")
")
")
")
")
 |
|
 |
|
 |
The Lyon method is the oldest in Europe. It was codified by Charles Gabriel Pravaz nearly 200 years ago in the book New Method for the Treatment of Vertebral Deviations. It has adapted to the evolution of technology with, in recent years, the digital transformation. Update books were written regularly and I had the honor to co-write the last one 40 years ago. The main features of this method will be studied in this chapter with a greater emphasis on understanding the method, although many examples and typical sessions will illustrate the main principles. |
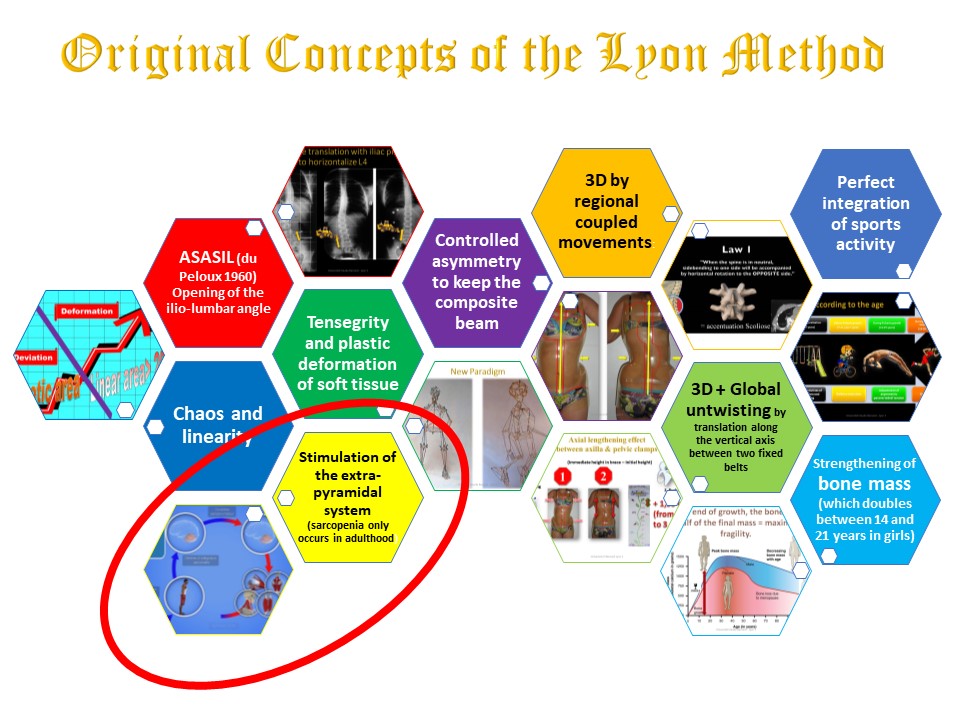 |
The fundamental concept illustrated by the Pravaz orthopedic swing is that of stimulation of the extra-pyramidal system. |
 |
|
 |
Reminder of the anatomo-physiological basis of the extra-pyramidal system. |
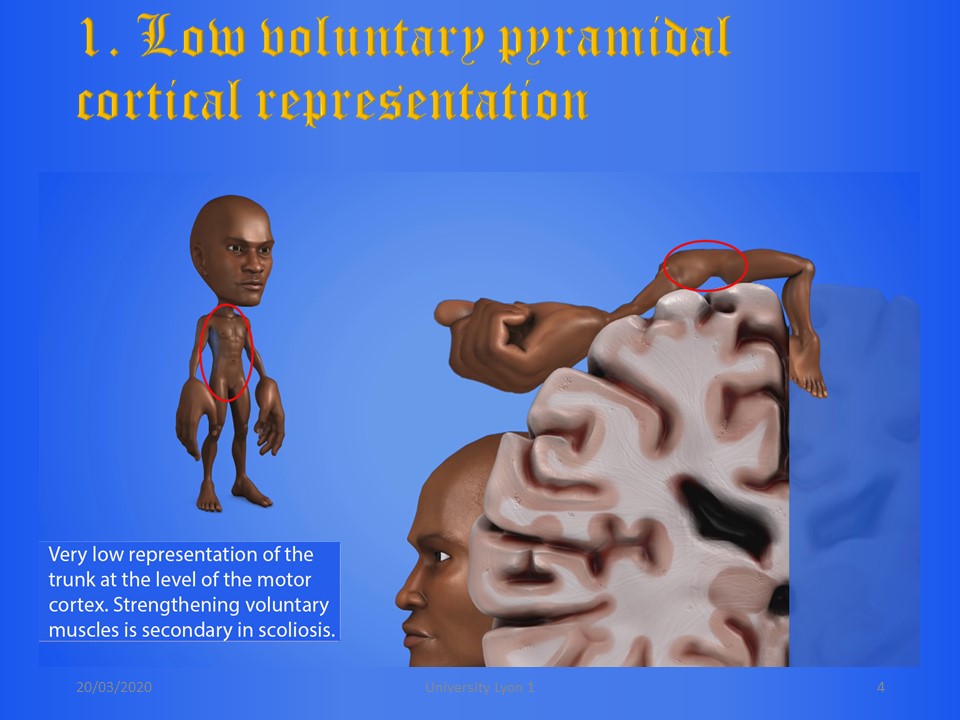 |
At the level of the spine, the representation of the pyramidal system is very limited. There are few type II pyramidal muscle fibers. |
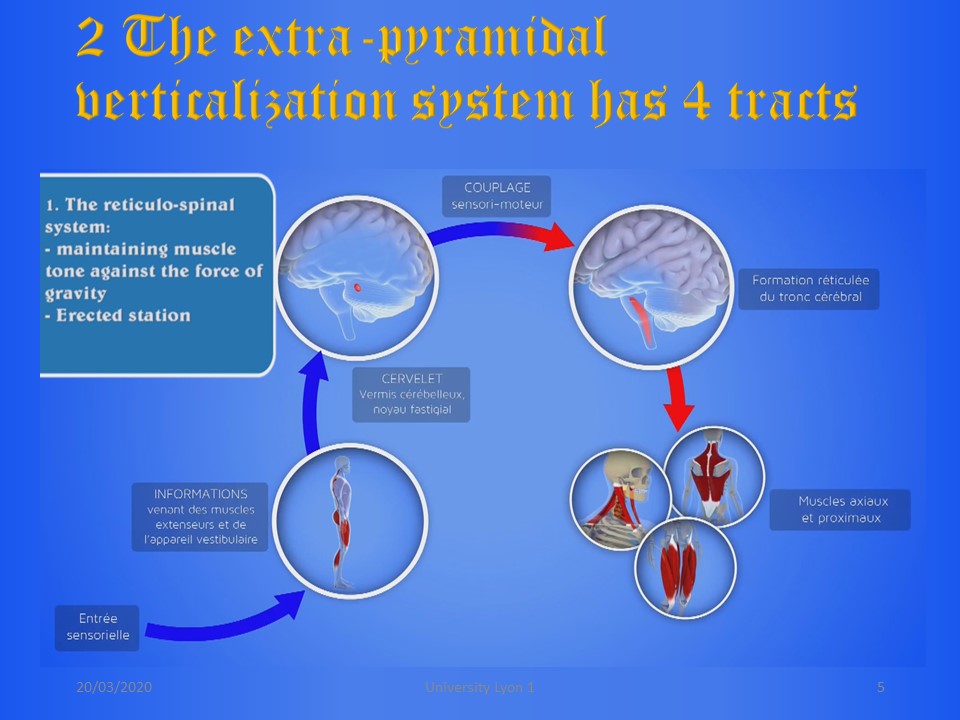 |
The extra-pyramidal system has 4 specialized tracts. The first is the reticulospinal tract, which specializes in muscle tone against gravity. It is the way of standing posture. Sensorimotor coupling takes place at the level of the reticular formation of the brainstem. |
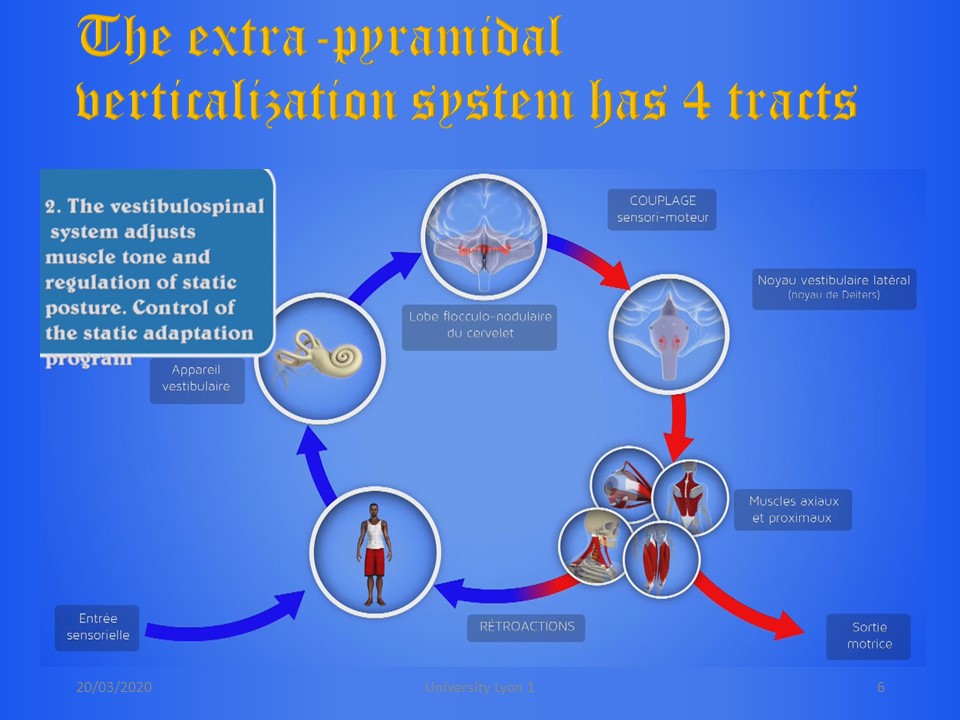 |
The second is the vestibulospinal tract, which involves the vestibular balance system. This tract controls the static adaptation, for example the feet on a tilting platform. The consequence is the search for a balance of the head despite the postural correction. |
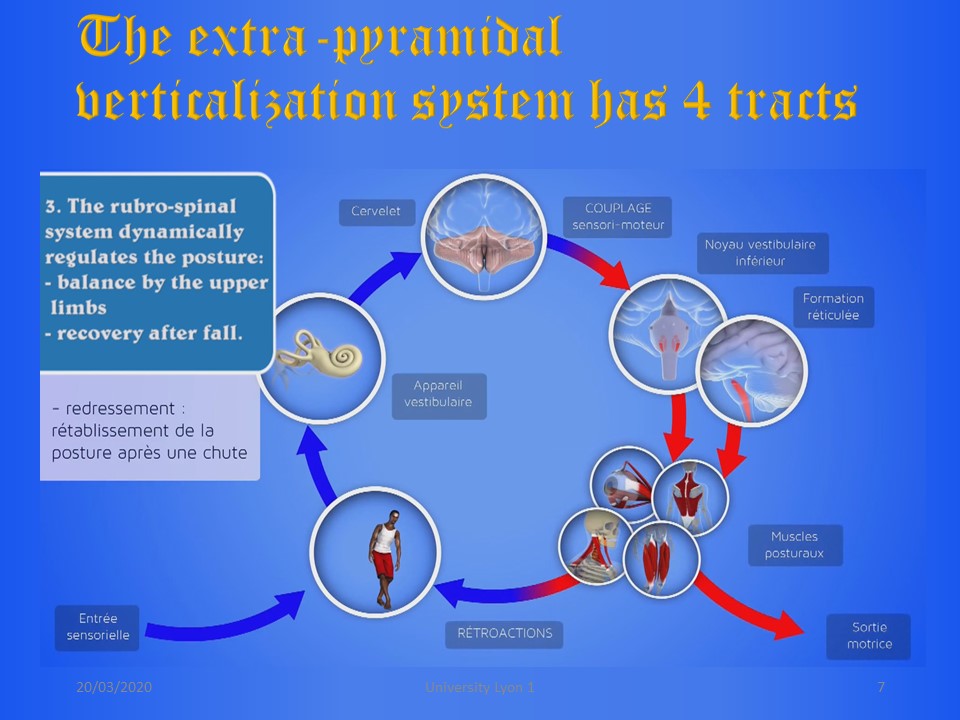 |
The third is the rubro-spinal tract which controls the dynamic posture after a greater imbalance to avoid the fall. It is used during exercises on a Swiss ball. Sensorimotor coupling also concerns the vestibule and the red nuclei of the reticular formation. |
