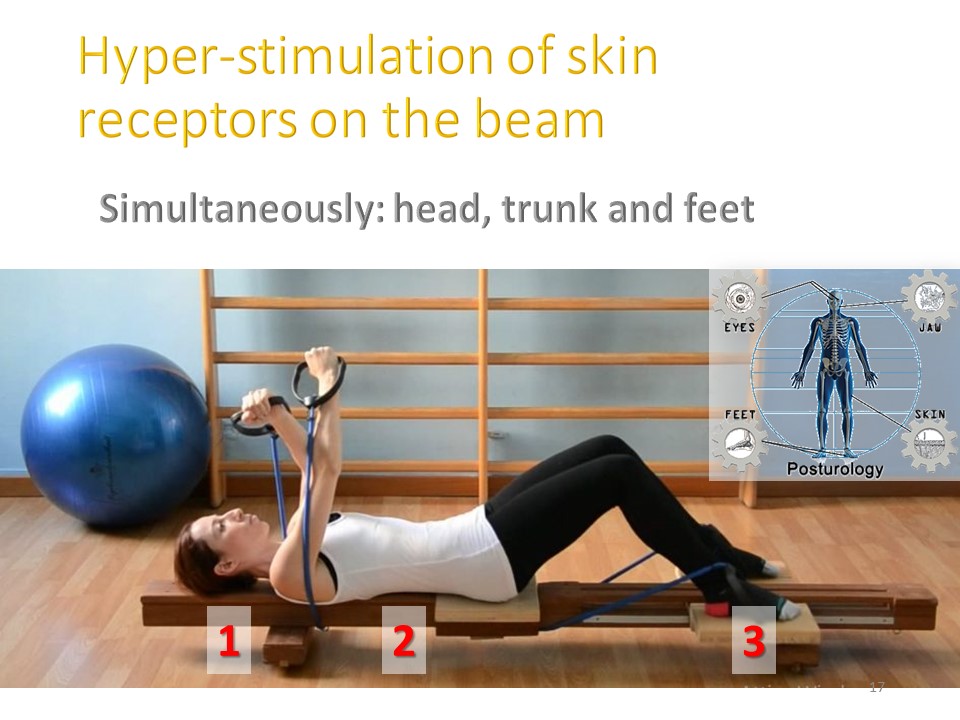 |
In ARTbrace there is no longer any skin contact at the level of the vertebral spinous line. Decubitus on beam allows to restore these contacts and to compensate for the absence of stimulation in brace. |
 |
|
The third type of exercise is performed in procubitus, and isostatic kyphosis in the sagittal plane. A corrective side bending can be performed in this position. If the cushion is placed under the left hemi-thorax, derotation by concavity is facilitated. |
|
 |
|
After the overall longitudinal stretching exercises, segmental mobilization exercises can be carried out in the areas of stiffness, ie at the apex of scoliosis. A shearing movement is made between the convex joint facet and the underlying concave joint facet. |
|
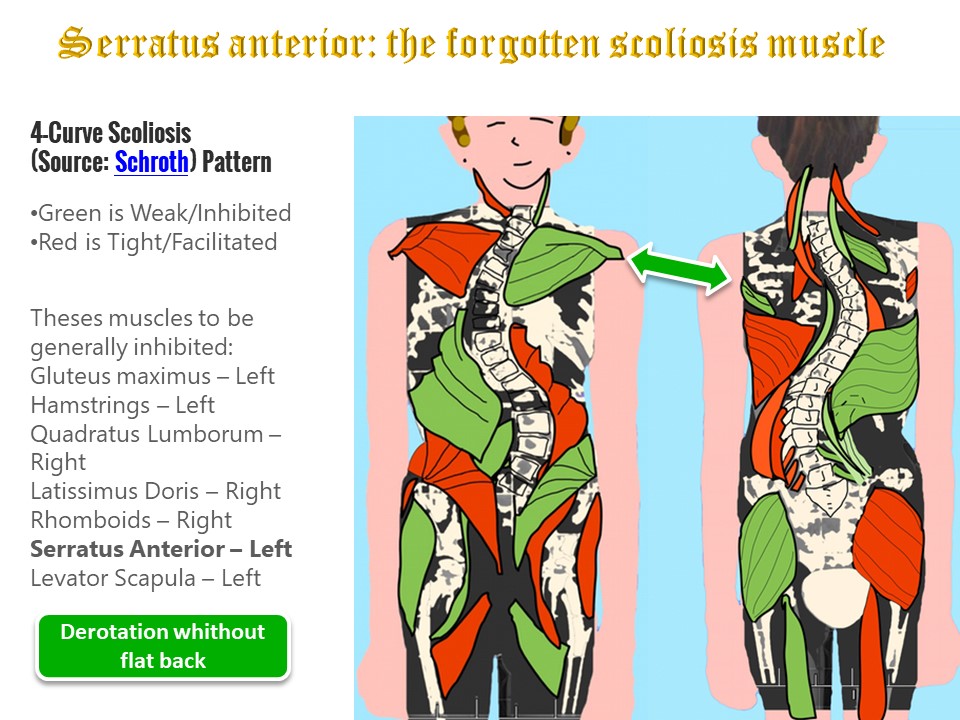 |
In scoliosis, the fasciae are asymmetrical without any evidence of muscle weak or strong. There is neither facilitation nor inhibition. The Lyon method aims to readjust tensions (tensegrity) by stretching the shortest fasciae. For example, one of the shortened muscles is the concave serratus magnus. |
The concave serratus magnus is shortened, it will be stretched by pressing the scapula against the table. The load is exerted on the elbow in the axis of the arm. The active contraction of the muscle by the technique of hold relax also allows derotation by concavity. Convexity is only a fixed point. The child can also be teached to perform the exercises alone in self-passive. The big advantage of the derotation by the concavity is that it is associated with the thoracic kyphosis, contrary to the classic derotation by the convexity which is associated with the flat back. |
|
 |
|
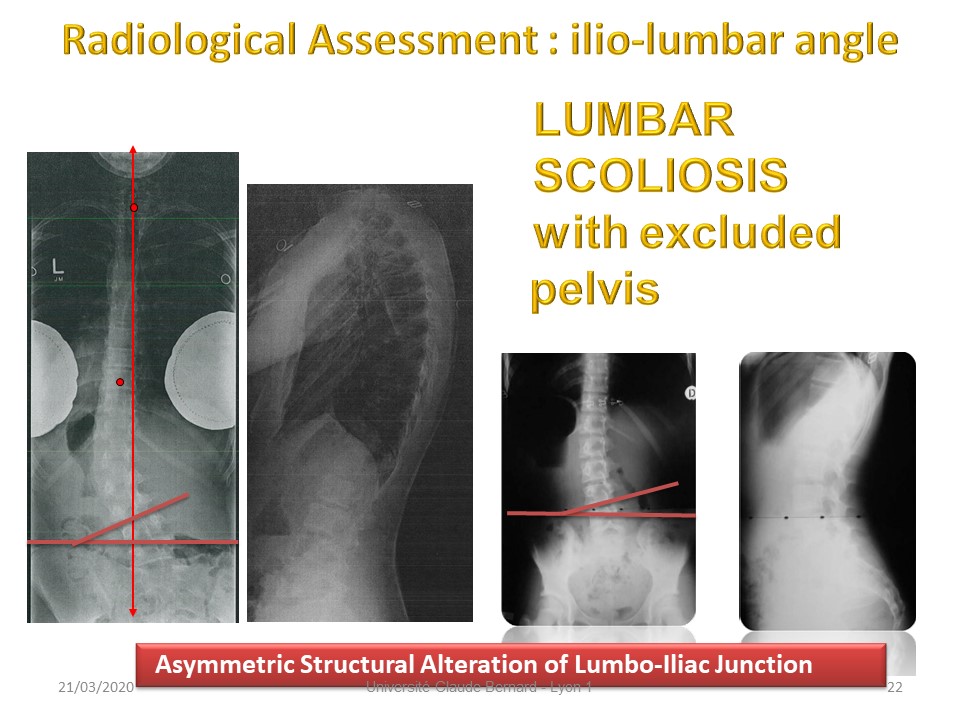 |
We have seen that since the Rhesus monkey, the ilio-lumbar muscles have been transformed into ligaments. It is an asymmetry of the ilio-lumbar ligaments that can be measured by the angle formed by a tangent to the upper plate of L4 and the bi iliac crest line . The pelvis is then excluded, that is to say it is no longer perpendicular to the last lumbar vertebrae. |
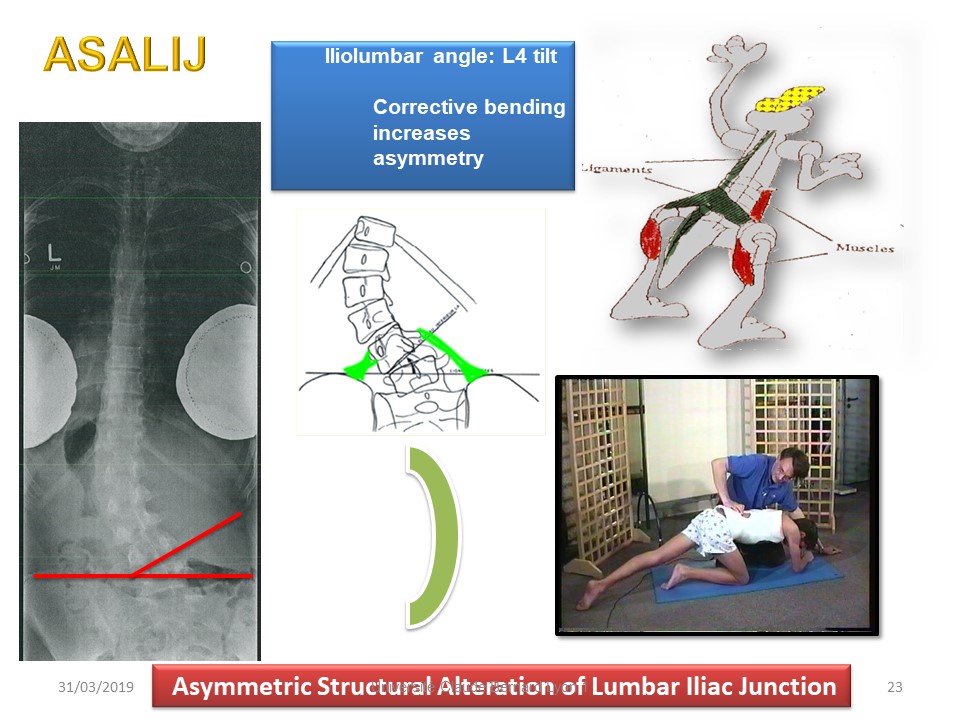 |
This "Asymmetric Structural Alteration of lumbar-Iliac Junction" is primary and lumbar scoliosis is secondary. It is more a symptomatic scoliosis than an idiopathic scoliosis. The characteristic signs are the radiological tilt of L4 and the clinical imbalance of the occipital axis. |
 |
With the unbalanced occipital axis, the pelvis is often rotating. In physiotherapy, the problem is no longer the correction of lumbar scoliosis, but the ligament readjustment of tensions with stretching of the convex transverse-iliac ligament. As always in the Lyon method, the initial in-brace “total time” will facilitate plastic deformation. |
In the frontal plane, the ilio-lumbar angle can be opened laterally on the side of the concavity and initially the physiotherapist uses the lever arm of the lower limb in the axis of the trunk to lower the convex iliac crest, seeking to include the pelvis in the lumbar scoliosis. Manually all the convex structures are stretched. Then the stretch can be completed by derotation of the pelvis in a horizontal plane. The lower limb is positioned 90 ° to the trunk towards the convexity while the trunk rotates 90 ° towards the concavity so that the chest rests on the examination table. |
|
The ilio-lumbar angle can also be opened in a half-seated position on the concave ischium. The physiotherapist asks the patient to flex the convex lower limb to lower the convex iliac crest. In this position, it is easy to manually carry out a corrective shift from the convexity to the concavity which moves the transverse insertion of L4 toward the gravity line and stretches the ligament. One can use the technique of hold relax by asking the patient for a contraction of the convex muscles (quadratus lumborum and psoas). |
|
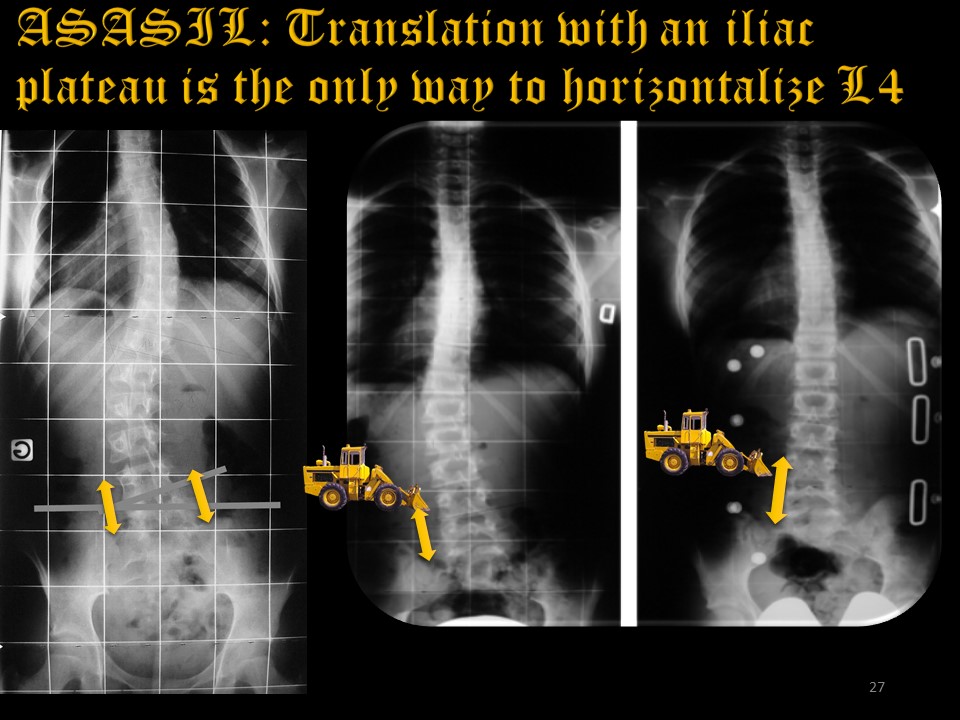 |
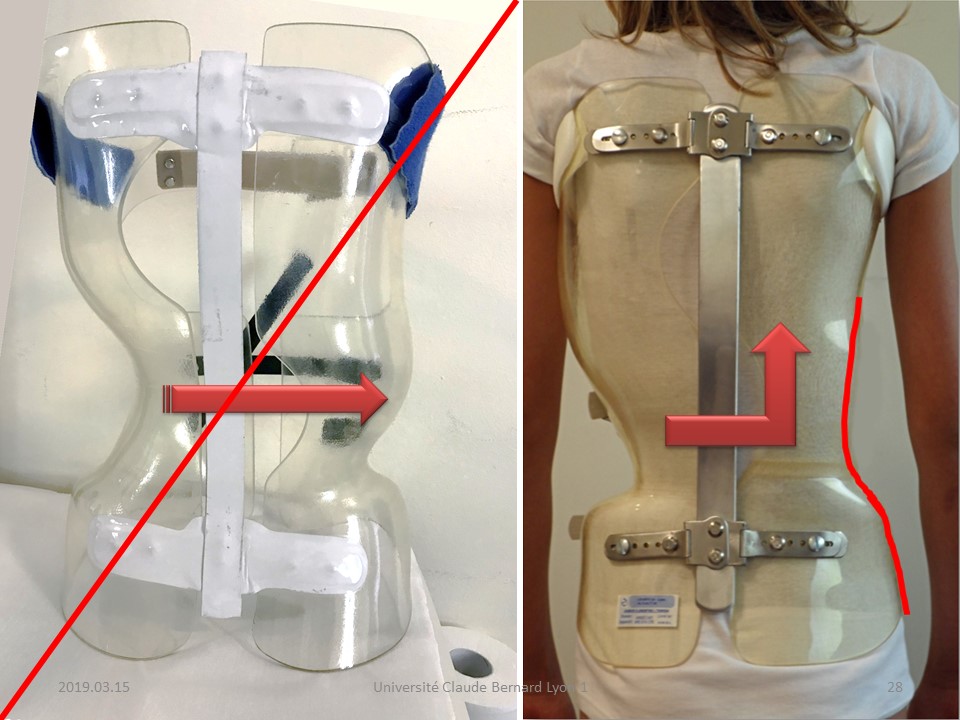