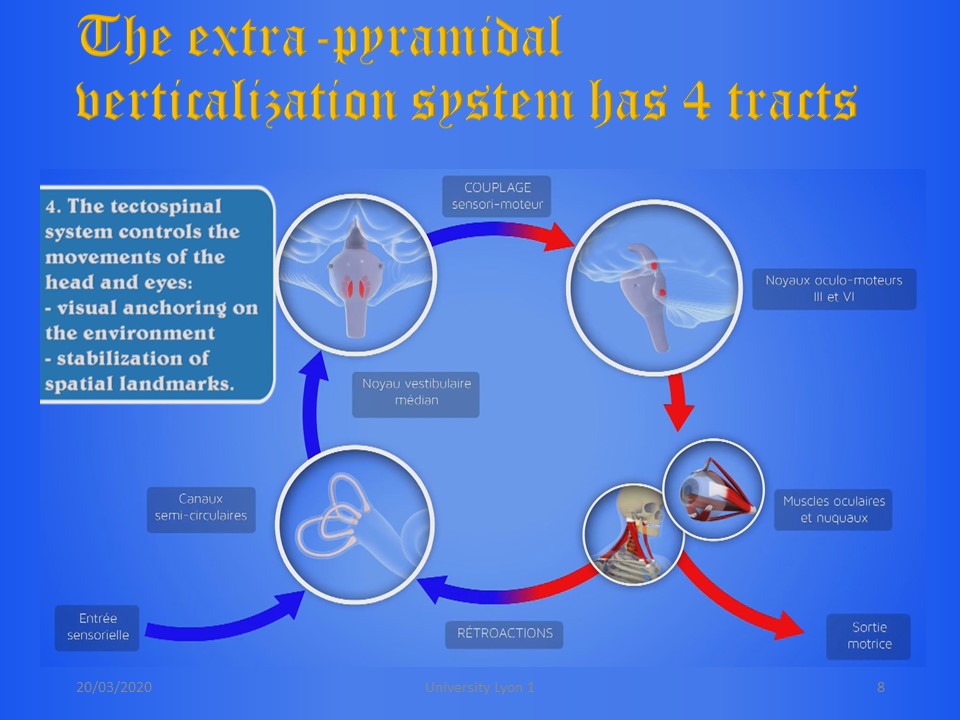 |
The fourth tract is the tectospinal tract specific to the cervical spine and the eyes. Sensory entry is almost exclusively at the level of the semi-circular canals. The coupling involves the oculo-motor nuclei, because the effector muscles are at the level of the eyes, cervical spine, and upper limbs. |
 |
The four specific functions of the extra-pyramidal system are grouped here with the representation of the balancing cone in an inverted pendulum of chaotic type. The tecto-spinal tract works simultaneously with the other tracts, it is requested by the mirror or the leval stick. |
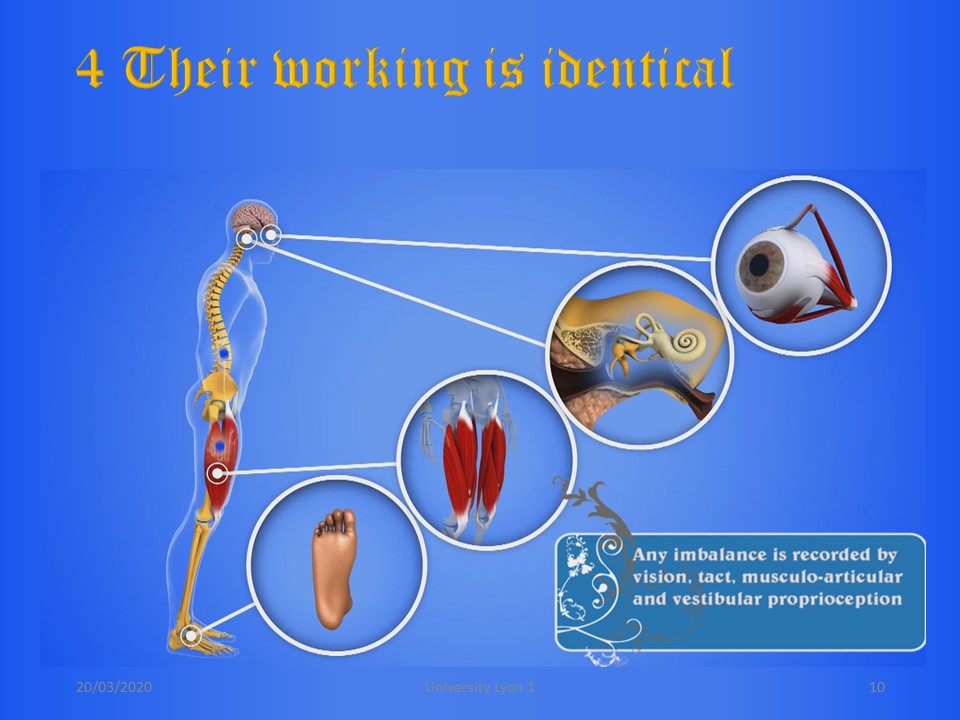 |
The operating mode of the 4 tracts is identical. Sensitive sensors are mainly used at the level of the feet for the reticulospinal tract, at the level of the lower limbs for the vestibulospinal tract, at the level of the vestibules for the rubro-spinal tract, at the level of the semi-circular canals and the eyes for the tectospinal tract. |
  |
Sensitive integration takes place at the level of the oarietal and occipital cortex. |
 |
The information is transmitted to the motor centers which will send an order of muscular contraction intended to compensate for the imbalance. |
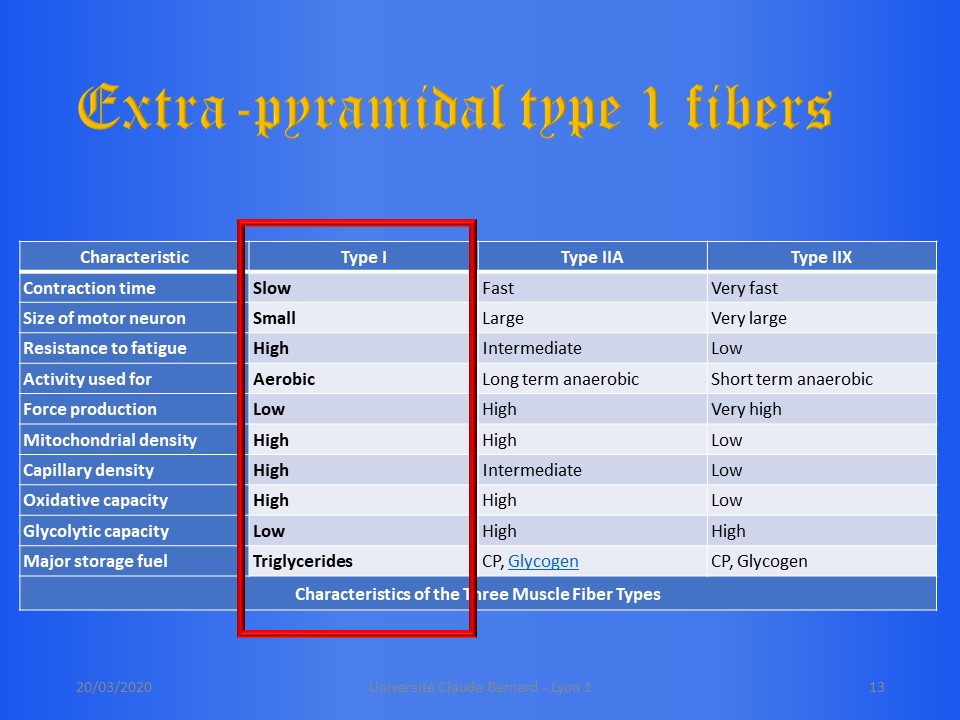 |
The extra-pyramidal system manages Type I fibers, which are slow, red, aerobic fibers that work with triglycerides. |
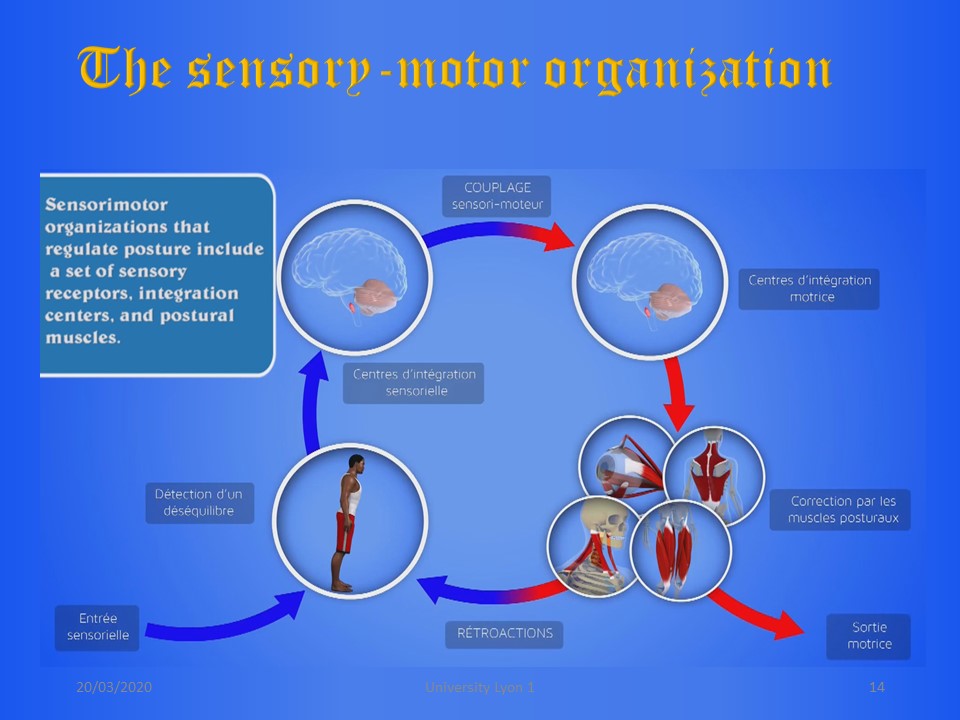 |
Overall, sensorimotor organization includes a set of sensori receptors, cortical integration centers, sensorimotor coupling, motor integration centers and postural muscles. These postural muscles are themselves sensory sensors, which allows feedback. |
 |
During scoliosis, the system gradually adapts to the deformation. When we are going to correct scoliosis, we must associate a reprogramming of the extra-pyramidal system in the corrected posture. The more corrective the bracing and the surgery, the more necessary this reprogramming physiotherapy. |
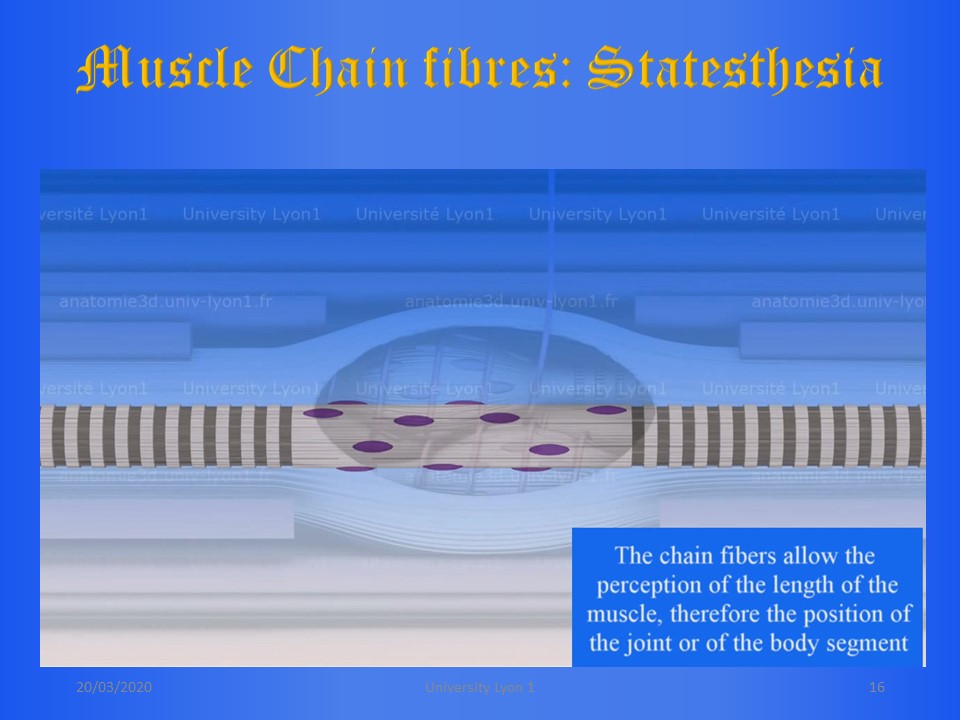 |
At the muscle level, there are two types of receptors. Both are sensitive to stretching. The chain fibers are statesthetic and sensitive to the length of the muscle at the end of the movement. |
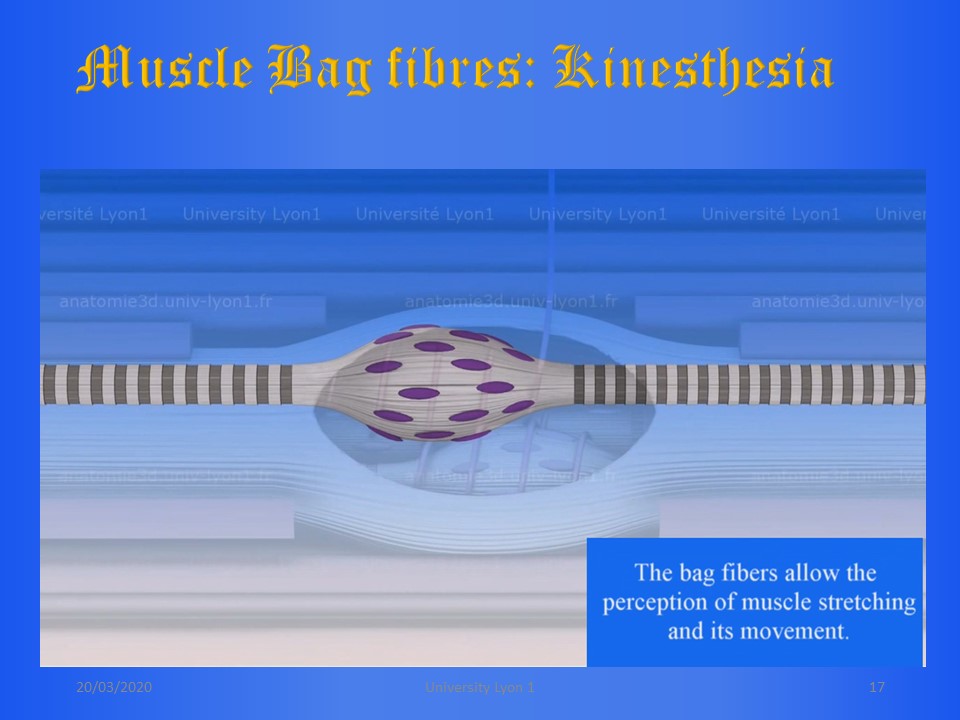 |
On the contrary, the kinesthetic bag fibers are sensitive to movement. |
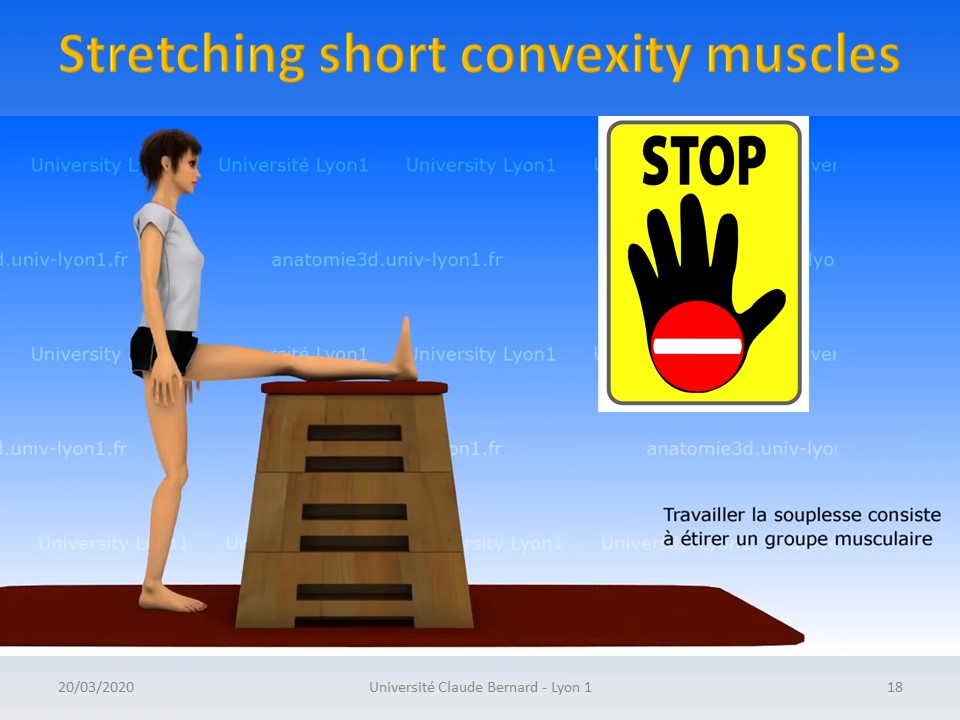 |
In scoliosis, the shortest muscles have often to be stretched. This stretching should be slow to avoid the myotatic reflex. The muscle receptors operate in frequency modulation with a relaxation or habituation phase after a voluntary contraction. This habituation phase promotes a new passive or activo-passive stretching before a new voluntary contraction. It is the mechanism of extra-pyramidal stretching by hold-relax. |
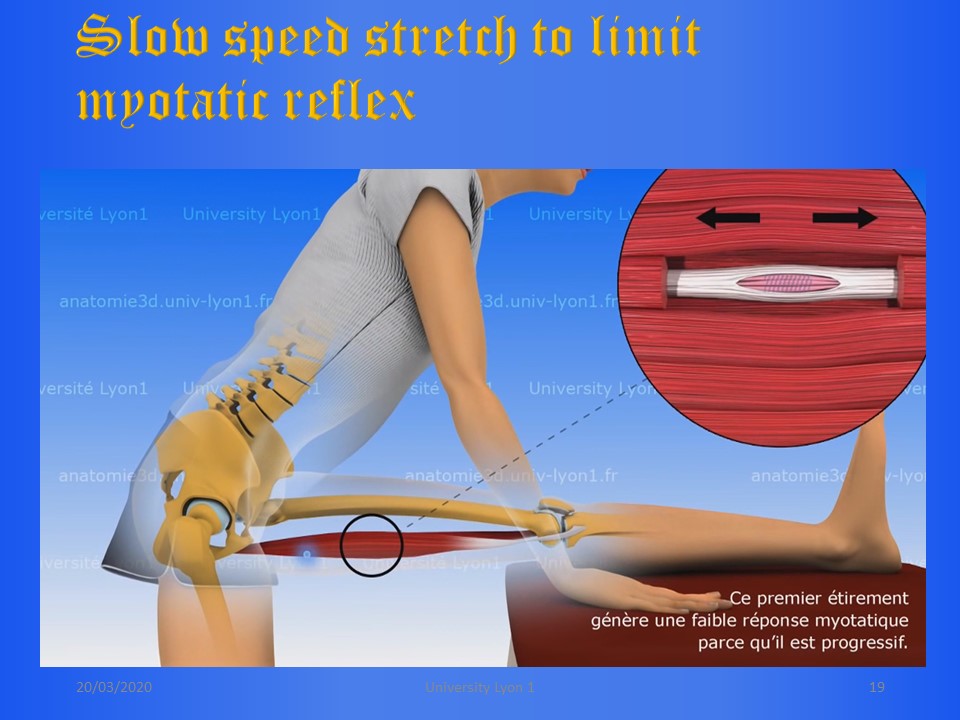 |
The first step is therefore a very slow and progressive stretch to limit the myotatic reflex. |
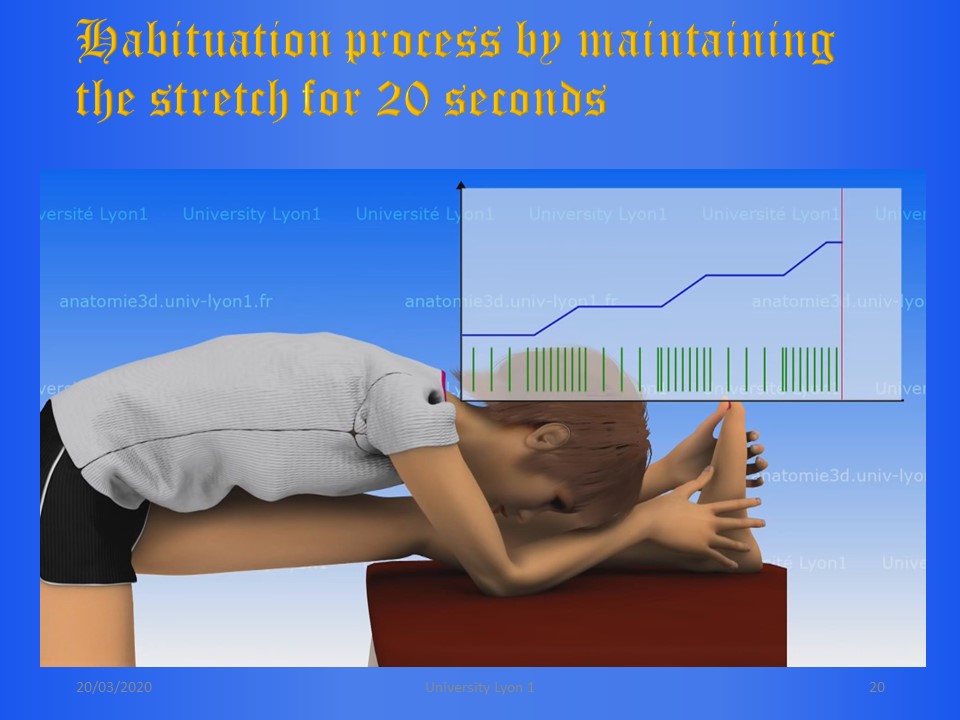 |
During each successive contraction, the frequency of the sensors increases from 50 to 100 Hz. At the end of the contraction, the frequency decreases to 30 Hz for 20 seconds below the rest frequency of 50 Hz. We can then take advantage of this relaxation phaserto further stretch the fascia and so on until the occurrence of painful phenomena. |
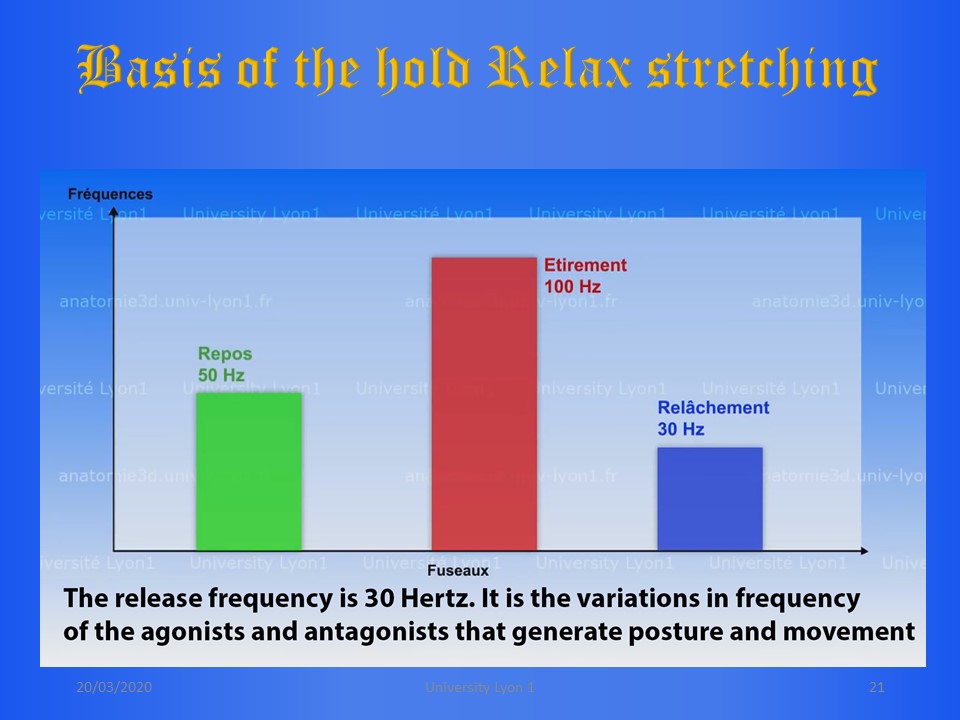 |
The rest frequency is 50 Hz, the muscular contraction frequency is 100 Hz, the release frequency is 30 Hz. The variation in frequency of the agonists and antagonists generate posture and movement. |
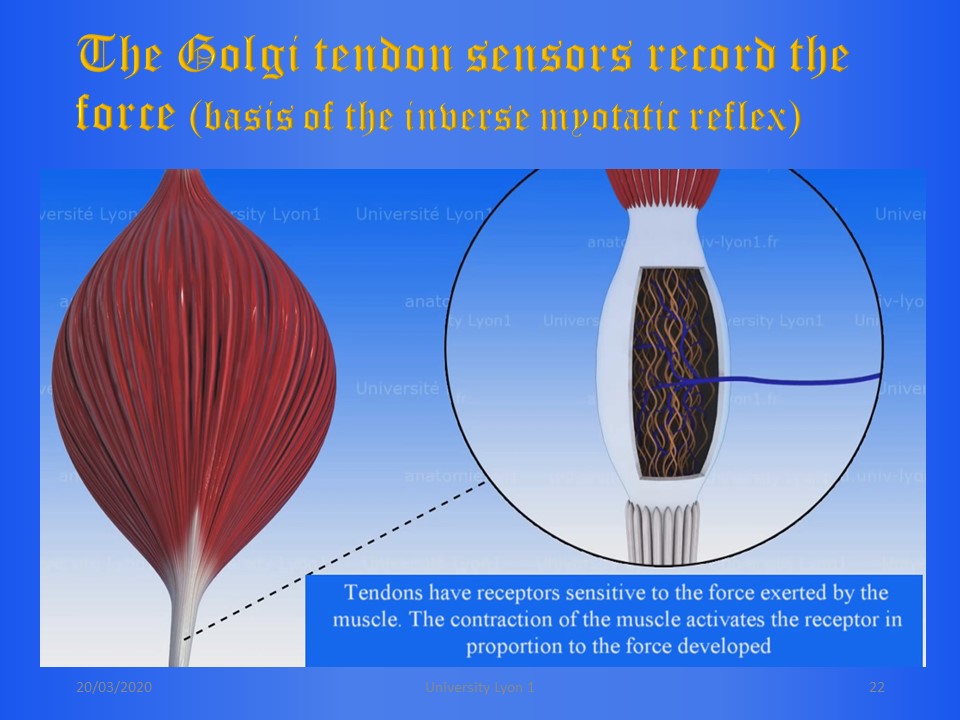 |