This last exercise in the half-seated position is an excellent preparation for ARTbrace molding No. 2 of the lumbar region. Lumbopelvic ligament asymmetry was described by du Peloux 45 years ago. It was the basis for the Lyon short brace, then the GTB brace. The only way to stretch the ligament is to push the vertebral body of L4 towards the midline, that is to say to translate along the transverse axis or "shift". This is usually enough to straighten the entire lumbar spine. |
 |
In these cases of Asymmetric Structural Alteration of Lumbar Iliac Junction. The expansion in the concavity is useless, on the contrary we must create a concave wall to propel the frontal translation forces upwards. In case of double curve, the concave wall facilitates the corrective bending of the thoracic convexity. |
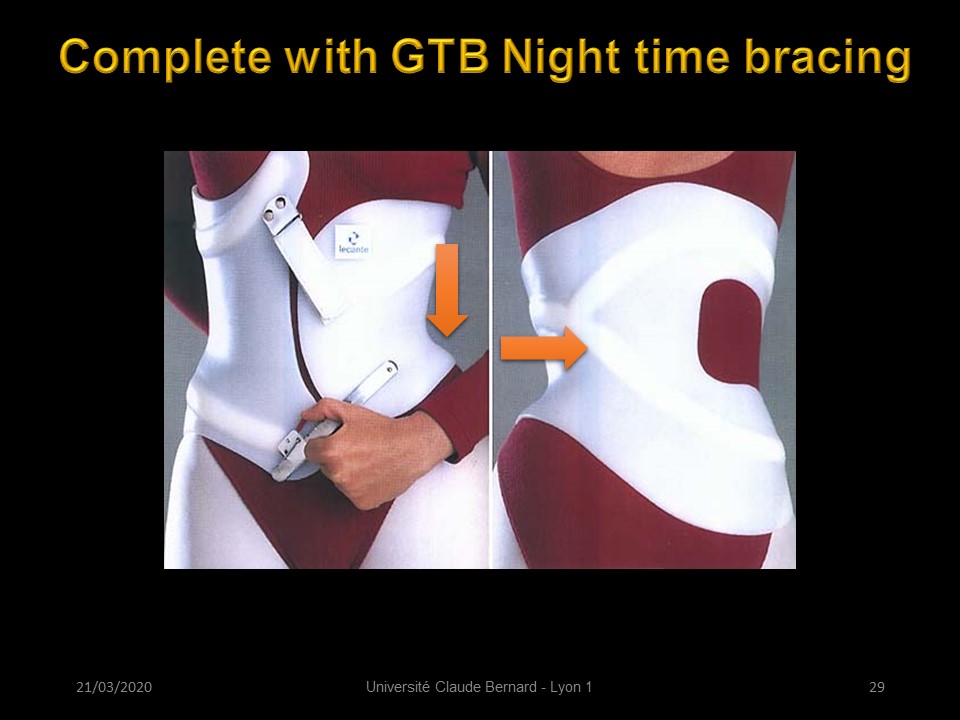 |
The short GTB brace completes the manual translation of the physiotherapist. It best performs plastic deformation with restoration of the tensegrity at the base of the spine. |
 |
The short GTB brace completes the manual translation of the physiotherapist. It best performs plastic deformation with restoration of the tensegrity at the base of the spine. |
In case of structural lumbar scoliosis, the basic exercise combines manual shift with the right upper limb from the left convexity towards the concavity and an isometric contraction of the concave psoas by locking the knee with the left hand, which facilitates the realignment of the lumbar vertebrae on the line of gravity. |
|
TAnatomical reminder of the ilio-psoas. |
|
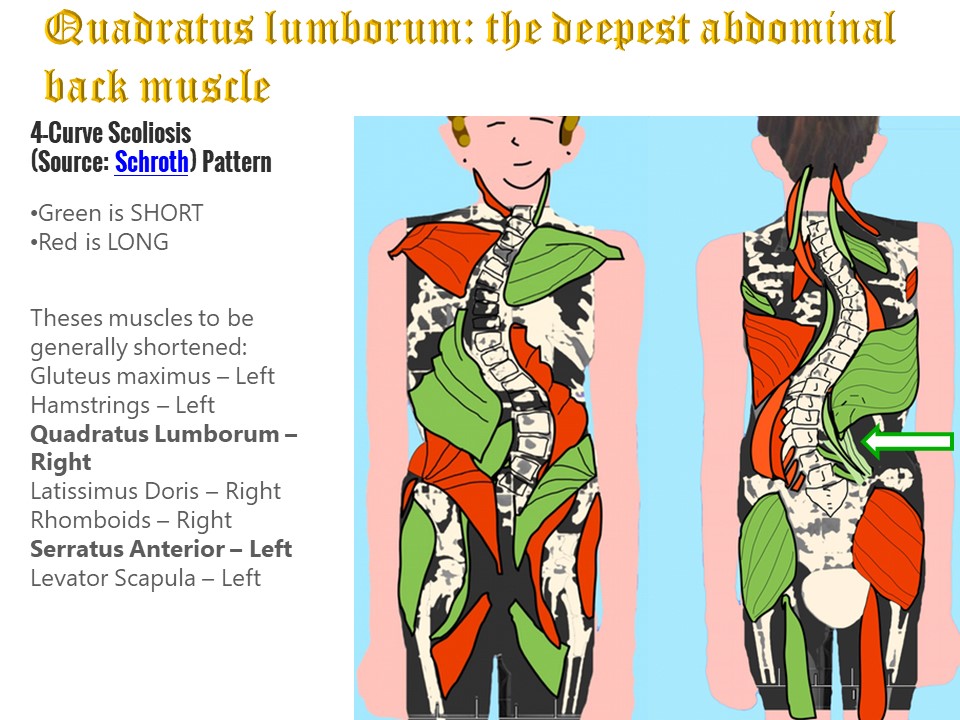 |
In the lumbar concavity, the quadratus lumborum is shortened like the string of an arc. |
The concave quadratus lumborum can be strengthened in lateral decubitus on the lumbar convexity. The convex lower limb is flexed with 90 ° angle to stabilize position. The concave lower limb is adducted into the void and the latissimus dorsi is stabilized by positioning the concave hand on the head. The technique of hold relax is used by requesting an isometric contraction of the concave side chain and more particularly of the lumborum quadratus. The passive extension is increased during the relaxation phase. |
|
Anatomical Reminder of quadratus lumborum and transversus abdominalis |