This muscular mechanism is supplemented by Golgi sensors at the level of the tendons. They are the basis of the inverted myotatic reflex. Golgi sensors are sensitive to the force exerted by the muscle and their frequency is proportional to this force. |
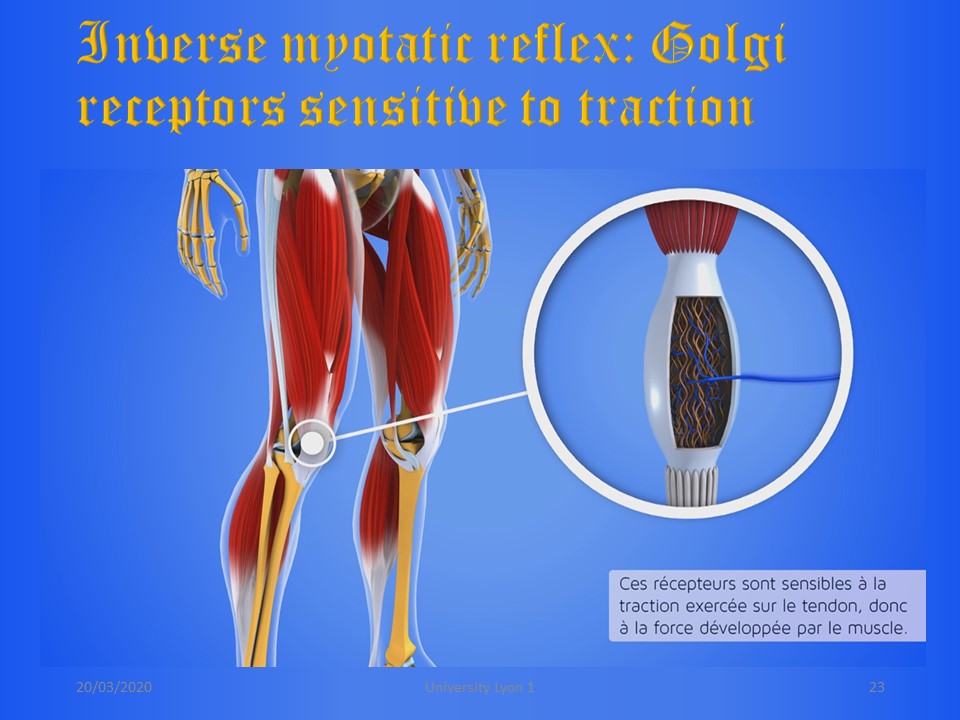 |
The coding of the tension takes place at the level of all the tendons and particularly at the level of the small deep segmental paravertebral muscles. |
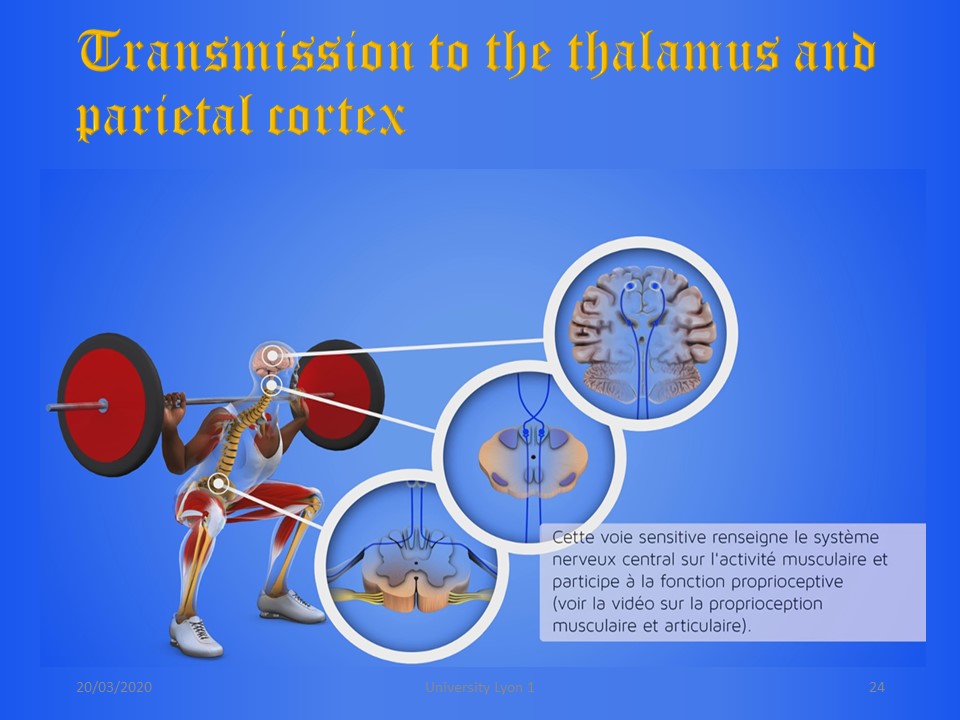 |
The force developed by each muscle during traction is coded at the level of all tendons. The influxes are continuously transmitted to the thalamus and the parietal cortex. |
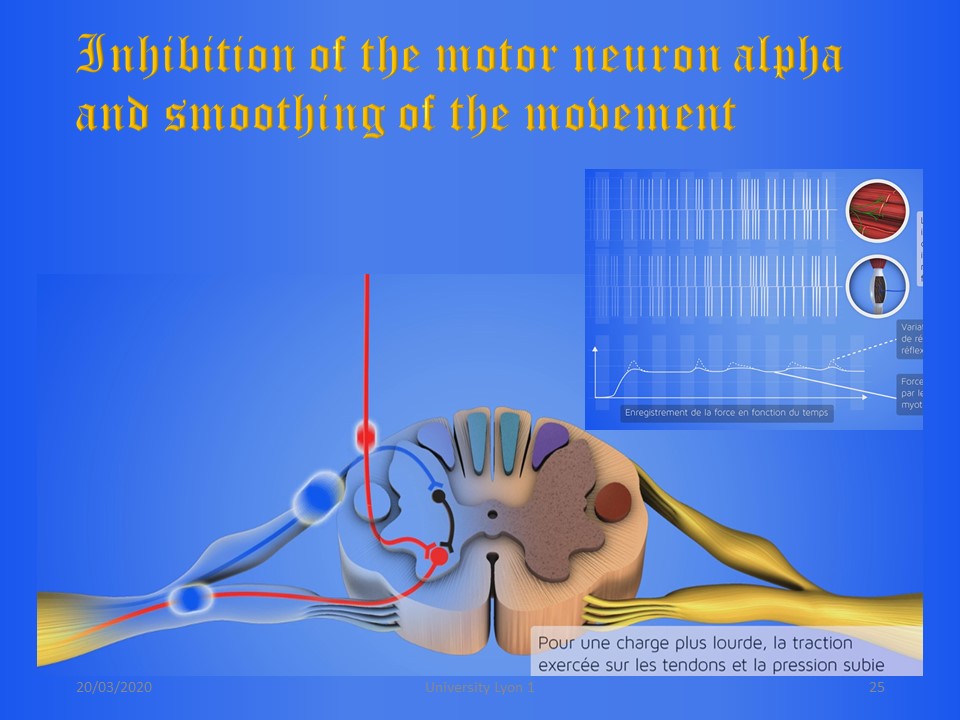 |
The reflex loop is located at the medullary level, type inhibition of the motor neuron alpha. The result is a smoothing of the movement. |
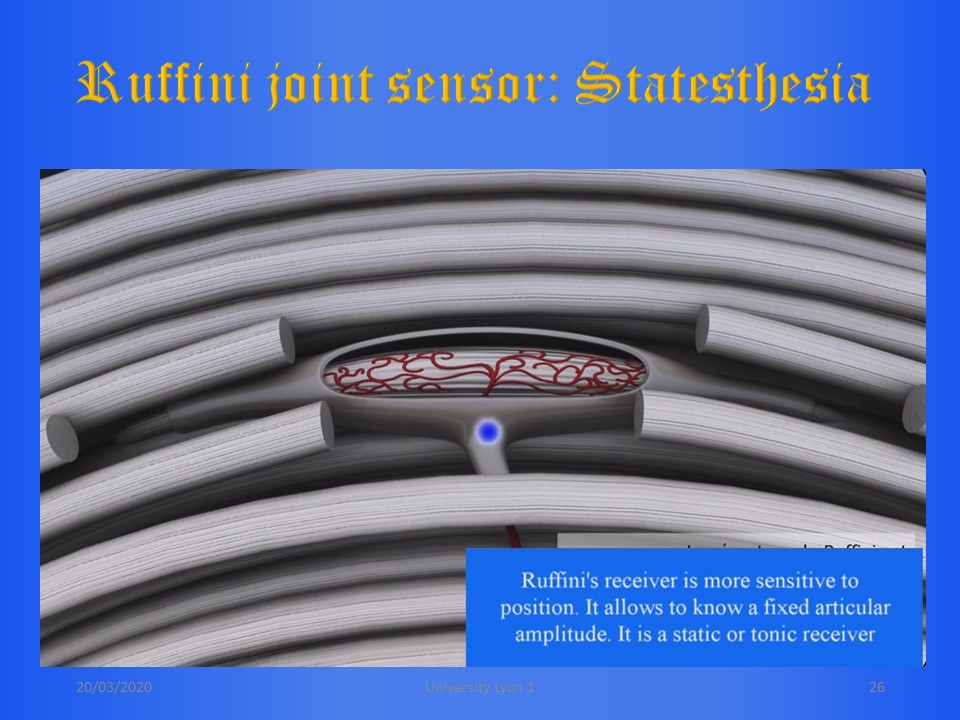 |
At the level of the joints and ligaments, there are also 2 types of statesthetic and kinesthetic sensors. Ruffini's statesthetic sensors are sensitive to the position of the joint. They provide information on the range of motion. |
 |
Pacini's kinesthetic sensors are sensitive to the movement of the joint capsule and ligaments, particularly during maximum amplitude. These are dynamic or phasic sensors. They provide information on the speed of movement. |
 |
The 3D postural correction is identical to that used for the regional molding in the corrected position of the ARTbrace. |
 |
|
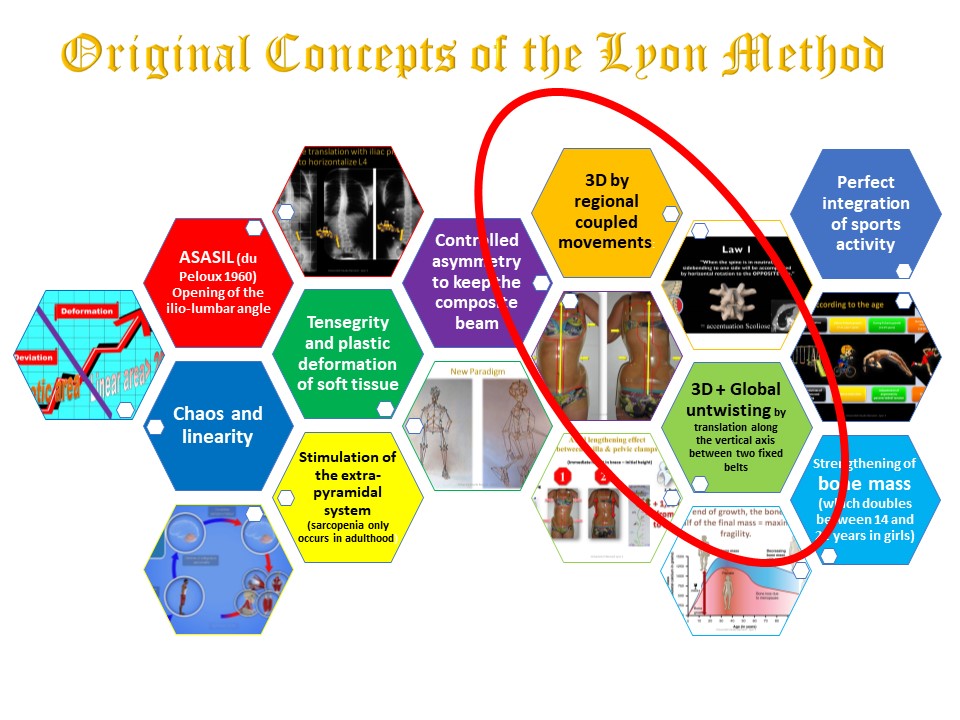 |
The 3D postural correction is based on the law of coupled spinal movements and on the overall detorsion by translation along the vertical axis in active axial self-elongation. These two mechanisms will be coupled during the production of the brace, bur they will be dissociated in physiotherapy, because the isostatic sagittal balance is incompatible with the translation along the vertical axis. |