|
 |
Once the ilio-lumbar ligaments are symmetrized, the correction is done in blocks with either a single thoraco-lumbar curvature or a double curvature as in the case we present. |
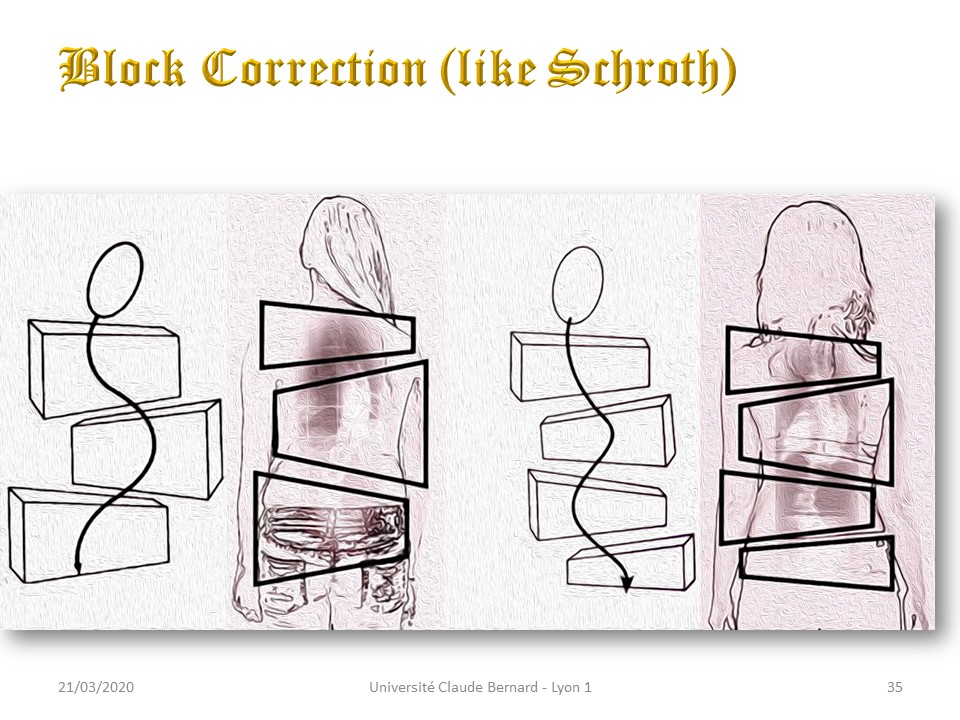 |
Once the ilio-lumbar ligaments are symmetrized, the correction is done in blocks with either a single thoraco-lumbar curvature or a double curvature as in the case we present. |
 |
The characteristic of the Lyon method is the symmetry so that the head is always in the axis of the lower limbs. Indeed vestibular sensors are fundamental in the extra-pyramidal system. The correction is done in the sagittal and frontal planes, derotation is the consequence of coupled movements. |
The pelvic version and the lordosis can be adjusted while seated on a tilting platform which also stimulates kinesthetic sensors. The sitting position relaxes the pelvi-trochanteric muscles. The child becomes aware of the pelvic anteversion - lordosis and pelvic retroversion - delordosis coupling. The definite setting will be adjusted according to the sagittalometer data, therefore adapted to each lumbopelvic incidence. |
|
Physiological basis of pelvic version adjustment. Any movement of the pelvis changes the 3 curvatures. These modifications allow to find a new isostatic balance of the trunk. |
|
| In addition to functional electrical stimulation tests, conventional treatments are becoming more relevant. In London, Min Mehta performs the serial casting for infantile scoliosis. |
|
After the restoration of the isostatic balance in the sagittal plane, the corrections in the frontal plane will be carried out according to the principles well defined by Min Mehta, ie lumbar translation, from the convexity to the concavity with if possible a slight extension by raising the concave shoulder without losing isokinetic lordosis. In general in the concavity, the sub-axillary zone is on the same vertical as the trochanter. |
|
 |
Once the ilio-lumbar ligaments are symmetrized, the correction is done in blocks with either a single thoraco-lumbar curvature or a double curvature as in the case we present. |
In the thoracic region, the exercises can also be performed in a seated position. Here the kyphosis in isostatic equilibrium is controlled by the level stick. The patient performs a corrective bending, by rotation on the sagittal axis of the vertebral body. The hold relax technique can be used. The head and the vestibular system remain fixed. |
|
An active-passive variant is performed manually by the physiotherapist. In this isostatic kyphotic posture, the bending automatically causes a detorsion. This detorsion can be completed manually at the convexity, as there is no risk of increasing the flat back in this position. In a second step, the bending will be done actively by taking support below the apex of the convexity and by stretching the concave latissimus dorsi with the concave hand on the head. |
|
Third example of a 3D thoracic correction exercise while seated. The thoracic spine is positioned in isostatic kyphosis. The right upper limb fixes the convexity, while the concave upper limb pulls the fascia of the concave latissimus dorsi, in this case with detorsion by the concavity. In this posture, the lumbar lordosis must also be maintained. |
|
 |
|
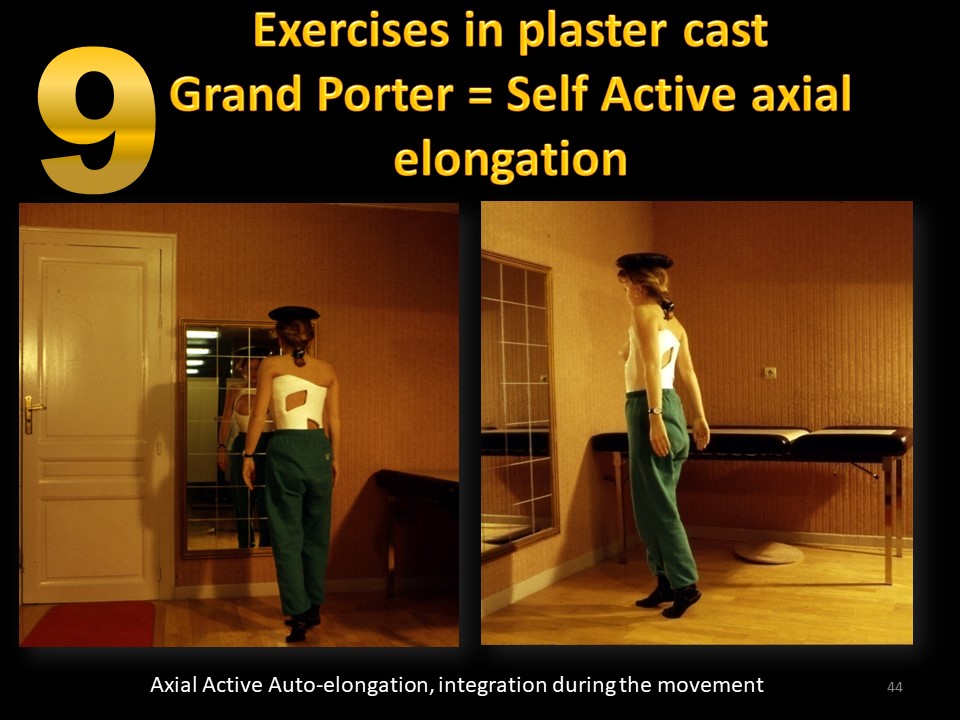 |
The active axial self-stretching exercise is one of the most characteristic exercises of the Lyon method. It is especially used i, brace to avoid the inconvenience of accentuating the flat back and to reprogram the whole extra-pyramidal system in the corrected position. The child walks on tiptoe, which reprograms the kinetic sensors of the reticulo-spinal tract. A small bag of sand on the head reprograms the kinesthetic sensors of the vestibulo-spinal and tecto-spinal system, especially as the child is asked to walk in front of a mirror. Walking will alternate with stationary positions that reprogram the statesthetic sensors. |
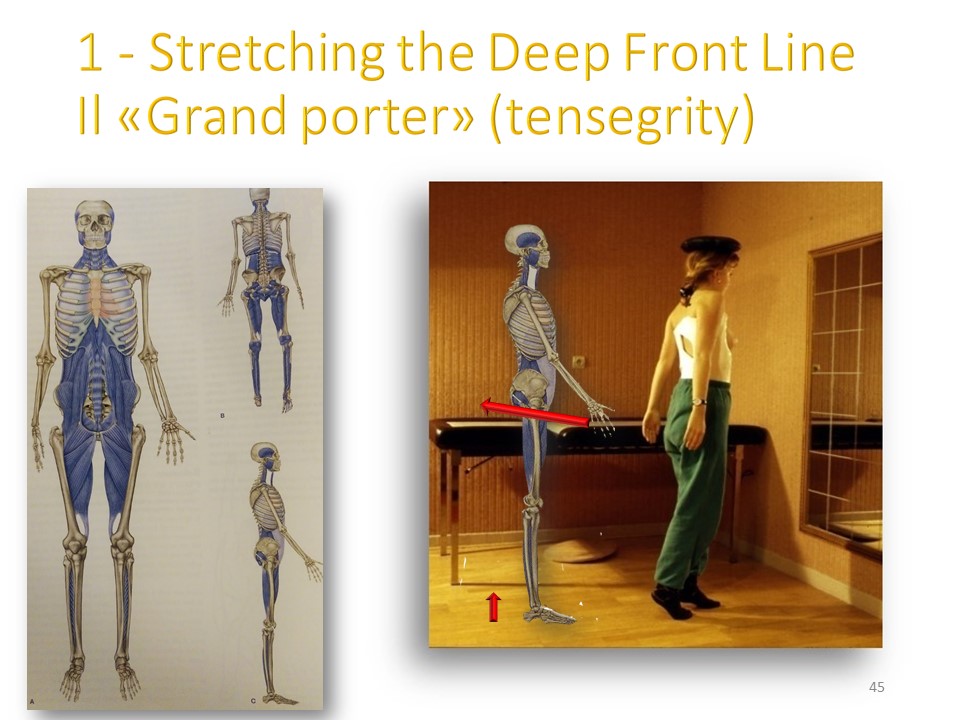 |
In the sagittal plane, harmony must be respected with realignment of the Tragus, Acromion, Trochanter, Malleolus line after in-brace correction. |
 |
|