 |
3D postural correction is carried out regionally by physiological thoracic and lumbar blocks. Care will also be taken to place the pelvic block in a physiological pelvic version determined by the lumbopelvic incidence appropriate to each patient.. |
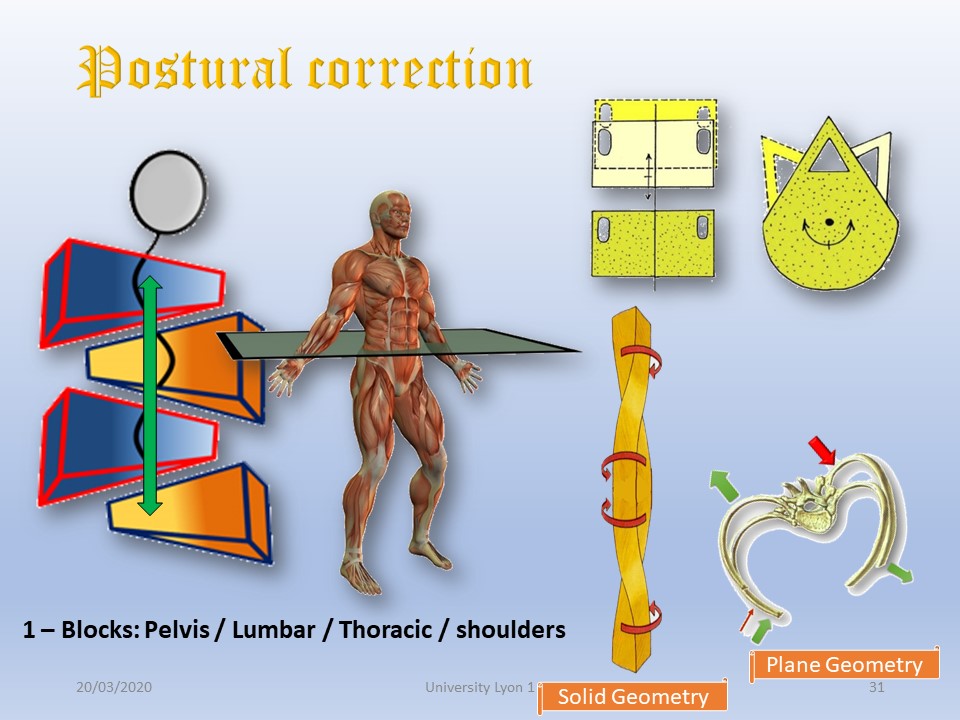 |
The translation along the vertical axis requires two fixed points, one at the pelvis, the other at the shoulders. The fascia of the latissimus dorsi and the trapezium facilitate the extension, for example but stabilizing on the iliac crests and asking for a shrug of the shoulders as in the “grand porter". |
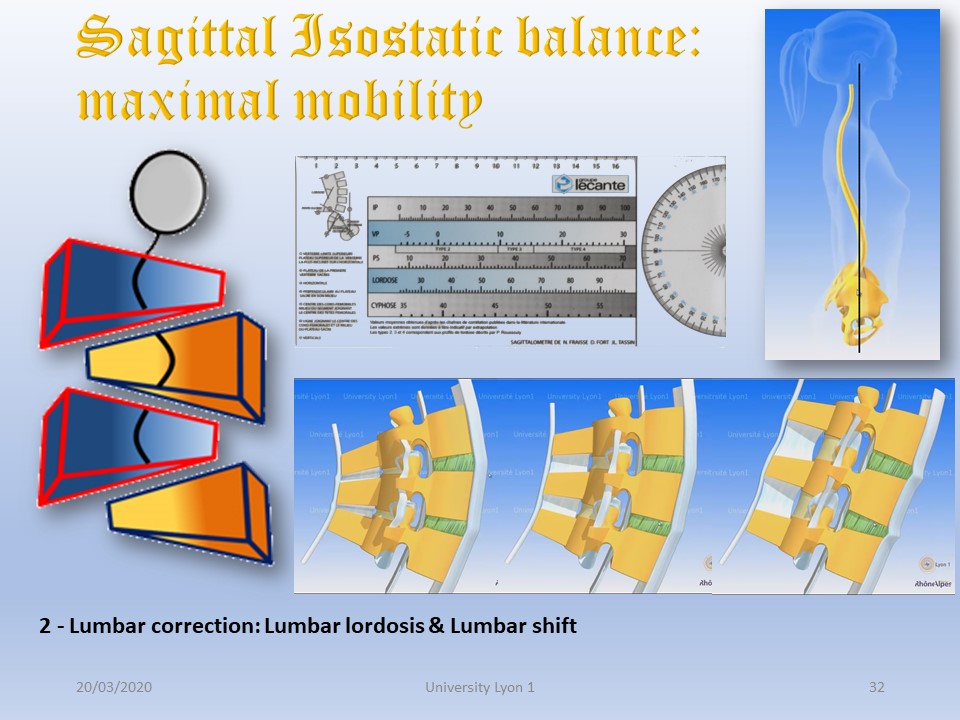 |
The first step in 3D correction by coupled movements is to determine the sagittal isostatic balance with the sagittalmeter. In this position, mobility is maximum in the frontal plane. |
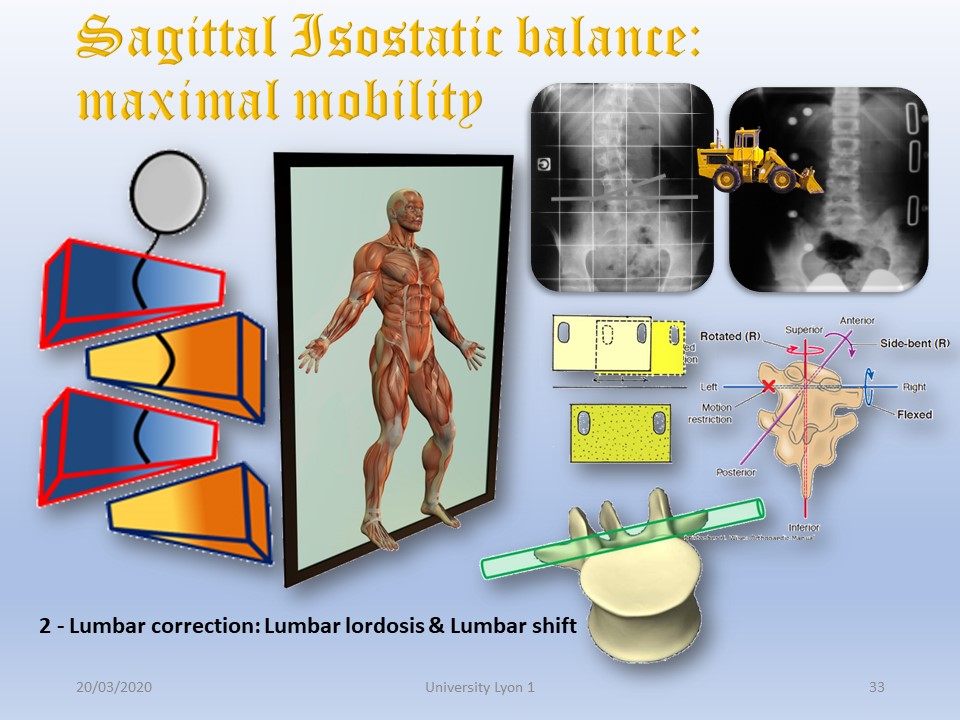 |
In the lumbar region, the sagittal orientation of the facet joints must be taken into account. The mobility of the lumbar spine is mainly located in the sagittal plane. The height of the intervertebral discs, however, allows translation along the horizontal axis passing through the transverse. It is the shift which aims to realign the vertebral bodies on the line of gravity in the frontal plane. The other advantage of the shift is the stretching of the convex transverso-sacral ligament in case of tilt of L4. |
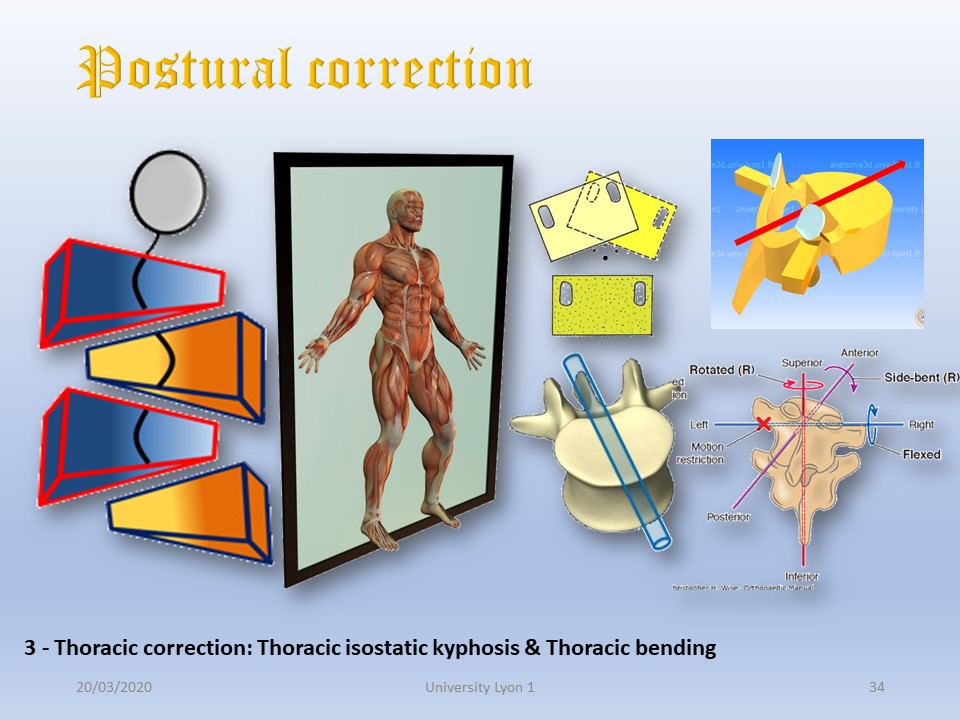 |
On the other hand, at the thoracic level, the facet joints are oriented in a frontal plane. The correction in the frontal plane can therefore be carried out by rotation around the sagittal axis. It is the frontal corrector bending which will be maximal in isokinetically balanced kyphosis. |
| |
The 3D postural correction is based on the law of coupled spinal movements and on the overall detorsion by translation along the vertical axis in active axial self-elongation. These two mechanisms will be coupled during the production of the brace, bur they will be dissociated in physiotherapy, because the isostatic sagittal balance is incompatible with the translation along the vertical axis. |
 |
|
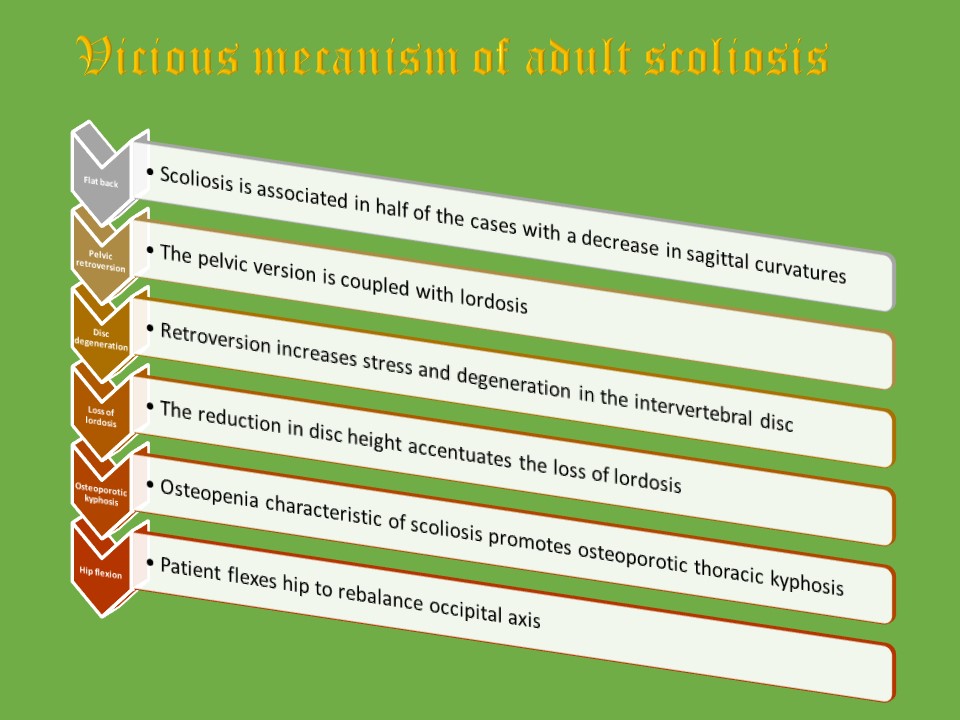 |
The vicious mechanism of scoliosis in adulthood must be known, even when treating adolescent scoliosis only. The first step is the frequent association of a flat back with scoliosis. This flat back is often favored by braces or physiotherapy based solely on active axial self-elongation. Knowing that the pelvic version is coupled with lordosis, pelvic retroversion promotes hypolordosis and increased stress on the disc and accentuate degenerative phenomena. These degenerative phenomena result in a loss of height of the intervertebral disc which will promote hypolorosis. At this level it is a veritable vicious circle. Osteopenia promotes upper thoracic kyphosis. Unfortunately sarcopenia prevents upper muscle compensation and the patient will have to flex their hips and knees to recover the line of gravity. |
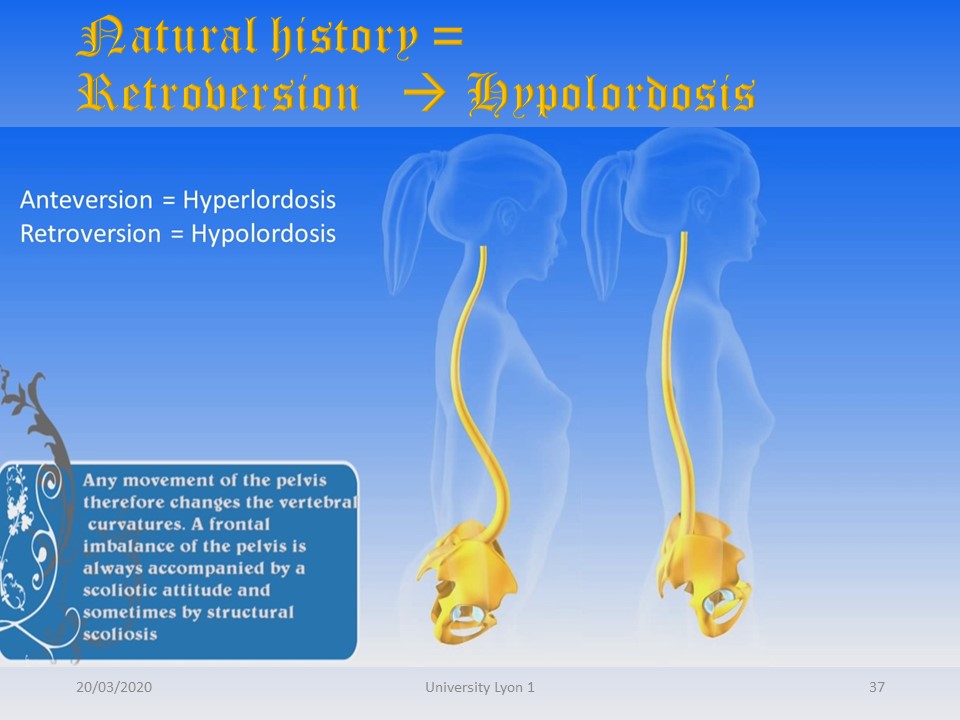 |
All the movements of the pelvis in the sagittal plane will modify the curvatures of the spine. The anteversion accentuates the curvatures, the retroversion reduces them. |
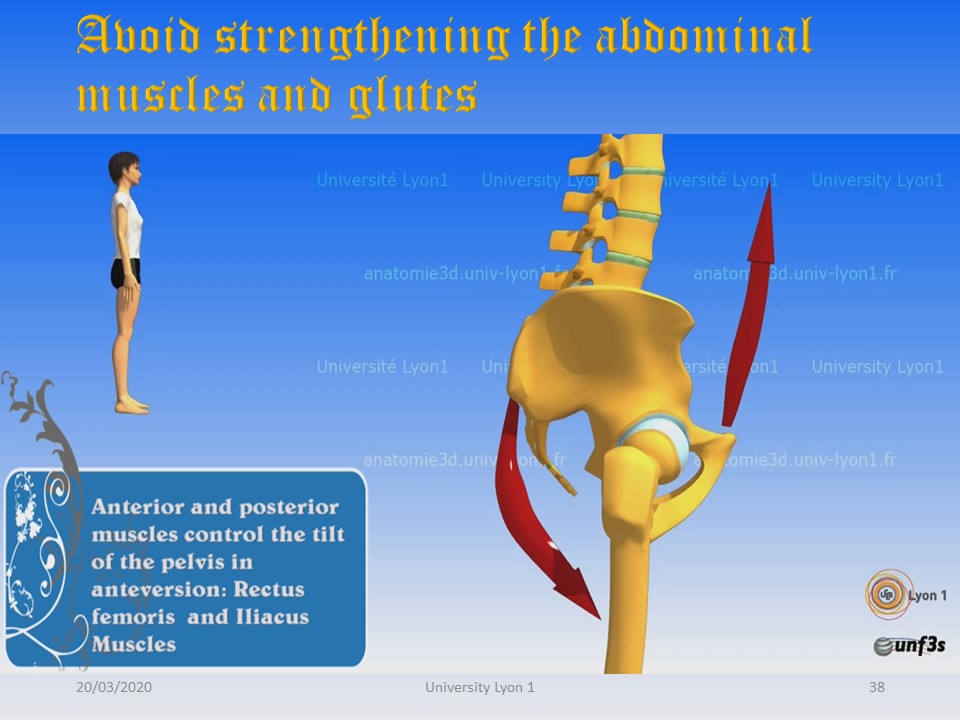 |
The pelvic version is controlled by the musculature. Glutes and abs are not to be strengthened in scoliosis, as they promote retroversion. |
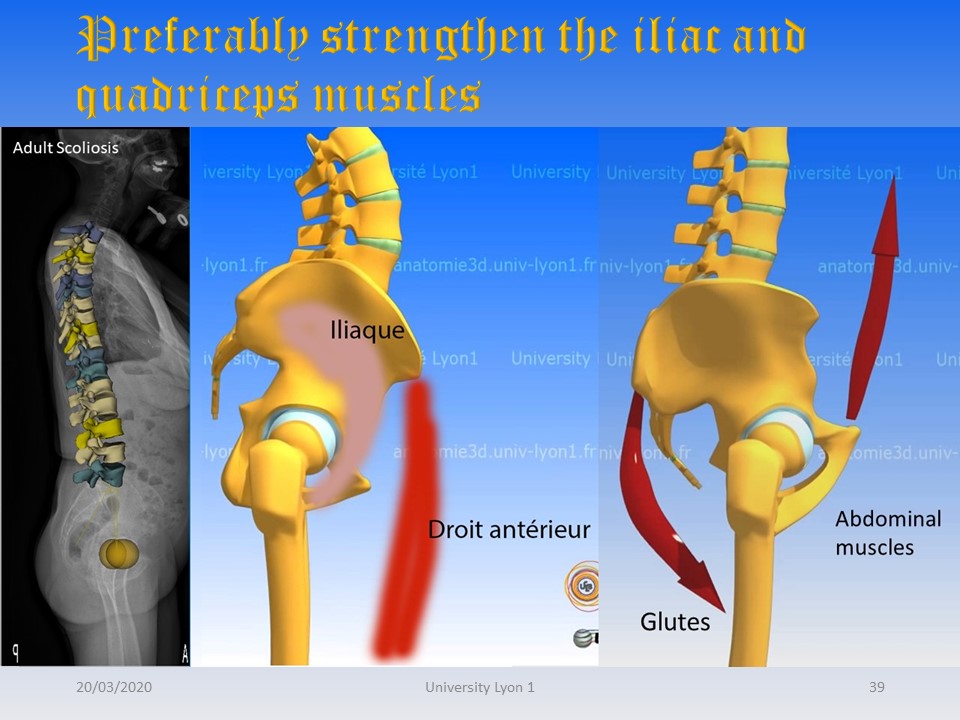 |
On the other hand, the quadriceps rectus femoris and the iliac favor anteversion, it is therefore the muscles to be strengthened in priority in scoliosis in adults. |
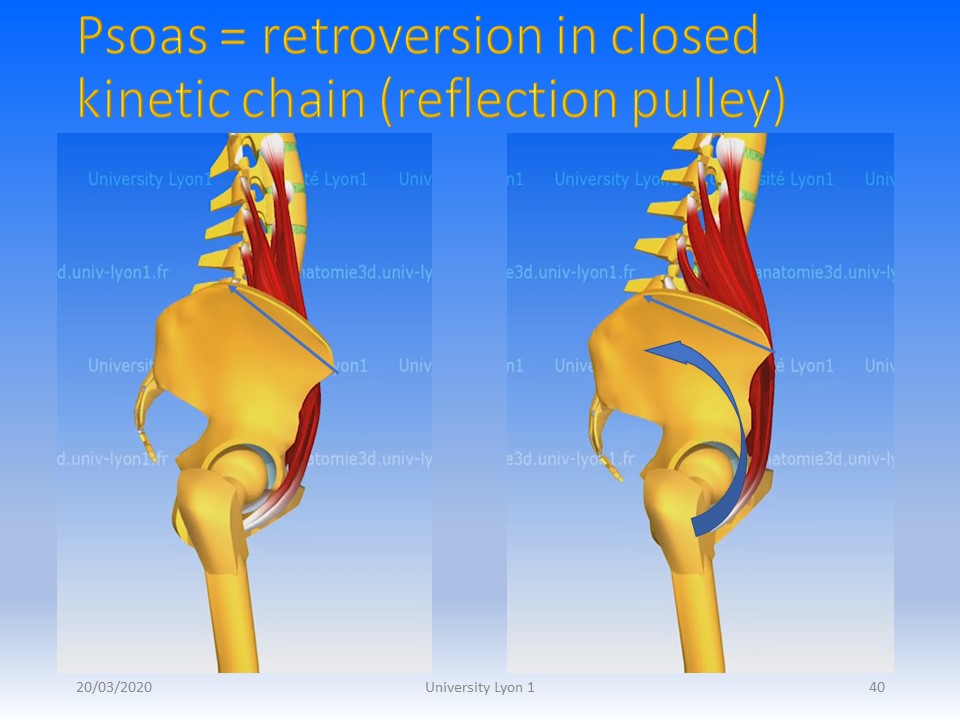 |