The rubrospinal tract for larger imbalances will be requested by the ball of the Swiss physiotherapist Suzanne Klein-Vogelbach. The child is seated on the ball and asked to roll it, while keeping the sagittal isokinetic balance. The upper limbs are automatically called upon. The asymmetry of amplitude in the frontal plane is clearly visible in this child. |
|
The rubro-spinal tract can be coupled to the tecto-spinal using the level stick. The exercise is then focused on the thoracic region with correction of the flat back. The overall backward projection of the trunk and the loss of lordosis will be corrected in a second step. |
|
 |
|
After the sitting position, the exercises will be performed in a standing position. The use of a tilting plate makes it possible to stimulate the vestibulo-spinal system in a plane, for example frontal. When balance is reached, the reticulospinal system is sollicited. The physiotherapist controls the sagittal isostatic balance posture with sometimes large projections of the trunk forward. |
|
Exercises in the standing position can be performed with active axial self-elongation. The feet are fixed on the ground to stimulate the reticulospinal tract. If the lordosis is too great, a flexion of the lower limbs will relax the psoas, rectus femoris and pelvi-trochanteric muscles. Once the iso-static equilibrium has been reached, the child is asked to flex the trunk forward up to 90 ° while stabilizing the trunk. This posture puts tension on the lumbopelvic fasciae. When stabilization is acquired, the feet will be placed on a half ball balance tray to stress the vestibulo-spinal tract in the 3 planes of space. The same postures will be reproduced until the trunk-thigh flexion at 90 °. The Tragus Acromion Trochanter alignment is here well preserved. Statesthesic and kinesthesic sensors are stimulated without excessive deviation in the sagittal plane. The same posture must be kept when passing from standing to sitting position and when picking up an object on the ground. |
|
 |
|
| > | Restoring the spinal tensegrity in the corrected position is essential for the future stability of scoliosis. Core axial stabilization exercises are often performed in quadrupedal posture. The positioning of the upper limbs is specific with hands, forearms and elbows crossed on the ground to promote isostatic thoracic kyphosis. The trunk is in axial elongation. A trunk-thigh square angle of 90 ° is asked, which puts in tension the ilio-psoas and the anterior chains of the lower limbs. In a second step, the positioning of the upper limbs is modified with adduction of the convex shoulder girdle to obtain a derotation of the apex of scoliosis. On the concave side, an extension of the upper limb is requested to complete the derotation by the concavity. In a third step, it is the concave fascia of the latissimus dorsi and the fascia lata convex which will be tensioned to obtain maximum detorsion. |
|
After core stability in the sagittal plane, the core stability will be achieved in the frontal plane. The classic yoga side plank is modified with elbow and convex forearm on the floor. Trunk and lower limbs are rectilinear with control of isostatic lordosis. The concave upper limb will then be placed in extension, which stretches the fascia of the latissimus dorsi. The posture will be maintained at least 7 seconds. |
After the two static exercises in the sagittal and frontal plane, the Klein-Vogelbach ball will be used in a downward-facing dog bent knees posture. The upper limbs are positioned in the same way like Russian squat dance. An extension of the lower limbs is requested while maintaining the entire spine in the position of isostatic balance. This exercise solicits more specifically the vestibulo-spinal tract with both Statesthesic and kinesthetic sensors. |
|
 |
The Lyon braces and in particular the ARTbrace eliminate the median contact of the spinous process with the brace. Given the richness of the sensors at this level, we recently added a 13th complementary exercise: the dynamic beam. |
 |
The beam exercises were classic and already described with the Milwaukee brace. The beam was stable and the child stimulated the kinesthetic sensors of the vestibulo-spinal and rubro-spinal tracts in the event of a fall. |