The contraction of the two ilio-psoas promotes lordosis and pelvic anteversion through the iliac. However, when wearing a brace creating a closed kinetic chain, the reflection pulley at the level of the iliac bone will have an opposite effect of retroversion and hypo-lordosis. It will therefore be necessary to contract the ilio-psoas in a kinetic chain open at its upper part. |
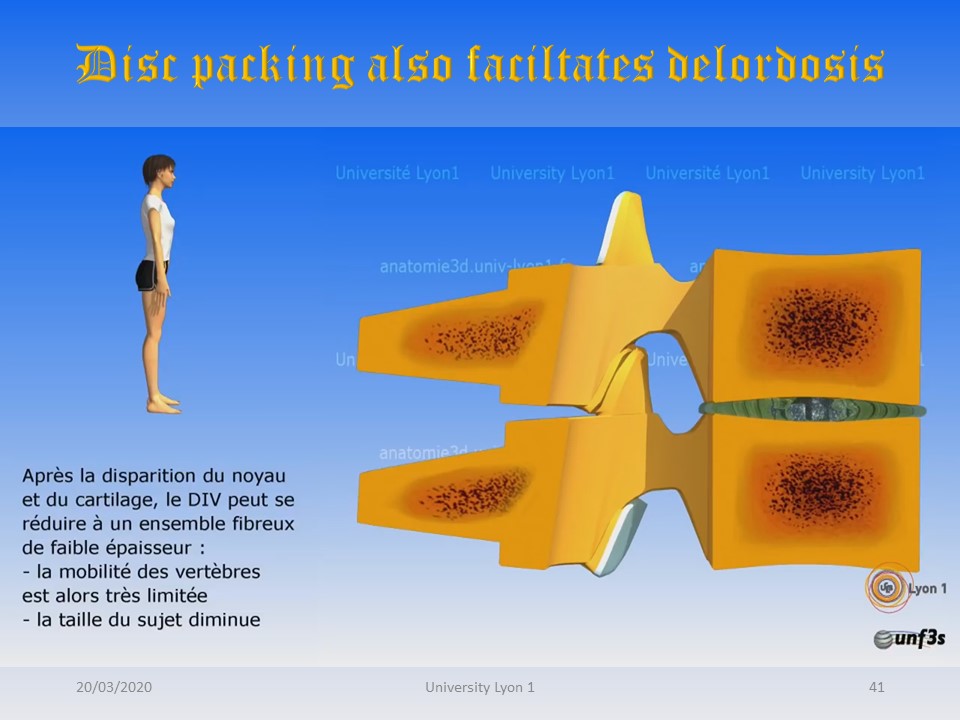 |
After the nucleus and cartilage have disappeared, the intervertebral disc can be reduced to a thin fibrous complex. The patient's size decreases as well as their mobility. In scoliosis, there is an asymmetry of load at the level of the facet joints, the concave posterior facet joint is strongly impacted, the convex posterior facet joint is distended. It is the beginning of the rotary dislocation. |
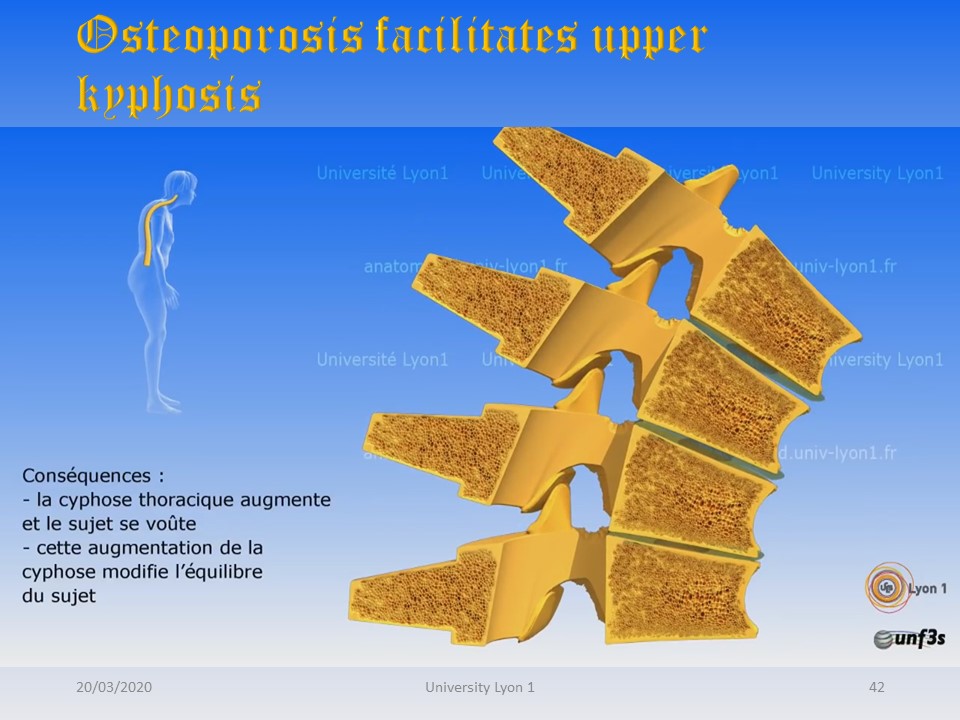 |
Osteopotic vertebral compaction predominates at the level of the upper thoracic kyphosis. It is the anterior wall of the vertebral body which settles, accentuating the upper thoracic kyphosis. This increase in kyphosis projects the head forward and changes the vestibular balance and posture. The head is no longer at the level of gravity line. |
 |
Shoulders upper limbs and head are projected forward. To rebalance the forces, the patient will flex his hips and knees so that the buttocks move back behind the line of gravity thanks to a retroversion of the pelvis. |
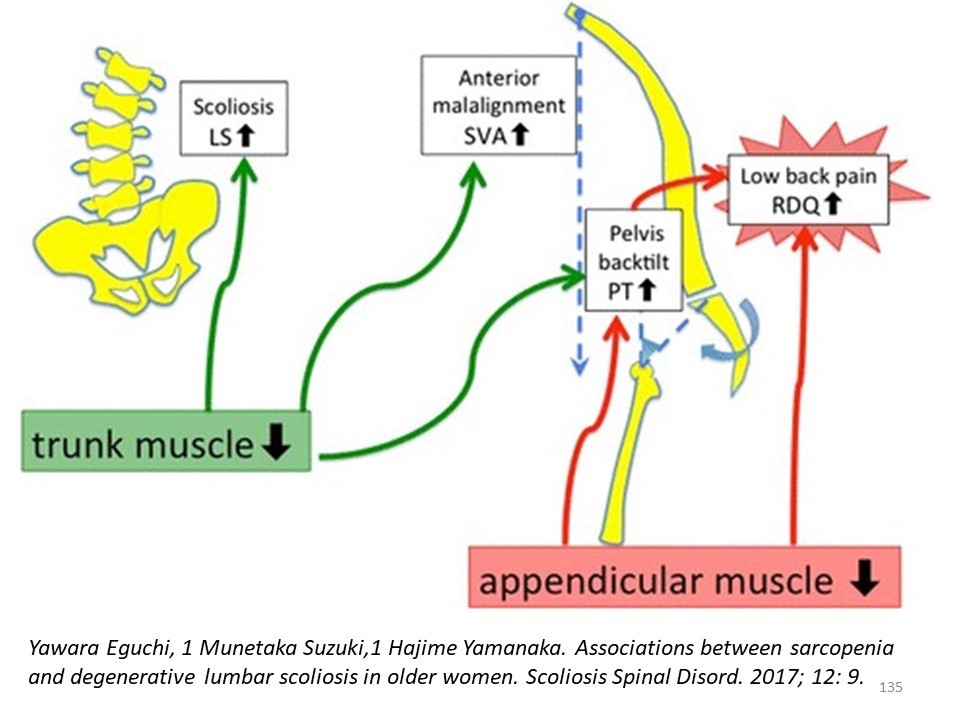 |
Each time you move away from the line of gravity, muscle tension increases. Unfortunately the sarcopenia associated with scoliosis decreases this muscular strength and the patient can no longer manage to balance. |
| |
Each time you move away from the line of gravity, muscle tension increases. Unfortunately the sarcopenia associated with scoliosis decreases this muscular strength and the patient can no longer manage to balance. |