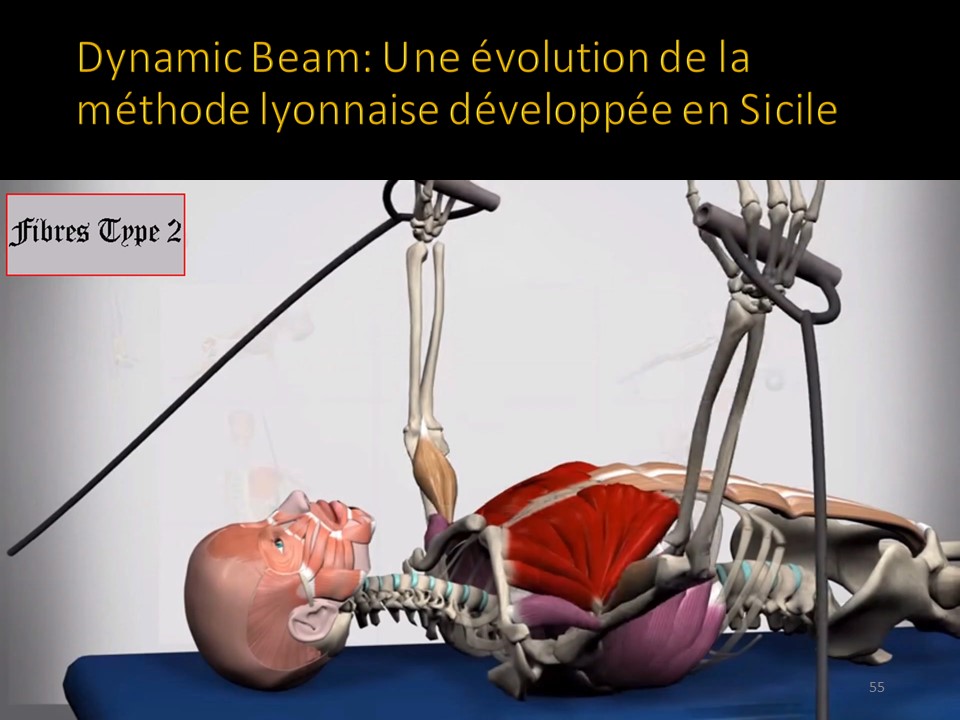 |
Dynamic Beam It is an innovative and multifunctional exerciser, which expands the professional background of the kinesiologist in the field of vertebral deviations and back pain. It acts on the polysensory system balance by improving the stability of the spine through the activation of the deep spine muscle. Dynamic Beam through stimulation of the biomecannical and physiological system of the column, puts it in the condition of actively participate in the reorganization of the Postural Tonic System. Its unbalancing action, during the execution of an exercise, stimulates the Spinal Proprioceptive System differently than what happens when the same exercise is performed in standing or sitting position. |
The dynamic beam allows a complementary physiotherapy of scoliosis both in children and in adults. The elastic work of the upper limbs stimulates all the sensory sensors which are sensitive to stretching. The classic work of the pectoral muscles will limit the tendency to flat back and the strengthening of the concave serratus major facilitates derotation by concavity. The instability of the beam stimulates all the static and dynamic sensors of the extra-pyramidal system and strengthens the tone of the axial muscles. The global extension takes place in disc and vertebral decompression. The deep sensitivity of the spine or proprioception is stimulated. The uses are multiple. It is possible to reprogram the sensors in the corrected scolisis posture. For adults the 90 ° angled trunk-thigh flexion facilitates tensegrity readjustment at the level of the pelvis. Walking on a beam with level stick control requires all the kinesthetic sensors and the tecto-spinal tract. A system of acquisition of 9 sensors placed at the level of the two girdles and the apex of the kyphosis makes it possible to control the balance concavity - convexity. The patient can control the recordings on his own screen and monitor the progress of physiotherapy. |
|
 |
|
 |