 |
|
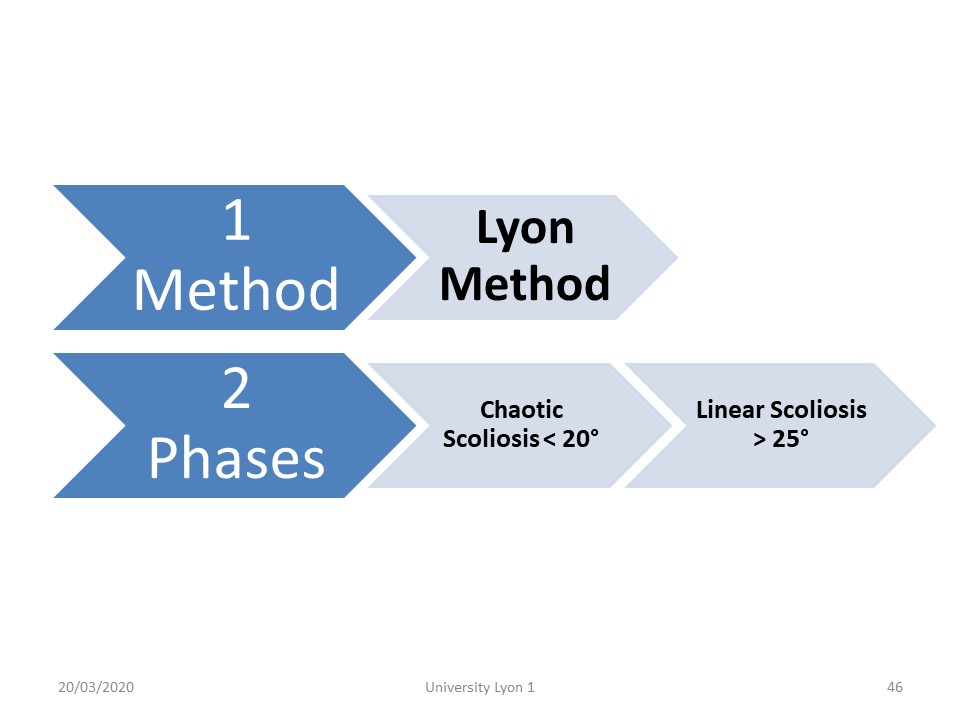 |
We have described in chaos module, the chaotic scoliosis of less than 20 °. The management is different depending on whether or not the scoliosis came into the vicious circle described by Ian Stokes. For scoliosis of more 25°, we talk about linear scoliosis, as it was initially described by Mrs. Duval-Beaupère for polio scoliosis. |
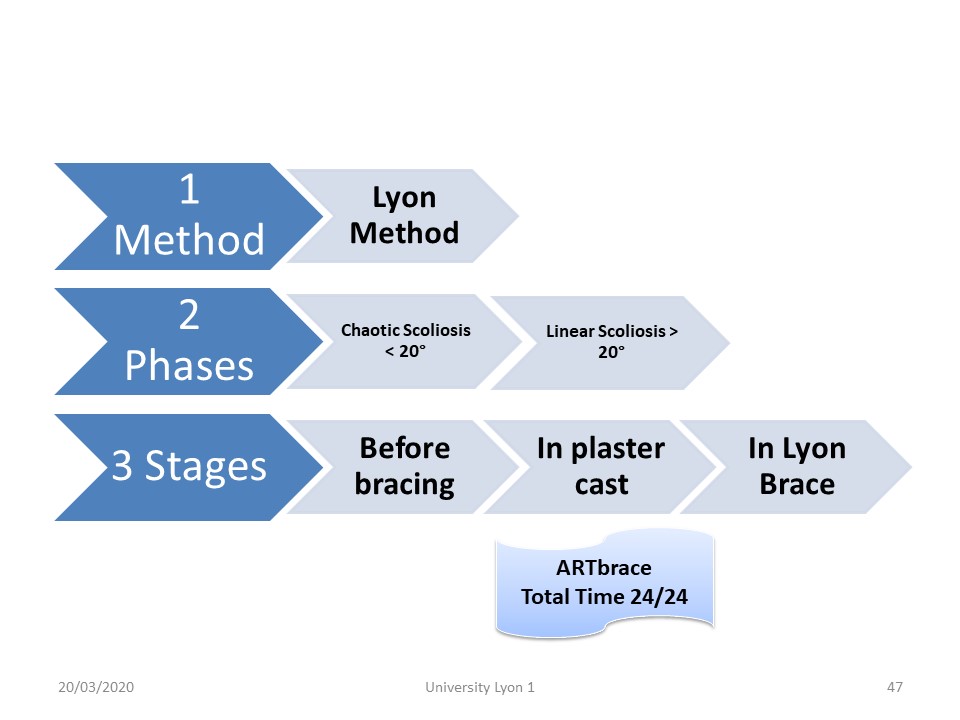 |
For pedagogical and practical reasons, we can distinguish three stages. Currently, the physiotherapist is asked to prepare the child at the 3 positions defined for the realization of the digital cast. In total time, physiotherapy is performed in the brace. |
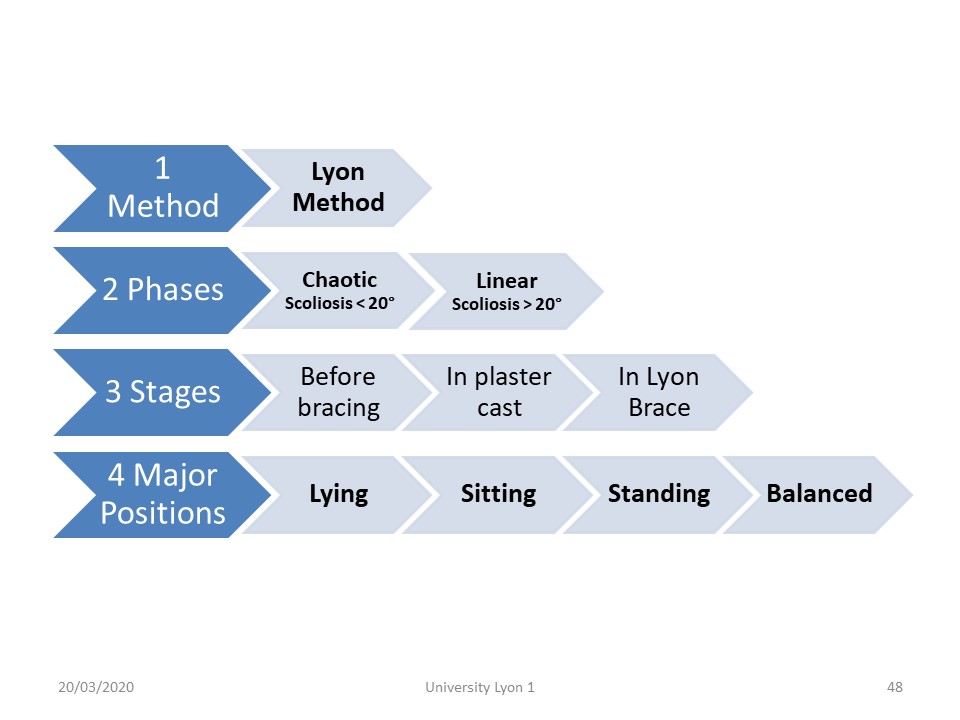 |
Physiotherapy will be gradually carried out in four positions. Lying, sitting, standing and balanced. Rolling is with the help of a Swiss ball. Balanced could be on tiliting tray, or on swiss ball. |
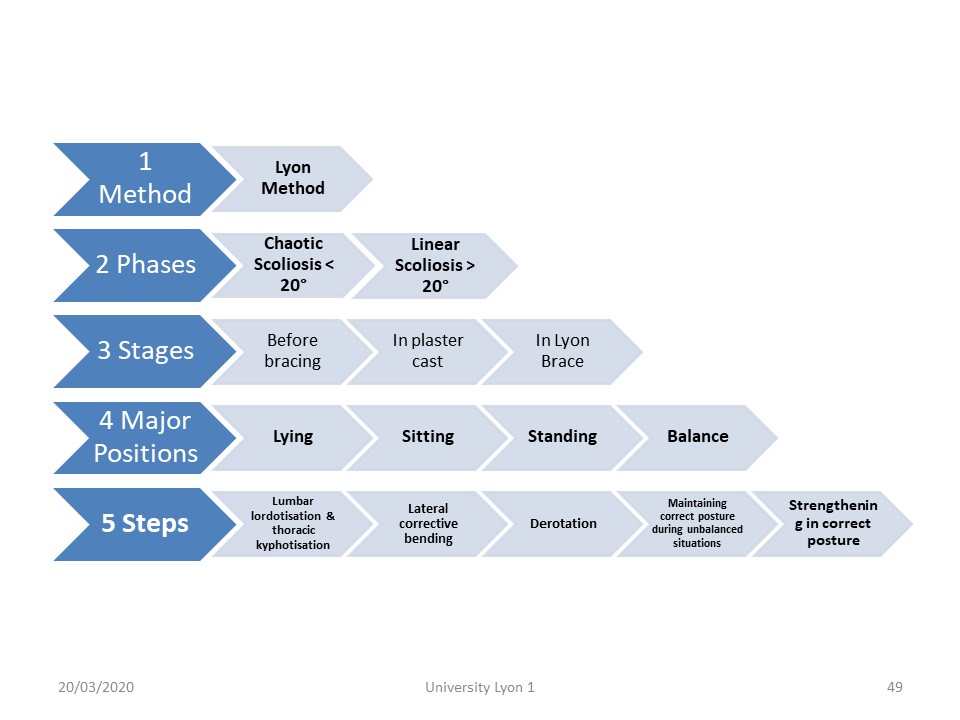 |
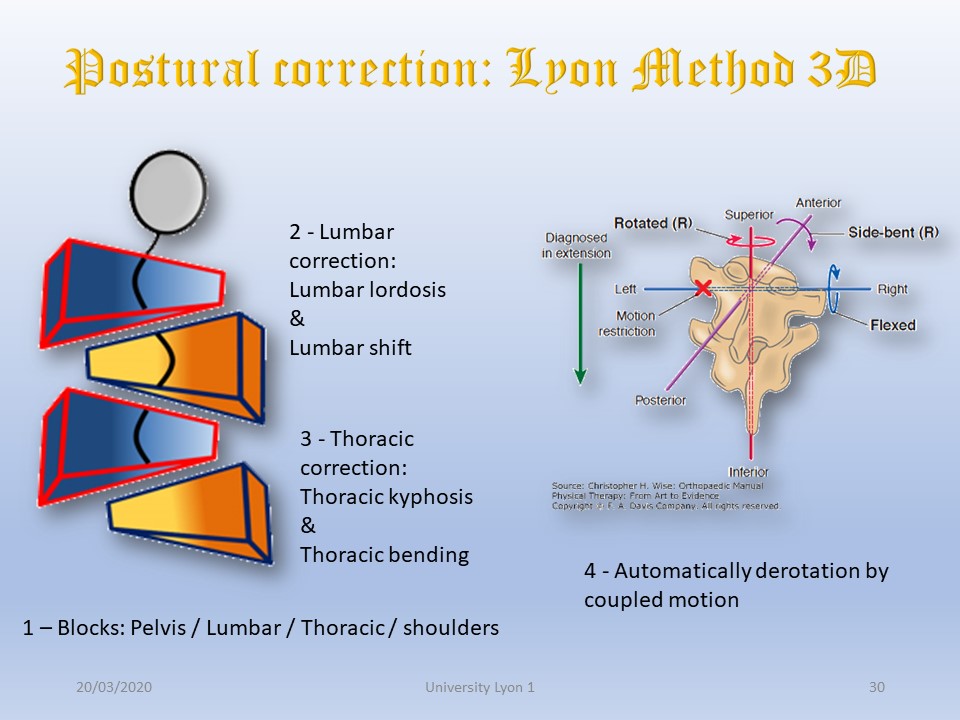
Whatever the position, we distinguish five steps: 1 – Isostatic balance in the sagittal plane 2 - Sidebending with thoracic kyphosis or shift with lumbar lordosis. 3 - The derotation is automatic under the laws of Harrison Fryette when we combine the two plans (sagittal first and then frontal). 4 - We must teach the child to maintain the position in the activities of daily life (24 hours of the back) 5 - The muscular strengthening in a corrected position is achieved first actively, and second automatically including sport activities. |
 |
Intuitively, many exercises performed once were very similar to those made today. In conclusion, the exercises of the Lyon method are very close to physiology and will thus be easily adapted to each patient and to each stage of treatment. |
 |
|
 |

